10 Tips To Reduce Morning Pain & Stiffness With Arthritis
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Physiotherapist and osteoarthritis specialist Dr. Alyssa Kuhn has professional advice:
Just the tips
We’ll not keep them a mystery; they are:
- Perform movements that target the range of motion in stiff joints, especially in knees and hips, to prevent them from being stuck in limited positions overnight.
- Use relaxation techniques like a hot shower, heating pad, or light reading before bed to reduce muscle tension and stiffness upon waking.
- Manage joint swelling during the day through gentle movement, compression sleeves, and self-massage .
- Maintain a balanced level of activity throughout the day to avoid excessive stiffness from either overactivity or, on the flipside, prolonged inactivity.
- Use pillows to support joints, such as placing one between your knees for hip and knee arthritis, and ensure you have a comfortable pillow for neck support.
- Eat anti-inflammatory foods prioritizing fruits and vegetables to reduce joint stiffness, and avoid foods high in added sugar, trans-fats, and saturated fats.
- Perform simple morning exercises targeting stiff areas to quickly relieve stiffness and ease into your daily routine.
- Engage in strength training exercises 2–3 times per week to build stronger muscles around the joints, which can reduce stiffness and pain.
- Ensure you get 7–8 hours of restful sleep, as poor sleep can increase stiffness and pain sensitivity the next day. 10almonds note: we realize there’s a degree of “catch 22” here, but we’re simply reporting her advice. Of course, do what you can to prioritize being able to get the best quality sleep you can.
- Perform gentle movements or stretches before bed to keep joints limber, focusing on exercises that feel comfortable and soothing.
For more on each of these plus some visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Avoiding/Managing Osteoarthritis
- Avoiding/Managing Rheumatoid Arthritis
- Managing Chronic Pain (Realistically!)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Detox: What’s Real, What’s Not, What’s Useful, What’s Dangerous?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
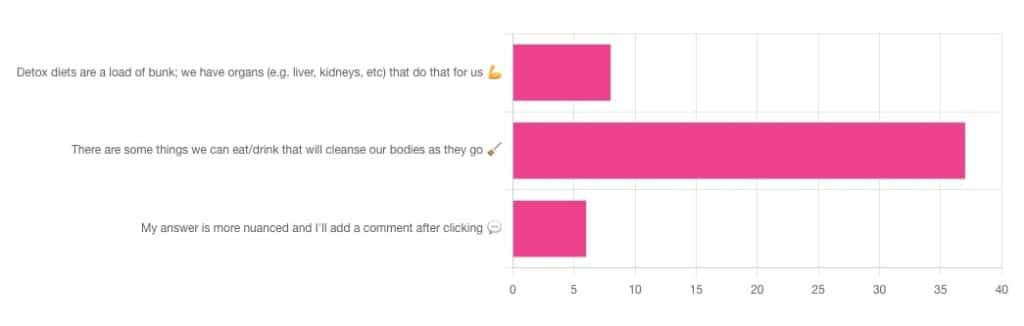
Detox: What’s Real, What’s Not, What’s Useful, What’s Dangerous?

Out of the subscribers who engaged in the poll, it looks like we have a lot of confidence in at least some detox approaches being useful!
Celery juice is most people’s go-to, and indeed it was the only one to get mentioned in the comments added. So let’s take a look at that first…
Celery juice
Celery juice is enjoyed by many people, with many health benefits in mind, including to:
- reduce inflammation
- lower blood pressure
- heal the liver
- fight cancer
- reduce bloating
- support the digestive system
- increase energy
- support weight loss
- promote good mental health
An impressive list! With such an impressive list, we would hope for an impressive weight of evidence, so regular readers might be wondering why those bullet-pointed items aren’t all shiny hyperlinks to studies backing those claims. The reason is…
There aren’t any high-quality studies that back any of those claims.
We found one case study (so, a study with a sample size of one; not amazing) that observed a blood pressure change in an elderly man after drinking celery juice.
Rather than trawl up half of PubMed to show the lacklustre results in a way more befitting of Research Review Monday, though, here’s a nice compact article detailing the litany of disappointment that is science’s observations regards celery juice:
Why Are People Juicing Their Celery? – by Allison Webster, PhD, RD
A key take-away is: juicing destroys the fiber that is celery’s biggest benefit, and its phytochemicals are largely unproven to be of use.
If you enjoy celery, great! It (when not juiced) is a great source of fiber and water. If you juice it, it’s a great source of water.
Activated Charcoal
Unlike a lot of greenery—whose “cleansing” benefits mostly come from fiber and disappear when juiced—activated charcoal has a very different way of operating.
Activated charcoal is negatively charged on a molecular level*, and that—along with its porous nature—traps toxins. It really is a superpowered detox that actually works very well indeed.
But…
It works very well indeed. It will draw out toxins so well, that it’s commonly used to treat poisonings. “Wait”, we hear you say, “why was that a but”?
It doesn’t know what a toxin is. It just draws out all of the things. You took medicine recently? Not any more you didn’t. You didn’t even take that medication orally, you took it some other way? Activated charcoal does not care:
- The effect of activated charcoal on drug exposure following intravenous administration: A meta-analysis
- Activated charcoal for acute overdose: a reappraisal
Does this mean that activated charcoal can be used to “undo” a night of heavy drinking?
Sadly not. That’s one of the few things it just doesn’t work for. It won’t work for alcohol, salts, or metals:
The Use of Activated Charcoal to Treat Intoxications
*Fun chemistry mnemonic about ions:
Cations are pussitive
Anions (by process of elimination) are negative
Onions taste good in salad (remember also: Cole’s Law)
Bottom line on detox foods/drinks:
- Fiber is great; juicing removes fiber. Eat your greens (don’t drink them)!
- Activated charcoal is the heavy artillery of detoxing
- Sometimes it will remove things you didn’t want removed, though
- It also won’t help against alcohol, sadly
Share This Post
-

Herbs For Evidence-Based Health & Healing
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Herbs have been used since prehistoric times to treat injuries and illnesses, but which ones actually work, as opposed to being “old wives’ tales”?
Even today, in pharmacies herbals products may come with a disclaimer “based on traditional use only”, which, in scientific terms, means it likely performs no better than placebo.
This is a “Saturday Life Hacks” edition, not a “Research Review Monday”, so we won’t be doing any deep-dives today, and will instead keep things short and snappy. We’ll also spotlight one main benefit, rather than trying to cover all bases, as we often have room to do on a Monday!
Basil
Helps boost immunity:
Chamomile
Significantly reduces symptoms of osteoarthritis:
(This one challenged your writer’s resolve as it does so many things, it was hard to pick just one. So, she went with one that’s less known that “settling the stomach” and “relieving PMS” and “relaxation” and so forth)
Echinacea
Significantly reduces the risk of catching a cold (but won’t help once you’ve caught it):
Echinacea for preventing and treating the common cold
Elderberry
Significantly hastens recovery from upper respiratory viral infections:
Evening Primrose
Fights neuropathy, along with many other benefits:
An updated review on pharmacological activities and phytochemical constituents of evening primrose
Fennel
Antinflammatory, along with many other benefits:
Ginkgo biloba
Antioxidant effects provide anti-aging benefits:
Advances in the Studies of Ginkgo Biloba Leaves Extract on Aging-Related Diseases
Ginseng
Combats fatigue:
Ginseng as a Treatment for Fatigue: A Systematic Review
Lavender
Enjoyed for its sedative effects, which is really does have:
Evidence for Sedative Effects of the Essential Oil of Lavender after Inhalation
Sage
Helps fight HIV type 1 and Herpes simplex type 2 (and probably other viruses, but that’s what we have the science for right now):
Aqueous extracts from peppermint, sage and lemon balm leaves display potent anti-HIV-1 activity
Valerian
Inconclusive data; “traditional use only” for restful sleep.
Can’t have everything!
Share This Post
-

What’s the difference between medical abortion and surgical abortion?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In Australia, around one in four people who are able to get pregnant will have a medical or surgical abortion in their lifetime.
Both options are safe, legal and effective. The choice between them usually comes down to personal preference and availability.
So, what’s the difference?

PeopleImages.com – Yuri A/Shutterstock What is a medical abortion?
A medical abortion involves taking two types of tablets, sold together in Australia as MS2Step.
The first tablet, mifepristone, stops the hormone progesterone, which is needed for pregnancy. This causes the lining of the uterus to break down and stops the embryo from growing.
After taking mifepristone, you wait 36–48 hours before taking the second tablet, misoprostol. Misoprostol makes the cervix (the opening of the uterus) softer and starts contractions to expel the pregnancy.
It’s normal to have strong pain and heavy bleeding with clots after taking misoprostol. Pain relief including ibuprofen and paracetamol can help.
After two to six hours, the bleeding and pain usually become like a normal period, although this may last between two to six weeks.
Haemorrhage after a medical abortion is rare (occurring in fewer than 1% of abortions). But you should seek help if bleeding remains heavy (if you soak two pads per hour for two consecutive hours) or if you have have signs of infection (such as a fever, increasing abdominal pain or smelly vaginal discharge).
Do I have to go to hospital?
It is legal to have a medical abortion outside of a hospital up to nine weeks of pregnancy.
Depending on state or territory law, the medication can be prescribed by a qualified health-care provider such as a GP, nurse practitioner or endorsed midwife. These clinicians often work in GP surgeries or sexual and reproductive health clinics and they may use telehealth.
Medical abortions also occur after nine weeks of pregnancy, but these are done in hospitals and overseen by doctors alongside nurses or midwives.
Medical abortions after 20 weeks are done by taking medications to start early labour in a maternity unit. Often, medications are first given to stop the foetal heartbeat so it is not born alive. Then, other medications are given to manage pain.
These types of abortions are very rare. They may be used when an obstacle has prevented someone accessing an abortion earlier, continuing with the pregnancy is dangerous for the pregnant person’s health or if there is a serious problem with the foetus.
Medical abortions in Australia involve taking two tablets, usually around two days apart. PeopleImages.com – Yuri A/Shutterstock What is a surgical abortion?
Surgical abortions are performed in an operating unit, usually with sedation, so you will not remember the procedure. Surgical abortions are sometimes preferred over medical abortions because they are quicker. But the decision should be between you and your health-care provider.
In the first 12–14 weeks of pregnancy, a surgical abortion takes less than 15 minutes and patients are usually discharged a few hours after the procedure.
Medications may be given before surgery to soften and open the cervix and to ease pain. During the procedure, the cervix is gently stretched open and the contents of the uterus are removed with a small tube. This procedure is carried out by trained doctors with the assistance of nurses.
Surgical abortions after 12–14 weeks are more complex and are performed by specially trained doctors. Similar to medical abortions, medications may be given first to stop the foetal heartbeat.
It is normal to experience some cramping and bleeding after a surgical abortion, which can last about two weeks. However, like medical abortion, you should seek help for heavy bleeding or signs of infection.
Do I need an ultrasound?
It used to be common before an abortion to have an ultrasound scan to check how far along the pregnancy was and to make sure it was not ectopic (outside the uterus).
However, this is no longer recommended in the early stages of pregnancy (up to 14 weeks) if it delays access to abortion. If the date of the last menstrual period is known and there are no other concerning symptoms, an ultrasound scan may not be necessary.
This means people can access medical abortion much sooner, even from the first day of a missed period, without waiting for the embryo to be big enough to be seen on an ultrasound scan. This is called “very early medical abortion”.
Before and after care
Before having an abortion, a health-care provider will explain common side effects and when to seek urgent medical attention. For people who want it, many types of contraception can be started the day of abortion.
Your health-care provider will help you understand your options, including whether you want to start contraception. PowerUp/Shutterstock Even though the success rate of medical abortion is very high (over 95%) it is routine to make sure the person is no longer pregnant.
This is usually done two to three weeks after taking the first tablet mifepristone, either by a low-sensitivity urine pregnancy test (which you can do at home) or a blood test.
In the rare case a medical abortion has not worked, a surgical abortion can be done.
Sometimes after a medical or surgical abortion, tissue is left behind in the uterus. If this happens you may need another dose of misoprostol (the second tablet) or a surgical procedure to remove the tissue.
Some people may also seek support-based counselling or peer support to help them work through the emotions that might accompany having an abortion.
Understanding the differences and similarities between medical and surgical abortions can help individuals make informed decisions about their reproductive health.
It’s important to speak with an unbiased health-care provider to discuss the best option for your circumstances and to ensure you receive the necessary follow-up care and support.
Lydia Mainey, Senior Nursing Lecturer, CQUniversity Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post




Related Posts
-
Hearty Healthy Ukrainian Borscht
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In the West, borscht is often thought of as Russian, but it is Ukrainian in origin and popular throughout much of Eastern Europe, with many local variations. Today’s borscht is a vegetarian (and vegan, depending on your choice of cooking fat) borscht from Kyiv, and it’s especially good for the gut, heart, and blood sugars.
You will need
- 1 quart vegetable stock; ideally you made this yourself from vegetable offcuts you kept in the freezer, but failing that, your supermarket should have low-sodium stock cubes
- 4 large beets, peeled and cut into matchsticks
- 1 can white beans (cannellini beans are ideal), drained and rinsed
- 1 cup sauerkraut
- 1 large onion, finely chopped
- 1 green bell pepper, roughly chopped
- 1 large russet potato, peeled and cut into large chunks
- 3 small carrots, tops removed and cut into large chunks
- 1 tbsp tomato paste
- ½ bulb garlic, finely chopped
- 2 tsp black pepper, coarse ground
- 1 bunch fresh dill, chopped. If you cannot get fresh, substitute with parsley (1 bunch fresh, chopped, or 1 tbsp dried). Do not use dried dill; it won’t work.
- A little fat for cooking; this one’s a tricky and personal decision. Butter is traditional, but would make this recipe impossible to cook without going over the recommended limit for saturated fat. Avocado oil is healthy, relatively neutral in taste, and has a high smoke point, though that latter shouldn’t be necessary here if you are attentive with the stirring. Extra virgin olive oil is also a healthy choice, but not as neutral in flavor and does have a lower smoke point. Coconut oil has arguably too strong a taste and a low smoke point. Seed oils are very heart-unhealthy. All in all, avocado oil is a respectable choice from all angles except tradition.
- On standby: a little vinegar (your preference what kind)
Salt is conspicuous by its absence, but there should be enough already from the other ingredients, especially the sauerkraut.
Method
(we suggest you read everything at least once before doing anything)
1) Heat some oil in a large sauté pan (cast iron is perfect if you have it), add the onion and pepper, and stir until the onion is becoming soft.
2) Add the carrots and beets and stir until they are becoming soft. If you need to add a little more oil, that’s fine.
3) Add the tomato paste, and stir in well.
4) Add a little (about ½ cup) of the vegetable stock and stir in well until you get a consistent texture with the tomato paste.
5) Add the sauerkraut and the rest of the broth, and cook for about 20 minutes.
6) Add the potatoes and cook for another 10 minutes.
7) Add the beans and cook for another 5 minutes.
8) Add the garlic, black pepper, and herbs. Check that everything is cooked (poke a chunk of potato with a fork) and that the seasoning is to your liking. The taste should be moderately sour from the sauerkraut; if it is sweet, you can stir in a little vinegar now to correct that.
9) Serve! Ukrainian borscht is most often served hot (unlike Lithuanian borscht, which is almost always served cold), but if the weather’s warm, it can certainly be enjoyed cold too:

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Making Friends With Your Gut (You Can Thank Us Later)
- Eat More (Of This) For Lower Blood Pressure
- No, Beetroot Isn’t Vegetable Viagra. But Here’s What It Can Do
- The Many Health Benefits Of Garlic
- Black Pepper’s Impressive Anti-Cancer Arsenal
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Bridging The Generation Gap Over The Holidays
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Often seen as a time for family connection, this same holiday period is often experienced as a time of family tension. But it doesn’t have to be that way!
Hopefully this will be of benefit to readers of all ages, but we’re going to write with the largest age-group of our readership, which is people who are most likely to have Gen-Z grandkids.
why are we writing about this?
Not only are health and happiness closely linked, and not only is mental health also just health, but… In terms of the healthy longevity secrets of the “Blue Zones”, strong intergenerational connections are usually a feature.
First, the obvious:
Any holiday tensions, of course, don’t usually start with grandkids, and are more likely amongst the adults, but some points of friction can be the same:
- Differences of opinion on political/social/economic issues
- Difference of opinion on parenting/dating choices
- Differences of opinion on life priorities
And yes, by the way, that includes even young teens (and perhaps younger) having opinions on these things—we are living in an information age, and this does mean a lot of information is a lot more accessible than it used to be, including for kids. Problems (at all ages) may occur when someone is only really exposed to views from within a certain “bias bubble”, but for better or worse, most people will have an opinion on most well-known things.
As a general rule of thumb, all of these differences of opinion can be shelved if (and only if) those involved seek to avoid conflict. And while age is no guarantee of maturity, often it’ll be the older person(s) in the strongest position to redirect things. So, have a stack of “safe” topics up your sleeve.
Bonus: you can also have non-conversational distractions up your sleeve! These may be kitchen-related, for example (time to produce something distracting, or if the nascent conflict was only between you and one other person, time to go check on something, thus removing yourself from the situation).
Next, about “family time” and technology
It can be tempting to try to have a “phones away” rule, but this will tend to only exacerbate a younger person’s withdrawal.
Better: ask (with a tone of cheerful curiosity, not accusation) about what captures their attention so. Ask about their favorite YouTubers or TikTokers or whatever it is that it is for them. Learn about that Subreddit.
Or maybe (more likely for Millennials) they were following what is going on in the world via social media, which takes on an intermediary role for the delivery of world news. Hopefully this won’t run into the differences of opinion that we mentioned up top, but it could also be a perfectly good avenue of conversation, and maybe there’s more common ground than you might expect.
Meanwhile, if you’re the older generation present, chances are your own social media use is more about the human element. That’s great, but watch out:
A common faux pas is taking pictures without asking, let alone posting them online without asking. For many people this may seem an odd thing to object to, but generationally speaking, the younger someone is (down to the upper single digits, anyway) the more likely they might feel strongly about this. So, ask first.
The reason, by the way, is that in this age of digital hypervisibility, what we choose to share online can be a deeply personal thing. And, say what you will about the pros or cons of someone carefully curating an image of how they wish to be seen, shortcutting through that for them with a candid photo posted on Facebook will not endear you to them, even if you can’t see anything wrong with the photo in question, for example.
See also: Make Social Media Work For Your Mental Health
Show an interest, but don’t interrogate
This one doesn’t take too much explanation. If people want to share about their lives, they’ll need only the smallest nudge to do so. If someone passes up an opportunity to talk about something you showed an interest in, chances are they have their own reasons for not wanting to talk about it. This might be hurtful if you feel like they’re keeping you out of their life, but the best way to get them to talk to you is just to be a good listener—not an interrogator that they have to dodge.
For some powerful tools on this, see: Listening, Better
Lastly, if things aren’t so good…
43% of people are currently experiencing some sort of familial estrangement, so if that’s you, you’re not on your own.
Sometimes, it really is too late to fix things, but sometimes it isn’t; we put together a guide that might help:
Family Estrangement & How To Fix It
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Older Americans Say They Feel Trapped in Medicare Advantage Plans
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In 2016, Richard Timmins went to a free informational seminar to learn more about Medicare coverage.
“I listened to the insurance agent and, basically, he really promoted Medicare Advantage,” Timmins said. The agent described less expensive and broader coverage offered by the plans, which are funded largely by the government but administered by private insurance companies.
For Timmins, who is now 76, it made economic sense then to sign up. And his decision was great, for a while.
Then, three years ago, he noticed a lesion on his right earlobe.
“I have a family history of melanoma. And so, I was kind of tuned in to that and thinking about that,” Timmins said of the growth, which doctors later diagnosed as malignant melanoma. “It started to grow and started to become rather painful.”
Timmins, though, discovered that his enrollment in a Premera Blue Cross Medicare Advantage plan would mean a limited network of doctors and the potential need for preapproval, or prior authorization, from the insurer before getting care. The experience, he said, made getting care more difficult, and now he wants to switch back to traditional, government-administered Medicare.
But he can’t. And he’s not alone.
“I have very little control over my actual medical care,” he said, adding that he now advises friends not to sign up for the private plans. “I think that people are not understanding what Medicare Advantage is all about.”
Enrollment in Medicare Advantage plans has grown substantially in the past few decades, enticing more than half of all eligible people, primarily those 65 or older, with low premium costs and perks like dental and vision insurance. And as the private plans’ share of the Medicare patient pie has ballooned to 30.8 million people, so too have concerns about the insurers’ aggressive sales tactics and misleading coverage claims.
Enrollees, like Timmins, who sign on when they are healthy can find themselves trapped as they grow older and sicker.
“It’s one of those things that people might like them on the front end because of their low to zero premiums and if they are getting a couple of these extra benefits — the vision, dental, that kind of thing,” said Christine Huberty, a lead benefit specialist supervising attorney for the Greater Wisconsin Agency on Aging Resources.
“But it’s when they actually need to use it for these bigger issues,” Huberty said, “that’s when people realize, ‘Oh no, this isn’t going to help me at all.’”
Medicare pays private insurers a fixed amount per Medicare Advantage enrollee and in many cases also pays out bonuses, which the insurers can use to provide supplemental benefits. Huberty said those extra benefits work as an incentive to “get people to join the plan” but that the plans then “restrict the access to so many services and coverage for the bigger stuff.”
David Meyers, assistant professor of health services, policy, and practice at the Brown University School of Public Health, analyzed a decade of Medicare Advantage enrollment and found that about 50% of beneficiaries — rural and urban — left their contract by the end of five years. Most of those enrollees switched to another Medicare Advantage plan rather than traditional Medicare.
In the study, Meyers and his co-authors muse that switching plans could be a positive sign of a free marketplace but that it could also signal “unmeasured discontent” with Medicare Advantage.
“The problem is that once you get into Medicare Advantage, if you have a couple of chronic conditions and you want to leave Medicare Advantage, even if Medicare Advantage isn’t meeting your needs, you might not have any ability to switch back to traditional Medicare,” Meyers said.
Traditional Medicare can be too expensive for beneficiaries switching back from Medicare Advantage, he said. In traditional Medicare, enrollees pay a monthly premium and, after reaching a deductible, in most cases are expected to pay 20% of the cost of each nonhospital service or item they use. And there is no limit on how much an enrollee may have to pay as part of that 20% coinsurance if they end up using a lot of care, Meyers said.
To limit what they spend out-of-pocket, traditional Medicare enrollees typically sign up for supplemental insurance, such as employer coverage or a private Medigap policy. If they are low-income, Medicaid may provide that supplemental coverage.
But, Meyers said, there’s a catch: While beneficiaries who enrolled first in traditional Medicare are guaranteed to qualify for a Medigap policy without pricing based on their medical history, Medigap insurers can deny coverage to beneficiaries transferring from Medicare Advantage plans or base their prices on medical underwriting.
Only four states — Connecticut, Maine, Massachusetts, and New York — prohibit insurers from denying a Medigap policy if the enrollee has preexisting conditions such as diabetes or heart disease.
Paul Ginsburg is a former commissioner on the Medicare Payment Advisory Commission, also known as MedPAC. It’s a legislative branch agency that advises Congress on the Medicare program. He said the inability of enrollees to easily switch between Medicare Advantage and traditional Medicare during open enrollment periods is “a real concern in our system; it shouldn’t be that way.”
The federal government offers specific enrollment periods every year for switching plans. During Medicare’s open enrollment period, from Oct. 15 to Dec. 7, enrollees can switch out of their private plans to traditional, government-administered Medicare.
Medicare Advantage enrollees can also switch plans or transfer to traditional Medicare during another open enrollment period, from Jan. 1 to March 31.
“There are a lot of people that say, ‘Hey, I’d love to come back, but I can’t get Medigap anymore, or I’ll have to just pay a lot more,’” said Ginsburg, who is now a professor of health policy at the University of Southern California.
Timmins is one of those people. The retired veterinarian lives in a rural community on Whidbey Island just north of Seattle. It’s a rugged, idyllic landscape and a popular place for second homes, hiking, and the arts. But it’s also a bit remote.
While it’s typically harder to find doctors in rural areas, Timmins said he believes his Premera Blue Cross plan made it more challenging to get care for a variety of reasons, including the difficulty of finding and getting in to see specialists.
Nearly half of Medicare Advantage plan directories contained inaccurate information on what providers were available, according to the most recent federal review. Beginning in 2024, new or expanding Medicare Advantage plans must demonstrate compliance with federal network expectations or their applications could be denied.
Amanda Lansford, a Premera Blue Cross spokesperson, declined to comment on Timmins’ case. She said the plan meets federal network adequacy requirements as well as travel time and distance standards “to ensure members are not experiencing undue burdens when seeking care.”
Traditional Medicare allows beneficiaries to go to nearly any doctor or hospital in the U.S., and in most cases enrollees do not need approval to get services.
Timmins, who recently finished immunotherapy, said he doesn’t think he would be approved for a Medigap policy, “because of my health issue.” And if he were to get into one, Timmins said, it would likely be too expensive.
For now, Timmins said, he is staying with his Medicare Advantage plan.
“I’m getting older. More stuff is going to happen.”
There is also a chance, Timmins said, that his cancer could resurface: “I’m very aware of my mortality.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: