6 Lifestyle Factors To Measurably Reduce Biological Age
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Julie Gibson Clark competes on a global leaderboard of people actively fighting aging (including billionaire Bryan Johnson, who is famously very focused on such). She’s currently ahead of him on that leaderboard, so what’s she doing?
Top tips
We’ll not keep the six factors a mystery; they are:
- Exercise: her weekly exercise includes VO2 Max training, strength training, balance work, and low-intensity cardio. She exercises outdoors on Saturdays and takes rest days on Fridays and Sundays.
- Diet: she follows a 16-hour intermittent fasting schedule (eating between 09:00–17:00), consumes a clean omnivore diet with an emphasis on vegetables and adequate protein, and avoids junk food.
- Brain: she meditates for 20 minutes daily, prioritizes mental health, and ensures sufficient quality sleep, helped by morning sunlight exposure and time in nature.
- Hormesis: she engages in 20-minute sauna sessions followed by cold showers four times per week to support recovery and longevity.
- Supplements: she takes longevity supplements and bioidentical hormones to optimize her health and aging process.
- Testing: she regularly monitors her biological age and health markers through various tests, including DEXA scans, VO2 Max tests, lipid panels, and epigenetic aging clocks, allowing her to adjust her routine accordingly.
For more on all of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Age & Aging: What Can (And Can’t) We Do About It?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why Zebras Don’t Get Ulcers – by Dr. Robert M. Sapolsky

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The book does kick off with a section that didn’t age well—he talks of the stress induced globally by the Spanish Flu pandemic of 1918, and how that kind of thing just doesn’t happen any more. Today, we have much less existentially dangerous stressors!
However, the fact we went and had another pandemic really only adds weight to the general arguments of the book, rather than detracting.
We are consistently beset by “the slings and arrows of outrageous fortune” as Shakespeare would put it, and there’s a reason (or twenty) why many people go grocery-shopping with the cortisol levels of someone being hunted for sport.
So, why don’t zebras get ulcers, as they actually are hunted for food?
They don’t have rent to pay or a mortgage, they don’t have taxes, or traffic, or a broken washing machine, or a project due in the morning. Their problems come one at a time. They have a useful stress response to a stressful situation (say, being chased by lions), and when the danger is over, they go back to grazing. They have time to recover.
For us, we are (usually) not being chased by lions. But we have everything else, constantly, around the clock. So, how to fix that?
Dr. Sapolsky comprehensively describes our physiological responses to stress in quite different terms than many. By reframing stress responses as part of the homeostatic system—trying to get the body back into balance—we find a solution, or rather: ways to help our bodies recover.
The style is “pop-science” and is very accessible for the lay reader while still clearly coming from a top-level academic who is neck-deep in neuroendocrinological research. Best of both worlds!
Bottom line: if you try to take very day at a time, but sometimes several days gang up on you at once, and you’d like to learn more about what happens inside you as a result and how to fix that, this book is for you!
Click here to check out “Why Zebras Don’t Get Ulcers” and give yourself a break!
Share This Post
-

Superfood Broccoli Pesto
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cruciferous vegetables have many health benefits of their own (especially: a lot of anticancer benefits). But, it can be hard to include them in every day’s menu, so this is just one more way that’ll broaden your options! It’s delicious mixed into pasta, or served as a dip, or even on toast.
You will need
- 4 cups small broccoli florets
- 1 cup fresh basil leaves
- ½ cup pine nuts
- ¼ bulb garlic
- 3 tbsp extra virgin olive oil
- 2 tbsp nutritional yeast
- 1 tbsp lemon juice
- 2 tsp black pepper, coarse ground
- 1 tsp red pepper flakes
- ½ tsp MSG or 1 tsp low-sodium salt
Method
(we suggest you read everything at least once before doing anything)
1) Steam the broccoli for 3–5 minutes. Allow to cool.
2) Blend the pine nuts, garlic, lemon juice, and nutritional yeast.
3) Add the broccoli, basil, olive oil, black pepper, red pepper, and MSG or salt, and blend in the food processor again until well-combined.
4) Serve:

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Broccoli vs Cauliflower – Which is Healthier?
- Level-Up Your Fiber Intake! (Without Difficulty Or Discomfort)
- Herbs for (Evidence-Based) Health & Healing ← Basil features here! It’s easy to think that medicinal herbs have to be some kind of arcane obscurity, but it’s often not so.
- Our Top 5 Spices: How Much Is Enough For Benefits? ← Black pepper, red pepper, and garlic all feature here
- All About Olive Oil: Is “Extra Virgin” Worth It?
- Monosodium Glutamate: Sinless Flavor-Enhancer Or Terrible Health Risk?
Take care!
Share This Post
-

Homeopathy: Evidence So Tiny That It’s Not there?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Homeopathy: Evidence So Tiny That It’s Not There?

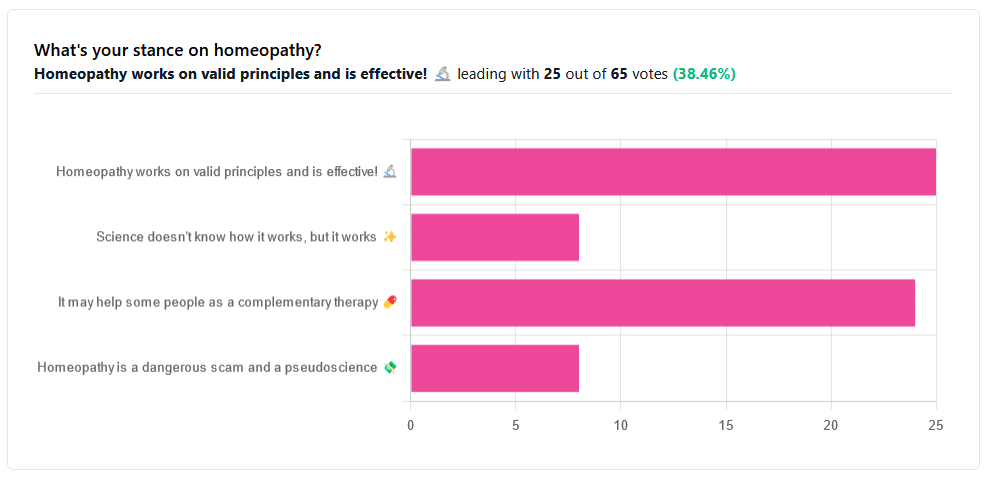
Yesterday, we asked you your opinions on homeopathy. The sample size of responses was a little lower than we usually get, but of those who did reply, there was a clear trend:
- A lot of enthusiasm for “Homeopathy works on valid principles and is effective”
- Near equal support for “It may help some people as a complementary therapy”
- Very few people voted for “Science doesn’t know how it works, but it works”; this is probably because people who considered voting for this, voted for the more flexible “It may help some people as a complementary therapy” instead.
- Very few people considered it a dangerous scam and a pseudoscience.
So, what does the science say?
Well, let us start our investigation by checking out the position of the UK’s National Health Service, an organization with a strong focus on providing the least expensive treatments that are effective.
Since homeopathy is very inexpensive to arrange, they will surely want to put it atop their list of treatments, right?
❝Homeopathy is a “treatment” based on the use of highly diluted substances, which practitioners claim can cause the body to heal itself.
There’s been extensive investigation of the effectiveness of homeopathy. There’s no good-quality evidence that homeopathy is effective as a treatment for any health condition.❞
The NHS actually has a lot more to say about that, and you can read their full statement here.
But that’s just one institution. Here’s what Australia’s National Health and Medical Research Council had to say:
❝There was no reliable evidence from research in humans that homeopathy was effective for treating the range of health conditions considered: no good-quality, well-designed studies with enough participants for a meaningful result reported either that homeopathy caused greater health improvements than placebo, or caused health improvements equal to those of another treatment❞
You can read their full statement here.
The American FDA, meanwhile, have a stronger statement:
❝Homeopathic drug products are made from a wide range of substances, including ingredients derived from plants, healthy or diseased animal or human sources, minerals and chemicals, including known poisons. These products have the potential to cause significant and even permanent harm if they are poorly manufactured, since that could lead to contaminated products or products that have potentially toxic ingredients at higher levels than are labeled and/or safe, or if they are marketed as substitute treatments for serious or life-threatening diseases and conditions, or to vulnerable populations.❞
You can read their full statement here.
Homeopathy is a dangerous scam and a pseudoscience: True or False?
False and True, respectively, mostly.
That may be a confusing answer, so let’s elaborate:
- Is it dangerous? Mostly not; it’s mostly just water. However, two possibilities for harm exist:
- Careless preparation could result in a harmful ingredient still being present in the water—and because of the “like cures like” principle, many of the ingredients used in homeopathy are harmful, ranging from heavy metals to plant-based neurotoxins. However, the process of “ultra-dilution” usually removes these so thoroughly that they are absent or otherwise scientifically undetectable.
- Placebo treatment has its place, but could result in “real” treatment going undelivered. This can cause harm if the “real” treatment was critically needed, especially if it was needed on a short timescale.
- Is it a scam? Probably mostly not; to be a scam requires malintent. Most practitioners probably believe in what they are practising.
- Is it a pseudoscience? With the exception that placebo effect has been highly studied and is a very valid complementary therapy… Yes, aside from that it is a pseudoscience. There is no scientific evidence to support homeopathy’s “like cures like” principle, and there is no scientific evidence to support homeopathy’s “water memory” idea. On the contrary, they go against the commonly understood physics of our world.
It may help some people as a complementary therapy: True or False?
True! Not only is placebo effect very well-studied, but best of all, it can still work as a placebo even if you know that you’re taking a placebo… Provided you also believe that!
Science doesn’t know how it works, but it works: True or False?
False, simply. At best, it performs as a placebo.
Placebo is most effective when it’s a remedy against subjective symptoms, like pain.
However, psychosomatic effect (the effect that our brain has on the rest of our body, to which it is very well-connected) can mean that placebo can also help against objective symptoms, like inflammation.
After all, our body, directed primarily by the brain, can “decide” what immunological defenses to deploy or hold back, for example. This is why placebo can help with conditions as diverse as arthritis (an inflammatory condition) or diabetes (an autoimmune condition, and/or a metabolic condition, depending on type).
Here’s how homeopathy measures up, for those conditions:
(the short answer is “no better than placebo”)
Homeopathy works on valid principles and is effective: True or False?
False, except insofar as placebo is a valid principle and can be effective.
The stated principles of homeopathy—”like cures like” and “water memory”—have no scientific basis.
We’d love to show the science for this, but we cannot prove a negative.
However, the ideas were conceived in 1796, and are tantamount to alchemy. A good scientific attitude means being open-minded to new ideas and testing them. In homeopathy’s case, this has been done, extensively, and more than 200 years of testing later, homeopathy has consistently performed equal to placebo.
In summary…
- If you’re enjoying homeopathic treatment and that’s working for you, great, keep at it.
- If you’re open-minded to enjoying a placebo treatment that may benefit you, be careful, but don’t let us stop you.
- If your condition is serious, please do not delay seeking evidence-based medical treatment.
Share This Post



Related Posts
-

Total Recovery – by Dr. Gary Kaplan
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, know: Dr. Kaplan is an osteopath, and as such, will be mostly approaching things from that angle. That said, he is also board certified in other things too, including family medicine, so he’s by no means a “one-trick pony”, nor are there “when your only tool is a hammer, everything starts to look like a nail” problems to be found here. Instead, the scope of the book is quite broad.
Dr. Kaplan talks us through the diagnostic process that a doctor goes through when presented with a patient, what questions need to be asked and answered—and by this we mean the deeper technical questions, e.g. “what do these symptoms have in common”, and “what mechanism was at work when the pain become chronic”, not the very basic questions asked in the initial debriefing with the patient.
He also asks such questions (and questions like these get chapters devoted to them) as “what if physical traumas build up”, and “what if physical and emotional pain influence each other”, and then examines how to interrupt the vicious cycles that lead to deterioration of one’s condition.
The style of the book is very pop-science and often narrative in its presentation, giving lots of anecdotes to illustrate the principles. It’s a “sit down and read it cover-to-cover” book—or a chapter a day, whatever your preferred pace; the point is, it’s not a “dip directly to the part that answers your immediate question” book; it’s not a textbook or manual.
Bottom line: a lot of this work is about prompting the reader to ask the right questions to get to where we need to be, but there are many illustrative possible conclusions and practical advices to be found and given too, making this a useful read if you and/or a loved one suffers from chronic pain.
Click here to check out Total Recovery, and solve your own mysteries!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Older, Faster, Stronger – by Margaret Webb
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The author, now in her 60s, made it her mission in her 50s to become the best runner she could. Before that, she’d been a keen runner previously, but let things slip rather in her 40s. But the book’s not about her 40s, it’s about her 50s and onwards, and other female runners in their 50s, 60s, 70s, 80s, and even 90s.
There’s a lot of this book that’s about people’s individual stories, and those should certainly be enough to prompt almost any reader that “if they can do it, I can”.
A lot, meanwhile, is about health and exercise science, training methods, and what has worked for various later-life athletes, including the author. So, it’s also partway instruction manual, with plenty of reference to science and medical considerations too.
Bottom line: sometimes, life throws us challenges. Sometimes, the best response is “Yeah? Bet” and surprise everyone.
Click here to check out Older, Faster, Stronger, and become all those cool things!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Better Than BMI
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
BMI is a very flawed system, and there are several more useful ways of measuring our bodies. Let’s take a look at them!
What’s wrong with BMI?
Oof, what isn’t wrong with BMI?
In short, it was developed as a demographic-based tool to specifically chart the weight-related health of working-age European white men a little under 200 years ago.
This means that if you are, perchance, not a working-age European white man in 1830 or so, then it’s not so useful. It’d be like first establishing height norms based on NBA basketball players, and then applying it to the general population, and thus coming to the conclusion that someone who is 6’2″ is very short.
In long, we did a deep-dive into it here, and in particular what things go dangerously wrong when it’s applied to women, non-white people, athletic people, pregnant people, people under 16 or over 65 and more:
When BMI Doesn’t Quite Measure Up
What we usually recommend instead
For heart disease risk and diabetes risk both, waist circumference is a much more universally reliable indicator. And since those two things tend to affect a lot of other health risks, it becomes an excellent starting point for being aware of many aspects of health.
Pregnancy will still throw off waist circumference a little (measure below the bump, not around it!), but it will nevertheless be more helpful than BMI even then, as it becomes necessary to just increase the numbers a little, according to gestational month and any confounding factors e.g. twins, triplets, etc. Ask your obstetrician about this, as it’s beyond the scope of our article today!
As to what’s considered a risk:
- Waist circumference of more than 35 inches for women
- Waist circumference of more than 40 inches for men
These numbers are considered applicable across demographics of age, ethnicity, and lifestyle.
Bonus extra measurement based on the above
Important also is waist to hip ratio.
How to calculate it:
- measure your waist circumference
- measure your hip circumference
- divide the first measurement by the second one
Because it’s a ratio, it doesn’t matter what units you use (e.g. inches, cm, etc) so long as you use the same units for both measurements.
The World Health Organization offers the following chart:
Health risk Women Men Low 0.80 or lower 0.95 or lower Moderate 0.81–0.85 0.96–1.0 High 0.86 or higher 1.1 or higher Source: Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation
This is especially relevant for cardiovascular disease risk:
…and also holds true for all-cause mortality:
Waist-Hip-Ratio as a Predictor of All-Cause Mortality in High-Functioning Older Adults
An ancient contender that’s still more useful than BMI
Remember Archimedes? The (perhaps apocryphal) story of his “Eureka” moment in the bathtub when he realized that water displacement could be used to measure the volume of an irregular shape?
Just like Archimedes (who, the story goes, had been hired to determine the composition of a crown that might or might not have been pure gold), we can use this method to determine body composition, because we have references for how much a given volume of a given substance will weigh, so combing what we know about a body’s weight and volume will tell us about its composition in ways that neither metric could give us alone.
Indeed, it’s one of the commonly-mentioned flaws of BMI that muscle weighs more than fat, and Archimedes’ method not only avoids that problem, but also, actually turns that knowledge (muscle weighs more than fat) to our advantage.
It’s called “hydrostatic weighing” now:
You may be wondering: what about bones? Or internal organs?
The fact is that those are slightly confounding factors that do get in the way of a truly accurate analysis, but the variation in how much one person’s skeleton weighs vs another’s, or one person’s set of organs weigh than another’s, is too small to make an important difference to the health implications.
Lastly…
Hydrostatic weighing isn’t the only way to work out how much of our body is made of fat; if you have for example a smart scale at home (like this one) that tells you your body fat percentage, that is an estimate based on bioelectrical impedance analysis.
It’s less accurate than the hydrostatic method, but easier to do at home!
As to what percentages are “best”, healthy body fat percentages are (assuming normal hormones) generally considered to be in the range of 20–25% for women and 15–20% for men.
You can read more about this here:
Is A Visible Six-Pack Obtainable Regardless Of Genetic Predisposition?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: