Why is migraine more common in women than men?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve known for a long time that women are more likely than men to have migraine attacks.
As children, girls and boys experience migraine equally. But after puberty, women are two to three times more likely to experience this potentially debilitating condition.
Recently, an Australian study showed it may be even more common than we previously thought – as many as one in three women live with migraine.
For comparison, migraine affects roughly one in 15 men in Australia.
So, what’s behind the difference? Here’s what we know.
More than a headache
Migraine is not just a bad headache – it is a complex disorder that causes the brain to process sensory information abnormally.
This means “migraine brains” can have difficulty processing information from any of the five senses:
- sight (leading to problems with light sensitivity and glare)
- sound (leading to noise sensitivity)
- smell (certain smells can trigger headaches)
- touch (leading to face or scalp tenderness)
- taste (causing distorted taste, nausea and vomiting).
Migraine attacks typically last anywhere from four hours to three days – but can be longer.
In addition to the symptoms above, attacks can include throbbing head pain, dizziness, fatigue and difficulty concentrating. It is these extra symptoms that help diagnose migraine – not the location of head pain or pain severity.
Why are attacks more frequent in women?
Puberty is when the difference between men and women emerges. This is when our bodies massively increase the production of sex hormones.
People are often surprised to learn that both men and women produce oestrogen, progesterone and testosterone. Testosterone levels are higher in men, whereas women have higher levels of oestrogen and progesterone.
However, it is not just the type of hormone that makes a difference, but the way they fluctuate over time.
For many women, there are certain “milestone moments” when their migraine tends to worsen due to hormonal fluctuations – puberty, menstruation, pregnancy and perimenopause (the lead-up to your final period).
For example, some women notice migraine flare-ups every month, linked to phases in their monthly menstrual cycle when oestrogen levels drop.
They might even be able to predict when their period will start, as migraine attacks typically start a few days before the bleeding.
How hormones affect the brain
Women with migraine can be more sensitive to hormonal changes. This is particularly the case for sudden decreases in oestrogen. But even more subtle changes to hormone levels can cause migraine attacks.
These hormonal changes can activate brain processes that trigger migraine, such as cortical spreading depression. This is a very slow wave of electrical activity that spreads in the brain, causing some areas to function more slowly than others after it passes.
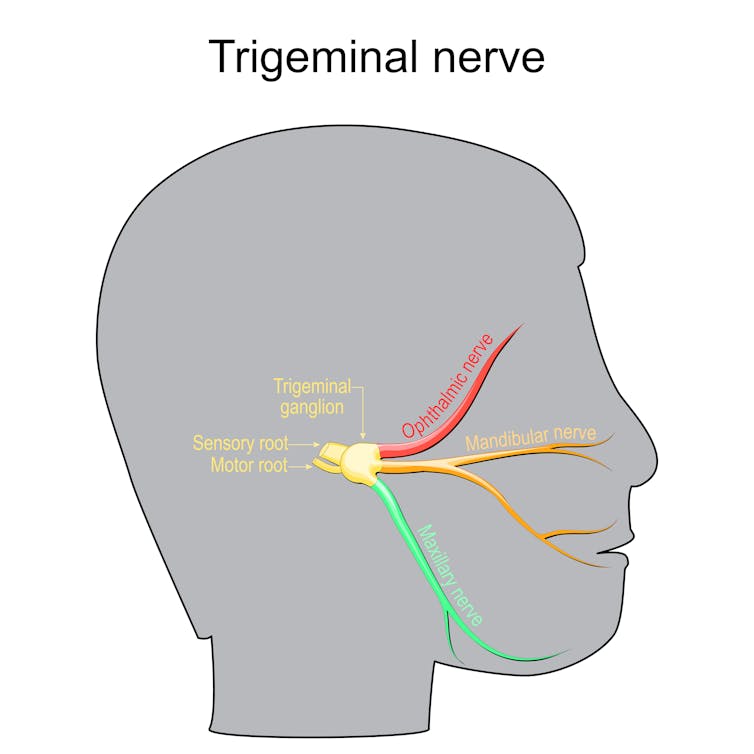
Decrease in oestrogen can also affect how we receive and process information through the trigeminal nerve. This plays a key role in the onset and maintenance of migraine pain.
All kinds of fluctuations can be a trigger
Pregnancy can often destabilise migraine again and make attacks more likely, even when someone has previously enjoyed a period of good migraine control.
Migraine symptoms often become uncontrolled in the first trimester in particular, due to rapid hormonal changes needed to sustain a pregnancy. This usually settles in the second and third trimesters, when hormonal changes stabilise.
However, giving birth is yet another change.
Towards the end of pregnancy, oestrogen levels can be 30 times higher than pre-pregnancy levels, and progesterone can be 20 times higher. When these hormones plummet back to normal after giving birth, migraine attacks can often sharply worsen again.
Perimenopause can also involve random surges of oestrogen from the dwindling supplies of eggs within the ovaries – which previously produced these hormones cyclically and in abundance. This irregular hormone production can cause random spikes in migraine attacks. It can be extra challenging when combined with other symptoms of menopause such as hot flushes or mood changes.
Hormonal contraceptives and menopause hormone therapy can also affect migraine control. Sometimes, supplementing hormones at a regular, steady daily dose can help manage the hormone-sensitive headaches and other symptoms. However, for others, adding extra hormones can cause head pain to flare up.
Does migraine run in the family?
Genes also play a role. It’s not a coincidence that migraine is passed down in families through the maternal side.
This is because mothers pass on mitochondria to children (while fathers do not). Mitochondria are parts inside the cell that control energy.
People with migraine have fewer functional enzymes within their mitochondria, meaning their brains are in an energy-deficient state. This worsens with migraine attacks as there is even more stress to the system.
This is also why extra stress (such as sleep deprivation, missed meals, or emotional stress) can trigger a migraine and worsen pain.
There is also a strong link between migraine in women and anxiety and depression – conditions women are more likely to develop in response to stressful life events.
Knowing your own patterns
If you suspect hormones may be affecting your migraine attacks, it is helpful to keep a diary of symptoms, including headaches. Mark each day per month where you get migraine symptoms, as well as your period, to find patterns.
Identifying patterns in pain flares helps doctors guide you to a personalised medication plan, which may include hormone therapies or non-hormonal therapies.
Lakshini Gunasekera, PhD Candidate in Neurology, Monash University; Caroline Gurvich, Associate Professor and Clinical Neuropsychologist, Monash University; Eveline Mu, Research Fellow in Women’s Mental Health, Monash University, and Jayashri Kulkarni, Professor of Psychiatry, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Secret Behind Losing Inches, Not Weight

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Ignore the numbers on the scale” turns out to be good advice:
What matters more for the health
Taken at face value, the numbers on the scale represent nothing more nor less than your relationship with gravity.
On a more complex level, weight reflects muscle, fat, water, hormonal fluctuations, food*, stress, and sleep, so the number can stay the same while your body shrinks.
*Literally, the food itself, not the consequences. Let’s put it this way: if you eat an entire cabbage, then you’re not going to “put on weight” from it, but nevertheless, the mass of the cabbage is inside you right now and the scale will reflect that.
As you probably know, muscle weighs more than fat, so if you gain the former and lose the latter, you can look leaner at the same weight. In other words, losing inches without losing weight means body recomposition is happening and your body is probably doing well, all else being equal. This also means that you can see progress sooner than the scale would tell you, by taking measurements and noting how your clothes fit.
A common mistake that many people make when trying to “lose weight” is cutting calories and adding cardio, but that usually breaks down muscle and slows long-term fat loss, rather than hastening it.
A three-step process that’s better:
- Set your intentions by replacing restricting and overtraining with fueling well, training with purpose, and recovering intentionally too
- Add protein, nutrient diversity, water, and energizing whole foods that contain plenty of fiber
- Strengthen by focusing on strength training and progressive overload, which outperforms cardio for long-term fat burning
Some myths to not fall for:
- The muscle and fat myth: muscle does not turn into fat; losing muscle lowers daily burn and increases fat storage
- The menopause myth: you can build muscle during menopause by adjusting training, protein intake, and recovery
- The cardio myth: cardio burns energy briefly, but muscle burns energy all day and thus has a bigger long-term impact
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Can You Gain Muscle & Lose Fat At The Same Time?
Take care!
Share This Post
-
5 Things To Know About Passive Suicidal Ideation
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you’ve ever wanted to go to sleep and never wake up, or have some accident/incident/illness take you with no action on your part, or a loved one has ever expressed such thoughts/feelings to you… Then this video is for you. Dr. Scott Eilers explains:
Tired of living
We’ll not keep them a mystery; here are the five things that Dr. Eilers wants us to know about passive suicidal ideation:
- What it is: a desire for something to end your life without taking active steps. While it may seem all too common, it’s not necessarily inevitable or unchangeable.
- What it means in terms of severity: it isn’t a clear indicator of how severe someone’s depression is. It doesn’t necessarily mean that the person’s depression is mild; it can be severe even without active suicidal thoughts, or indeed, suicidality at all.
- What it threatens: although passive suicidal ideation doesn’t usually involve active planning, it can still be dangerous. Over time, it can evolve into active suicidal ideation or lead to risky behaviors.
- What it isn’t: passive suicidal ideation is different from intrusive thoughts, which are unwanted, distressing thoughts about death. The former involves a desire for death, while the latter does not.
- What it doesn’t have to be: passive suicidal ideation is often a symptom of underlying depression or a mood disorder, which can be treated through therapy, medication, or a combination of both. Seeking treatment is crucial and can be life-changing.
For more on all of the above, here’s Dr. Eilers with his own words:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- The Mental Health First Aid You’ll Hopefully Never Need ← about depression generally
- How To Stay Alive (When You Really Don’t Want To) ← about suicidality specifically
Take care!
Share This Post
-
Radiation-Eating, Mind Control, & Other Secret Superpowers Of Fungi
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Fungi are more closely related to animals than to plants, though in truth they are neither, and cannot be killed in a way that matters:
Decay exists as an extant form of life
The fungal kingdom ranges from athlete’s foot to mushrooms to the underground mycorrhizal network that allows trees to communicate with each other and share nutrients.
About that last one… Yes, really! Many plants depend on mycorrhizal fungi, which exchange soil nutrients such as phosphorus and nitrogen for carbon produced by plants, as ectomycorrhizal fungi surround roots, while arbuscular mycorrhizal fungi penetrate root cells to facilitate nutrient exchange. This symbiosis also means that when it comes to knowing* what’s happening, the fungus functions as though part of the plant, meaning that if more than one plant is connected to the same mycorrhizal network (as is almost always the case in the wild), then each plant has the same information as the entire network.
*Without getting too sidetracked, we’ll quickly mention that despite not having brains, yes, plants do process information, using various kinds of chemical signalling similar to animals’ use of hormones and pheromones, electrical signalling, and more. And yes, that includes sensory information, because plants are very receptive to light and dark, and thus can (to varying degrees) “see”. Perhaps the most clear example of this is Boquila trifoliolata, a plant known for mimicking the appearance of nearby plants. Researchers got curious (as researchers do), and placed one next to a plastic plant (so: no mycorrhizal or otherwise chemical signalling can be happening), and yes, it mimicked the leaf shape and color of the artificial plant that it evidently could indeed see. Fun stuff!
You can read more about that one here, if you’re interested: Boquila trifoliolata mimics leaves of an artificial plastic host plant
Now, back to fungi:
Fungi were once classified as plants because many grow from the soil on branching, root-like networks, but they differ fundamentally in biology, for example:
- Most people know that unlike plants, fungi don’t use sunlight for energy but instead decompose organic matter or obtain nutrients from living organisms.
- Most people don’t know that fungal cell walls are made of chitin (the same material found in the exoskeletons of insects, arachnids, and the like) rather than cellulose as in plants.
On which note, yes, many fungi produce compounds including antibiotics, toxins, and psychedelic chemicals to defend themselves, exploit other organisms, or manipulate their surroundings, including:
- Altering minds: mushrooms in the Psilocybe genus produce psilocybin, which binds to serotonin receptors and causes hallucinations in humans, though it likely evolved to discourage grazing by slugs and snails.
- Zombifying ants: many Cordyceps fungi infect ants, alter their nervous systems and muscles, compel them to climb to elevated locations, and then release millions of spores from their bodies.
- Eating radiation: some fungi thrive in harsh environments, including the radioactive ruins of Chernobyl nuclear power plant, where at least 37 fungal species have been identified, and studies aboard the International Space Station found that fungi such as Cryptococcus neoformans can convert absorbed gamma radiation into usable energy.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
The Magic Of Mushrooms: “The Longevity Vitamin” (That’s Not A Vitamin) ← about ergothioneine, of which mushrooms are an excellent source
What kind of mushrooms? All kinds, but please stick to non-poisonous ones!
Take care!
Share This Post

-
Tooth Remineralization: How To Heal Your Teeth Naturally
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Michelle Jorgensen, dentist, explains:
The bare-bones details:
Teeth cannot be regrown (yet!) but can be remineralized, which simply involves restoring lost minerals. When we’re talking about health, “minerals” is usually used to mean elemental minerals, like calcium, magnesium, phosphorus, etc, but the specific mineral that’s needed here is hydroxyapatite (a calcium phosphate mineral, the same as is found in bones).
Not only can acids from food and bacteria dissolve the minerals from the teeth, but also, the body itself may extract minerals from the teeth if it needs them for other functions it considers more critical and/or more urgent.
Cavities occur when acids create porous holes in teeth by dissolving minerals, which allows bacteria to invade, which means more acid, and cavities.
Remineralization can be achieved by doing the following things:
- Use hydroxyapatite-based products (tooth powder, mouthwash).
- Improve gut health to ensure proper mineral absorption.
- Reduce acidic food and drink intake.
- Maintain good oral hygiene to prevent bacteria build-up.
- Eat foods rich in vitamins A, D, E, and K, which help direct minerals to teeth and bones.
For more on all of the above, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Less Common Oral Hygiene Options
- Fluoride Toothpaste vs Non-Fluoride Toothpaste – Which is Healthier?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
3 Tweaks To Cut Diabetes Risk By 1/3
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Today, the research we’ll be highlighting builds on the Mediterranean diet, by adding some extra interventions. We’ve written before about the Mediterranean diet, here:
The Mediterranean Diet: What Is It Good For? ← What isn’t it good for?
The Mediterranean diet’s strengths come from various factors including its good plant:animal ratio (leaning heavily on the plants), colorful fruit and veg minimally processed, and the fact that olive oil is the main source of fat:
All About Olive Oil ← pretty much one of the healthiest fats we can consume, if not healthiest all-rounder fat.
This is not the first time we’ve talked about making the Mediterranean even better; see: Four Ways To Upgrade The Mediterranean Diet ← to make it even more anti-inflammatory, even more gut-healthy, even more heart-healthy, and even more brain-healthy, respectively.
Med+
Researchers (Dr. Dolores Corella et al.) wanted to know the effectiveness of adding further interventions on top of the already-healthy Mediterranean diet.
Specifically, the Mediterranean diet, plus:
- Caloric restriction (600 fewer calories per day)
- Moderate exercise (brisk walking, strength, balance)
- Professional weight-loss support
On which note, the study participants were 4,746 adults (ages 55–75) categorized as overweight or obese, with metabolic syndrome but no diabetes at baseline, followed for six years.
With this in mind, the method may not be applicable to all people—if you are already exercising moderately, do not have extra weight to healthily lose, and are eating maintenance calories only, then cutting your caloric intake drastically will probably not be healthy or sustainable.
For more on the science of caloric restriction (including the pros and cons), see: Is Cutting Calories The Key To Healthy Long Life?
As for the study, the intervention group (Mediterranean diet plus those three things) and the control group (Mediterranean diet only) saw the following results after 6 years:
- Intervention group lost 3.3kg (7¼ lbs); control group lost 0.6kg (1⅓ lbs)
- Intervention group lost 3.6cm (1½ inches) waist circumference; control group lost 0.3cm (⅛ inch)
- Intervention group had 9.5% absolute risk of diabetes; control group had 12% risk
The overall reduction of diabetes incidence, however, was 31% lower for the intervention group than the control group
You may be wondering: since 9.5 is about 21% (not 31%) of 12, where did the 31% figure come from?
And the answer is: this is one of those places where absolute risk reduction, relative risk reduction, and hazard ratio-based incidence reduction get easily mixed up:
- Absolute risk reduction (ARR) = we take the cumulative risk in control and subtract the cumulative risk in intervention, so here, that’s 12.0% – 9.5% = 2.5 percentage points ARR
- Relative risk reduction (RRR) = we take the ARR we just calculated, and subtract the cumulative risk in control, so here, that’s 2.5/12 = 20.8% RRR
- Hazard ratio-based incidence reduction = what happens if we apply the resultant hazard ratio to person-years, i.e. instead of of looking at just those 6 years (and not caring if someone gets diabetes in 7 years, say), we take each participant’s 6 years and stretch them all end-to-end, so that we can see more accurately what incidence rate will be over more time. We then take the number of person-years generated (in this case, 6 years x 4746 people = 28,476 person-years, which is a lot of data), look at the reduction rate, and then scale it back down (keeping the same ratio) to a number that makes for a clearer representation that’s easy to apply to other models, in this case, 1,000 person years, using the same hazard ratio as we found from the 28,476 person-years. The result of this calculation, in this case, is a 31% lower incidence rate. This is more or less what we might reasonably have expected from a glance at the data—we could expect that it would be higher than the RRR, because this time we get to factor into the equation the people who will get diabetes in year 7, year 8, year 9, etc, from only a 6-year study, because of how we laid everyone’s 6 years end-to-end.
You can find the paper itself, here: Comparison of an Energy-Reduced Mediterranean Diet and Physical Activity Versus an Ad Libitum Mediterranean Diet in the Prevention of Type 2 Diabetes
Is it worth it?
If you have those 7¼ lbs and 1½ inches to lose, then a 31% reduction in diabetes risk is a big benefit.
If, on the other hand, you don’t, then as we say, probably skipping 600kcal per day is not so good an idea for you.
For everyone, meanwhile, moderate exercise is of course great.
As for the professional weight loss help? Well, that depends on the nature of the help, and this study didn’t separate its effects (if any) from the effects of the caloric reduction and moderate exercise. So, honestly we think it’s unhelpful that they included it with doing a separate control for it.
Want to reduce diabetes risk without reducing calories?
Check out:
How To Prevent And Reverse Type 2 Diabetes: Turn Back The Clock On Insulin Resistance!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Death by Sitting – by Carolyne Thompson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You may be wondering: is this a lot of words to say “sit down less”?
And the answer is: there’s a lot more in here than that. Of course, yes, “sit down less” is an important take-away, but there’s a lot about the specific problems caused by sitting in chairs, the health risks are that are increased and how, and the early warning signs to watch out for.
After these chapters of woe, most of the book is given over to solutions; about taking standing and walking breaks, tying movement to productivity, why exercise alone is not enough to offset the damage of sitting, relearning ergonomic posture in the context of mitigating the harm, psychological shifts to break the habit of sitting, redefining social norms around sitting and socializing, rewiring one’s body and retraining better movements as well as postures to always immediately move out of if one finds oneself in, and much much more.
The style is light and easy to read, while still including scientific research as appropriate along with practical, actionable advice.
Bottom line: if you’d like to do better for your body than slowly killing it for however many hours a day, then this book has a wealth of advice far beyond the obvious (but important!) “sit less”.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: