What is myasthenia gravis, the rare disease tennis great Monica Seles lives with?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Former tennis star Monica Seles recently revealed she is living with the rare disease myasthenia gravis, which affects 12 in 100,000 people globally.
Seles explained her first symptoms appeared suddenly around three years ago. She began experiencing double vision and weakness in her arms and legs. This made everyday activities, such as drying her hair, a challenge.

So what is this condition?
Myasthenia gravis is a chronic autoimmune disorder, where your own immune system disrupts the communication between nerves and skeletal muscle.
In healthy people, nerve cells send a chemical messenger called acetylcholine. This tells muscles to contract by binding to its receptor.
In myasthenia gravis, antibodies block or destroy these receptors, so the signal is weakened or lost.
The result is muscle weakness that worsens with activity and improves with rest. This is called “fatigueability”.
What are the symptoms?
Muscle weakness can affect everyday functions such as walking, speaking, breathing and swallowing.
Symptoms, which can appear suddenly, may also affect the eyes, causing drooping eyelids and double vision.
In some cases, weakness of the muscles makes it difficult to breathe or can result in choking on food or water. This is called a “myasthenic crisis” and requires hospitalisation and sometimes life support.
In our research interviews, a young woman in her 30s living with myasthenia gravis described what it feels like to experience a crisis:
My speech slows, and I sound like I’m drunk, even though I’m fighting to breathe. Sometimes I can’t talk at all. Having my mum there to advocate for me has been life-saving, because I can’t explain what’s happening. Staying calm helps me cope.
Another man in his 70s explained just how suddenly the disease can appear:
It came on at my 70th birthday party. I developed ocular MG [a form of myasthenia gravis affecting the eyes] in the middle of my speech, and my grown children thought I was having a stroke. They rushed me to hospital – and that’s how it all began.
What causes it and who does it affect?
It’s unclear what causes the disease but it’s not thought to be hereditary.
There is some evidence it is more likely to occur with other autoimmune conditions such as autoimmune thyroid disease, lupus and rheumatoid arthritis but the evidence remains incomplete.
Myasthenia gravis can appear at any age. Early onset is more common in women (often before 40), while men are more likely to develop myasthenia gravis later in life.
How is it diagnosed?
Despite its serious impact, myasthenia gravis remains under-recognised and is difficult to diagnose. The diagnosis is “clinical”, which requires a doctor with experience in myasthenia gravis to make a judgement, based on the information available.
A handful of tests are available to support the diagnosis: blood tests for antibodies, nerve conduction studies and needle electromyography, which record the electrical activity of nerves and muscles. But these are far from perfect in establishing the diagnosis.
How is it treated?
There is currently no cure for myasthenia gravis, but a range of treatments can help manage symptoms. These include:
- oral medicines called anticholinesterase inhibitors, which temporarily improve communication between nerves and muscles
- immunosuppressant medications, which are generally taken by mouth. These dampen the immune system and reduce its attack
- plasma exchange and intravenous immunoglobulin (IVIg), which is a blood product. These are resource-intensive therapies that remove or block the harmful antibodies. These treatments require hospital admission for at least half a day to administer via an intravenous drip
- in some patients, surgery is performed to remove the thymus gland, which is located in the chest between the lungs. This plays a key role in the abnormal immune response in people with myasthenia gravis.
While most treatments are subsidised through the health system, access remains a challenge for some people. Plasma exchange and IVIg are not available in all hospitals, for example, meaning patients in regional areas may face long travel distances or delays in receiving urgent care.
What is the long-term outlook?
While myasthenic crises are life-threatening, the evidence so far suggests the disease won’t have a significant impact on life expectancy for most people. Treatments aim to reduce disease activity rather than offering a complete cure.
People with myasthenia gravis can have very different journeys with their disease. Some may need frequent hospital admissions, and around 10% have a form of disease which is difficult to treat.
Others may experience minimal symptoms requiring little to no treatment.
Many find their symptoms are unpredictable. As a woman in her 60s, who has had myasthenia gravis for ten years, told us:
I think you just get used to managing – to finding your own rhythm in all the uncertainty.
Gozde Aydin, Research Fellow, Centre for Health Economics, Monash University and Yong Lin Wang, Neurologist and Phd Candidate, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Skincare – by Caroline Hirons

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our skin is our largest organ, and it affects (and is affected by) most of what it contains. In other words, us.
So how do we look after this organ? Caroline Hirons lays it bare for us, in this very clear (and well-illustrated with many photos) book that gives a ground-upwards explanation of:
- Our skin’s layers and features and what they do
- The many ways our skin can be different from others
- What lifestyle factors to worry about (or not)
- What exactly the many kinds of skincare products do
- How to understand which ones are actually for our skin
- How to craft the ideal skincare routine for any individual
- What should go into a personalized skincare kit
Because, as it turns out, shockingly we can’t trust advertising. Not only is it advertising, but also, they don’t know us. What will be perfect for one person’s skin may ruin another’s, and labels can be very misleading.
A strength of this book is how Hirons demystifies all that, so we can ignore the claims and just know what a product will actually do, from its ingredients.
She also covers the changes that occur in various life processes, including puberty, pregnancy, menopause, and just plain aging. In other words, what to do when what’s been working suddenly doesn’t anymore.
Bottom line: this is a great book for anyone (though: especially those of us with female hormones) who wants to understand the skin you’re in and how to keep it well-nourished and glowingly healthy.
Click here to check out “Skincare” and take good care of yourself!
Share This Post
-

How To Keep Warm (Without Sweat Patches!)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝I saw an advert on the subway for a pillow spray that guarantees a perfect night’s sleep. What does the science say about smells/sleep?❞
That is certainly a bold claim! Unless it’s contingent, e.g. “…or your money back”. Because otherwise, it absolutely cannot guarantee that.
There is some merit:
❝Odors can modulate the latency to sleep onset, as well as the quality and duration of sleep. Olfactory modulation of sleep may be mediated by direct synaptic interaction between the olfactory system and sleep control nuclei, and/or indirectly through odor modulation of arousal and respiration.
Such modulation appears most heavily influenced by past associations and expectations about the odor, beyond any potential direct physicochemical effect❞
Source: Reciprocal relationships between sleep and smell
Translating that from sciencese:
Sometimes we find pleasant smells relaxing, and placebo effect also helps.
That “any potential direct physiochemical effect”, though, when it does occur, is things like this…
Read: Odor blocking of stress hormone responses
…but that’s a mouse study, and those odors may only work to block three specific mouse stress responses to three specific stressors: physical restraint, predator odor, and male–male confrontation.
In other words: if, perchance, those three things are not what’s stressing you in bed at night (we won’t make assumptions), and/or you are not a mouse, it may not help.
(and this, dear readers, is why we must read articles, and not just headlines!)
But! If you are going to go for a pillow fragrance, something well-associated with being relaxing and soporific, such as lavender, is the way to go:
- Effects of aromatherapy on sleep quality and anxiety of patients
- Effects of Aromatherapy on the Anxiety, Vital Signs, and Sleep Quality of Percutaneous Coronary Intervention Patients in Intensive Care Units
- Effect of lavender aromatherapy on vital signs and perceived quality of sleep in the intermediate care unit: a pilot study
tl;dr = patients found lavender fragrances relaxing, experienced less anxiety, got better sleep (significantly or insignificantly, depending on the study) and enjoyed lower blood pressure (significantly or insignificantly, depending on the study).
PS: this writer uses a pillow spray like this one
Enjoy!
Share This Post
-

If you’re worried about inflammation, stop stressing about seed oils and focus on the basics
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You’ve probably seen recent claims online seed oils are “toxic” and cause inflammation, cancer, diabetes and heart disease. But what does the research say?
Overall, if you’re worried about inflammation, cancer, diabetes and heart disease there are probably more important things to worry about than seed oils.
They may or may not play a role in inflammation (the research picture is mixed). What we do know, however, is that a high-quality diet rich in unprocessed whole foods (fruits, vegetables, nuts, seeds, grains and lean meats) is the number one thing you can to do reduce inflammation and your risk of developing diseases.
Rather than focusing on seed oils specifically, reduce your intake of processed foods more broadly and focus on eating fresh foods. So don’t stress out too much about using a bit of seed oils in your cooking if you are generally focused on all the right things.
What are seed oils?
Seed oils are made from whole seeds, such as sunflower seeds, flax seeds, chia seeds and sesame seeds. These seeds are processed to extract oil.
The most common seed oils found at grocery stores include sesame oil, canola oil, sunflower oil, flaxseed oil, corn oil, grapeseed oil and soybean oil.
Seed oils are generally affordable, easy to find and suitable for many dishes and cuisines as they often have a high smoke point.
However, most people consume seed oils in larger amounts through processed foods such as biscuits, cakes, chips, muesli bars, muffins, dipping sauces, deep-fried foods, salad dressings and margarines.
These processed foods are “discretionary”, meaning they’re OK to have occasionally. But they are not considered necessary for a healthy diet, nor recommended in our national dietary guidelines, the Australian Guide for Healthy Eating.

Seed oils often have a high smoke point.
Gleb Usovich/ShutterstockI’ve heard people say seed oils ‘promote inflammation’. Is that true?
There are two essential types of omega fatty acids: omega-3 and omega-6. These are crucial for bodily functions, and we must get them through our diet since our bodies cannot produce them.
While all oils contain varying levels of fatty acids, some argue an excessive intake of a specific omega-6 fatty acid in seed oils called “linoleic acid” may contribute to inflammation in the body.
There is some evidence linoleic acid can be converted to arachidonic acid in the body and this may play a role in inflammation. However, other research doesn’t support the idea reducing dietary linoleic acid affects the amount of arachidonic acid in your body. The research picture is not clear cut.
But if you’re keen to reduce inflammation, the best thing you can do is aim for a healthy diet that is:
- high in antioxidants (found in fruits and vegetables)
- high in “healthy”, unsaturated fatty acids (found in fatty fish, some nuts and olive oil, for example)
high in fibre (found in carrots, cauliflower, broccoli and leafy greens) and prebiotics (found in onions, leeks, asparagus, garlic and legumes)
low in processed foods.
If reducing inflammation is your goal, it’s probably more meaningful to focus on these basics than on occasional use of seed oils.
Choose foods high in fibre (like many vegetables) and prebiotics (like legumes).
Kiian Oksana/ShutterstockWhat about seed oils and heart disease, cancer or diabetes risk?
Some popular arguments against seed oils come from data from single studies on this topic. Often these are observational studies where researchers do not make changes to people’s diet or lifestyle.
To get a clearer picture, we should look at meta-analyses, where scientists combine all the data available on a topic. This helps us get a better overall view of what’s going on.
A 2022 meta-analysis of randomised controlled trials investigated the relationship between supplementation with omega-6 fatty acid (often found in seed oils) and cardiovascular disease risk (meaning disease relating to the heart and blood vessels).
The researchers found omega-6 intake did not affect the risk for cardiovascular disease or death but that further research is needed for firm conclusions. Similar findings were observed in a 2019 review on this topic.
The World Health Organization published a review and meta-analysis in 2022 of observational studies (considered lower quality evidence compared to randomised controlled trials) on this topic.
They looked at omega-6 intake and risk of death, cardiovascular disease, breast cancer, mental health conditions and type 2 diabetes. The findings show both advantages and disadvantages of consuming omega-6.
The findings reported that, overall, higher intakes of omega-6 were associated with a 9% reduced risk of dying (data from nine studies) but a 31% increased risk of postmenopausal breast cancer (data from six studies).
One of the key findings from this review was about the ratio of omega-3 fatty acids to omega-6 fatty acids. A higher omega 6:3 ratio was associated with a greater risk of cognitive decline and ulcerative colitis (an inflammatory bowel condition).
A higher omega 3:6 ratio was linked to a 26% reduced risk of depression. These mixed outcomes may be a cause of confusion among health-conscious consumers about the health impact of seed oils.
Overall, the evidence suggests that a high intake of omega-6 fatty acids from seed oils is unlikely to increase your risk of death and disease.
However, more high-quality intervention research is needed.
The importance of increasing your omega-3 fatty acids
On top of the mixed outcomes, there is clear evidence increasing the intake of omega-3 fatty acids (often found in foods such as fatty fish and walnuts) is beneficial for health.
While some seed oils contain small amounts of omega-3s, they are not typically considered rich sources.
Flaxseed oil is an exception and is one of the few seed oils that is notably high in alpha-linolenic acid (sometimes shortened to ALA), an omega-3 fatty acid.
If you are looking to increase your omega-3 intake, it’s better to focus on other sources such as fatty fish (salmon, mackerel, sardines), chia seeds, hemp seeds, walnuts, and algae-based supplements. These foods are known for their higher omega-3 content compared to seed oils.
The bottom line
At the end of the day, it’s probably OK to include small quantities of seed oils in your diet, as long as you are mostly focused on eating fresh, unprocessed foods.
The best way to reduce your risk of inflammation, heart disease, cancer or diabetes is not to focus so much on seed oils but rather on doing your best to follow the Australian Guide for Healthy Eating.

Lauren Ball, Professor of Community Health and Wellbeing, The University of Queensland and Emily Burch, Lecturer, Southern Cross University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



Related Posts
-

Hitting the beach? Here are some dangers to watch out for – plus 10 essentials for your first aid kit
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Summer is here and for many that means going to the beach. You grab your swimmers, beach towel and sunscreen then maybe check the weather forecast. Did you think to grab a first aid kit?
The vast majority of trips to the beach will be uneventful. However, if trouble strikes, being prepared can make a huge difference to you, a loved one or a stranger.
So, what exactly should you be prepared for?
FTiare/Shutterstock Knowing the dangers
The first step in being prepared for the beach is to learn about where you are going and associated levels of risk.
In Broome, you are more likely to be bitten by a dog at the beach than stung by an Irukandji jellyfish.
In Byron Bay, you are more likely to come across a brown snake than a shark.
In the summer of 2023–24, Surf Life Saving Australia reported more than 14 million Australian adults visited beaches. Surf lifesavers, lifeguards and lifesaving services performed 49,331 first aid treatments across 117 local government areas around Australia. Surveys of beach goers found perceptions of common beach hazards include rips, tropical stingers, sun exposure, crocodiles, sharks, rocky platforms and waves.
Sun and heat exposure are likely the most common beach hazard. The Cancer Council has reported that almost 1.5 million Australians surveyed during summer had experienced sunburn during the previous week. Without adequate fluid intake, heat stroke can also occur.
Lacerations and abrasions are a further common hazard. While surfboards, rocks, shells and litter might seem more dangerous, the humble beach umbrella has been implicated in thousands of injuries.
Sprains and fractures are also associated with beach activities. A 2022 study linked data from hospital, ambulance and Surf Life Saving cases on the Sunshine Coast over six years and found 79 of 574 (13.8%) cervical spine injuries occurred at the beach. Surfing, smaller wave heights and shallow water diving were the main risks.
Rips and rough waves present a higher risk at areas of unpatrolled beach, including away from surf lifesaving flags. Out of 150 coastal drowning deaths around Australia in 2023–24, nearly half were during summer. Of those deaths:
- 56% occurred at the beach
- 31% were rip-related
- 86% were male, and
- 100% occurred away from patrolled areas.
People who had lived in Australia for less than two years were more worried about the dangers, but also more likely to be caught in a rip.
Safety Beach on Victoria’s Mornington Peninsula. Still bring your first aid essentials though. Julia Kuleshova/Shutterstock Knowing your DR ABCs
So, beach accidents can vary by type, severity and impact. How you respond will depend on your level of first aid knowledge, ability and what’s in your first aid kit.
A first aid training company survey of just over 1,000 Australians indicated 80% of people agree cardiopulmonary resuscitation (CPR) is the most important skill to learn, but nearly half reported feeling intimidated by the prospect.
CPR training covers an established checklist for emergency situations. Using the acronym “DR ABC” means checking for:
- Danger
- Response
- Airway
- Breathing
- Circulation
A complete first aid course will provide a range of skills to build confidence and be accredited by the national regulator, the Australian Skills Quality Authority.
What to bring – 10 first aid essentials
Whether you buy a first aid kit or put together you own, it should include ten essential items in a watertight, sealable container:
- Band-Aids for small cuts and abrasions
- sterile gauze pads
- bandages (one small one for children, one medium crepe to hold on a dressing or support strains or sprains, and one large compression bandage for a limb)
- large fabric for sling
- a tourniquet bandage or belt to restrict blood flow
- non-latex disposable gloves
- scissors and tweezers
- medical tape
- thermal or foil blanket
- CPR shield or breathing mask.
Before you leave for the beach, check the expiry dates of any sunscreen, solutions or potions you choose to add.
If you’re further from help
If you are travelling to a remote or unpatrolled beach, your kit should also contain:
- sterile saline solution to flush wounds or rinse eyes
- hydrogel or sunburn gel
- an instant cool pack
- paracetamol and antihistamine medication
- insect repellent.
Make sure you carry any “as-required” medications, such as a Ventolin puffer for asthma or an EpiPen for severe allergy.
Vinegar is no longer recommended for most jellyfish stings, including Blue Bottles. Hot water is advised instead.
In remote areas, also look out for Emergency Response Beacons. Located in high-risk spots, these allow bystanders to instantly activate the surf emergency response system.
If you have your mobile phone or a smart watch with GPS function, make sure it is charged and switched on and that you know how to use it to make emergency calls.
First aid kits suitable for the beach range in price from $35 to over $120. Buy these from certified first aid organisations such as Surf Lifesaving Australia, Australian Red Cross, St John Ambulance or Royal Life Saving. Kits that come with a waterproof sealable bag are recommended.
Be prepared this summer for your trip to the beach and pack your first aid kit. Take care and have fun in the sun.
Andrew Woods, Lecturer, Nursing, Faculty of Health, Southern Cross University and Willa Maguire, Associate Lecturer in Nursing, Southern Cross University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Some women’s breasts can’t make enough milk, and the effects can be devastating
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many new mothers worry about their milk supply. For some, support from a breastfeeding counsellor or lactation consultant helps.
Others cannot make enough milk no matter how hard they try. These are women whose breasts are not physically capable of producing enough milk.
Our recently published research gives us clues about breast features that might make it difficult for some women to produce enough milk. Another of our studies shows the devastating consequences for women who dream of breastfeeding but find they cannot.
Some breasts just don’t develop
Unlike other organs, breasts are not fully developed at birth. There are key developmental stages as an embryo, then again during puberty and pregnancy.
At birth, the breast consists of a simple network of ducts. Usually during puberty, the glandular (milk-making) tissue part of the breast begins to develop and the ductal network expands. Then typically, further growth of the ductal network and glandular tissue during pregnancy prepares the breast for lactation.
But our online survey of women who report low milk supply gives us clues to anomalies in how some women’s breasts develop.
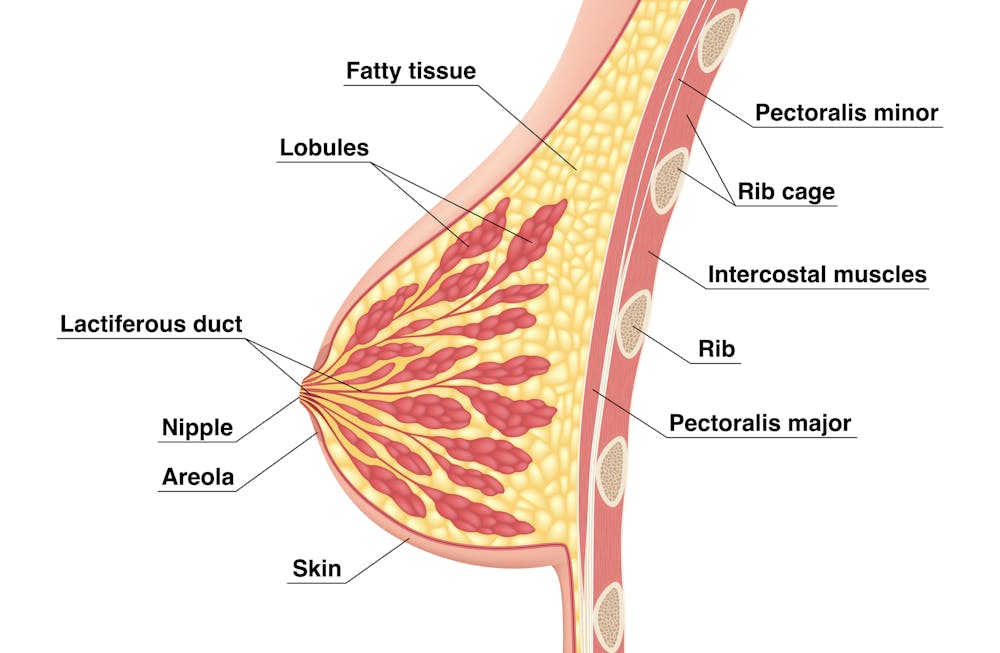
We’re not talking about women with small breasts, but women whose glandular tissue (shown in this diagram as “lobules”) is underdeveloped and have a condition called breast hypoplasia.
Sometimes not enough glandular tissue, shown here as lobules, develop.
Tsuyna/ShutterstockWe don’t know how common this is. But it has been linked with lower rates of exclusive breastfeeding.
We also don’t know what causes it, with much of the research conducted in animals and not humans.
However, certain health conditions have been associated with it, including polycystic ovary syndrome and other endocrine (hormonal) conditions. A high body-mass index around the time of puberty may be another indicator.
Could I have breast hypoplasia?
Our survey and other research give clues about who may have breast hypoplasia.
But it’s important to note these characteristics are indicators and do not mean women exhibiting them will definitely be unable to exclusively breastfeed.
Indicators include:
- a wider than usual gap between the breasts
- tubular-shaped (rather than round) breasts
- asymmetric breasts (where the breasts are different sizes or shapes)
- lack of breast growth in pregnancy
- a delay in or absence of breast fullness in the days after giving birth
In our survey, 72% of women with low milk supply had breasts that did not change appearance during pregnancy, and about 70% reported at least one irregular-shaped breast.
The effects
Mothers with low milk supply – whether or not they have breast hyoplasia or some other condition that limits their ability to produce enough milk – report a range of emotions.
Research, including our own, shows this ranges from frustration, confusion and surprise to intense or profound feelings of failure, guilt, grief and despair.
Some mothers describe “breastfeeding grief” – a prolonged sense of loss or failure, due to being unable to connect with and nourish their baby through breastfeeding in the way they had hoped.
These feelings of failure, guilt, grief and despair can trigger symptoms of anxiety and depression for some women.
Feelings of failure, guilt, grief and despair were common.
Bricolage/ShutterstockOne woman told us:
[I became] so angry and upset with my body for not being able to produce enough milk.
Many women’s emotions intensified when they discovered that despite all their hard work, they were still unable to breastfeed their babies as planned. A few women described reaching their “breaking point”, and their experience felt “like death”, “the worst day of [my] life” or “hell”.
One participant told us:
I finally learned that ‘all women make enough milk’ was a lie. No amount of education or determination would make my breasts work. I felt deceived and let down by all my medical providers. How dare they have no answers for me when I desperately just wanted to feed my child naturally.
Others told us how they learned to accept their situation. Some women said they were relieved their infant was “finally satisfied” when they began supplementing with formula. One resolved to:
prioritise time with [my] baby over pumping for such little amounts.
Where to go for help
If you are struggling with low milk supply, it can help to see a lactation consultant for support and to determine the possible cause.
This will involve helping you try different strategies, such as optimising positioning and attachment during breastfeeding, or breastfeeding/expressing more frequently. You may need to consider taking a medication, such as domperidone, to see if your supply increases.
If these strategies do not help, there may be an underlying reason why you can’t make enough milk, such as insufficient glandular tissue (a confirmed inability to make a full supply due to breast hypoplasia).
Even if you have breast hypoplasia, you can still breastfeed by giving your baby extra milk (donor milk or formula) via a bottle or using a supplementer (which involves delivering milk at the breast via a tube linked to a bottle).
More resources
The following websites offer further information and support:
- Australian Breastfeeding Association
- Lactation Consultants of Australia and New Zealand
- Royal Women’s Hospital, Melbourne
- Supply Line Breastfeeders Support Group of Australia Facebook support group
- IGT And Low Milk Supply Support Group Facebook support group
- Breastfeeding Medicine Network Australia/New Zealand
- Supporting breastfeeding grief (a collection of resources).
Shannon Bennetts, a research fellow at La Trobe University, contributed to this article.
Renee Kam, PhD candidate and research officer, La Trobe University and Lisa Amir, Professor in Breastfeeding Research, La Trobe University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Taking A Trip Through The Evidence On Psychedelics
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

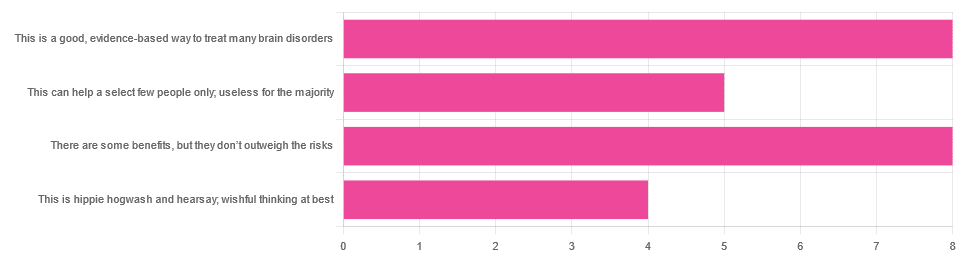
In Tuesday’s newsletter, we asked you for your opinions on the medicinal use of psychedelics, and got the above-depicted, below-described, set of responses:
- 32% said “This is a good, evidence-based way to treat many brain disorders”
- 32% said “There are some benefits, but they don’t outweigh the risks”
- 20% said “This can help a select few people only; useless for the majority”
- 16% said “This is hippie hogwash and hearsay; wishful thinking at best”
Quite a spread of answers, so what does the science say?
This is hippie hogwash and hearsay; wishful thinking at best! True or False?
False! We’re tackling this one first, because it’s easiest to answer:
There are some moderately-well established [usually moderate] clinical benefits from some psychedelics for some people.
If that sounds like a very guarded statement, it is. Part of this is because “psychedelics” is an umbrella term; perhaps we should have conducted separate polls for psilocybin, MDMA, ayahuasca, LSD, ibogaine, etc, etc.
In fact: maybe we will do separate main features for some of these, as there is a lot to say about each of them separately.
Nevertheless, looking at the spread of research as it stands for psychedelics as a category, the answers are often similar across the board, even when the benefits/risks may differ from drug to drug.
To speak in broad terms, if we were to make a research summary for each drug it would look approximately like this in each case:
- there has been research into this, but not nearly enough, as “the war on drugs” may well have manifestly been lost (the winner of the war being: drugs; still around and more plentiful than ever), but it did really cramp science for a few decades.
- the studies are often small, heterogenous (often using moderately wealthy white student-age population samples), and with a low standard of evidence (i.e. the methodology often has some holes that leave room for reasonable doubt).
- the benefits recorded are often small and transient.
- in their favor, though, the risks are also generally recorded as being quite low, assuming proper safe administration*.
*Illustrative example:
Person A takes MDMA in a club, dances their cares away, has had only alcohol to drink, sweats buckets but they don’t care because they love everyone and they see how we’re all one really and it all makes sense to them and then they pass out from heat exhaustion and dehydration and suffer kidney damage (not to mention a head injury when falling) and are hospitalized and could die;
Person B takes MDMA in a lab, is overwhelmed with a sense of joy and the clarity of how their participation in the study is helping humanity; they want to hug the researcher and express their gratitude; the researcher reminds them to drink some water.
Which is not to say that a lab is the only safe manner of administration; there are many possible setups for supervised usage sites. But it does mean that the risks are often as much environmental as they are risks inherent to the drug itself.
Others are more inherent to the drug itself, such as adverse cardiac events for some drugs (ibogaine is one that definitely needs medical supervision, for example).
For those who’d like to see numbers and clinical examples of the bullet points we gave above, here you go; this is a great (and very readable) overview:
NIH | Evidence Brief: Psychedelic Medications for Mental Health and Substance Use Disorders
Notwithstanding the word “brief” (intended in the sense of: briefing), this is not especially brief and is rather an entire book (available for free, right there!), but we do recommend reading it if you have time.
This can help a select few people only; useless for the majority: True or False?
True, technically, insofar as the evidence points to these drugs being useful for such things as depression, anxiety, PTSD, addiction, etc, and estimates of people who struggle with mental health issues in general is often cited as being 1 in 4, or 1 in 5. Of course, many people may just have moderate anxiety, or a transient period of depression, etc; many, meanwhile, have it worth.
In short: there is a very large minority of people who suffer from mental health issues that, for each issue, there may be one or more psychedelic that could help.
This is a good, evidence-based way to treat many brain disorders: True or False?
True if and only if we’re willing to accept the so far weak evidence that we discussed above. False otherwise, while the jury remains out.
One thing in its favor though is that while the evidence is weak, it’s not contradictory, insofar as the large preponderance of evidence says such therapies probably do work (there aren’t many studies that returned negative results); the evidence is just weak.
When a thousand scientists say “we’re not completely sure, but this looks like it helps; we need to do more research”, then it’s good to believe them on all counts—the positivity and the uncertainty.
This is a very different picture than we saw when looking at, say, ear candling or homeopathy (things that the evidence says simply do not work).
We haven’t been linking individual studies so far, because that book we linked above has many, and the number of studies we’d have to list would be:
n = number of kinds of psychedelic drugs x number of conditions to be treated
e.g. how does psilocybin fare for depression, eating disorders, anxiety, addiction, PTSD, this, that, the other; now how does ayahuasca fare for each of those, and so on for each drug and condition; at least 25 or 30 as a baseline number, and we don’t have that room.
But here are a few samples to finish up:
- Psilocybin as a New Approach to Treat Depression and Anxiety in the Context of Life-Threatening Diseases—A Systematic Review and Meta-Analysis of Clinical Trials
- Therapeutic Use of LSD in Psychiatry: A Systematic Review of Randomized-Controlled Clinical Trials
- Efficacy of Psychoactive Drugs for the Treatment of Posttraumatic Stress Disorder: A Systematic Review of MDMA, Ketamine, LSD and Psilocybin
- Changes in self-rumination and self-compassion mediate the effect of psychedelic experiences on decreases in depression, anxiety, and stress.
- Psychedelic Treatments for Psychiatric Disorders: A Systematic Review and Thematic Synthesis of Patient Experiences in Qualitative Studies
- Repeated lysergic acid diethylamide (LSD) reverses stress-induced anxiety-like behavior, cortical synaptogenesis deficits and serotonergic neurotransmission decline
In closing…
The general scientific consensus is presently “many of those drugs may ameliorate many of those conditions, but we need a lot more research before we can say for sure”.
On a practical level, an important take-away from this is twofold:
- drugs, even those popularly considered recreational, aren’t ontologically evil, generally do have putative merits, and have been subject to a lot of dramatization/sensationalization, especially by the US government in its famous war on drugs.
- drugs, even those popularly considered beneficial and potentially lifechangingly good, are still capable of doing great harm if mismanaged, so if putting aside “don’t do drugs” as a propaganda of the past, then please do still hold onto “don’t do drugs alone”; trained professional supervision is a must for safety.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: