Syringe Exchange Fears Hobble Fight Against West Virginia HIV Outbreak
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
CHARLESTON, http://w.va/. — More than three years have passed since federal health officials arrived in central Appalachia to assess an alarming outbreak of HIV spread mostly between people who inject opioids or methamphetamine.
Infectious disease experts from the Centers for Disease Control and Prevention made a list of recommendations following their visit, including one to launch syringe service programs to stop the spread at its source. But those who’ve spent years striving to protect people who use drugs from overdose and illness say the situation likely hasn’t improved, in part because of politicians who contend that such programs encourage illegal drug use.
Joe Solomon is a Charleston City Council member and co-director of SOAR WV, a group that works to address the health needs of people who use drugs. He’s proud of how his close-knit community has risen to this challenge but frustrated with the restraints on its efforts.
“You see a city and a county willing to get to work at a scale that’s bigger than ever before,” Solomon said, “but we still have one hand tied behind our back.”
The hand he references is easier access to clean syringes.
In April 2021, the CDC came to Charleston — the seat of Kanawha County and the state capital, tucked into the confluence of the Kanawha and Elk rivers — to investigate dozens of newly detected HIV infections. The CDC’s HIV intervention chief called it “the most concerning HIV outbreak in the United States” and warned that the number of reported diagnoses could be just “the tip of the iceberg.”
Now, despite attention and resources directed toward the outbreak, researchers and health workers say HIV continues to spread. In large part, they say, the outbreak lingers because of restrictions state and local policymakers have placed on syringe exchange efforts.
Research indicates that syringe service programs are associated with an estimated 50% reduction in HIV and hepatitis C, and the CDC issued recommendations to steer a response to the outbreak that emphasized the need for improved access to those services.
That advice has thus far gone unheeded by local officials.
In late 2015, the Kanawha-Charleston Health Department launched a syringe service program but shuttered it in 2018 under pressure, with then-Mayor Danny Jones calling it a “mini-mall for junkies and drug dealers.”
SOAR stepped in, hosting health fairs at which it distributed naloxone, an opioid overdose reversal drug; offered treatment and referrals; provided HIV testing; and exchanged clean syringes for used ones.
But in April 2021, the state legislature passed a bill limiting the number of syringes people could exchange and made it mandatory to present a West Virginia ID. The Charleston City Council subsequently added guidelines of its own, including requiring individual labeling of syringes.
As a result of these restrictions, SOAR ceased exchanging syringes. West Virginia Health Right now operates an exchange program in the city under the restrictions.
Robin Pollini is a West Virginia University epidemiologist who conducts community-based research on injection drug use. “Anyone I’ve talked to who’s used that program only used it once,” she said. “And the numbers they report to the state bear that out.”
A syringe exchange run by the health department in nearby Cabell County — home to Huntington, the state’s largest city after Charleston — isn’t so constrained. As Solomon notes, that program exchanges more than 200 syringes for every one exchanged in Kanawha.
A common complaint about syringe programs is that they result in discarded syringes in public spaces. Jan Rader, director of Huntington’s Mayor’s Office of Public Health and Drug Control Policy, is regularly out on the streets and said she seldom encounters discarded syringes, pointing out that it’s necessary to exchange a used syringe for a new one.
In August 2023, the Charleston City Council voted down a proposal from the Women’s Health Center of West Virginia to operate a syringe exchange in the city’s West Side community, with opponents expressing fears of an increase in drug use and crime.
Pollini said it’s difficult to estimate the number of people in West Virginia with HIV because there’s no coordinated strategy for testing; all efforts are localized.
“You would think that in a state that had the worst HIV outbreak in the country,” she said, “by this time we would have a statewide testing strategy.”
In addition to the testing SOAR conducted in 2021 at its health fairs, there was extensive testing during the CDC’s investigation. Since then, the reported number of HIV cases in Kanawha County has dropped, Pollini said, but it’s difficult to know if that’s the result of getting the problem under control or the result of limited testing in high-risk groups.
“My inclination is the latter,” she said, “because never in history has there been an outbreak of injection-related HIV among people who use drugs that was solved without expanding syringe services programs.”
“If you go out and look for infections,” Pollini said, “you will find them.”
Solomon and Pollini praised the ongoing outreach efforts — through riverside encampments, in abandoned houses, down county roads — of the Ryan White HIV/AIDS Program to test those at highest risk: people known to be injecting drugs.
“It’s miracle-level work,” Solomon said.
But Christine Teague, Ryan White Program director at the Charleston Area Medical Center, acknowledged it hasn’t been enough. In addition to HIV, her concerns include the high incidence of hepatitis C and endocarditis, a life-threatening inflammation of the lining of the heart’s chambers and valves, and the cost of hospital resources needed to address them.
“We’ve presented that data to the legislature,” she said, “that it’s not just HIV, it’s all these other lengthy hospital admissions that, essentially, Medicaid is paying for. And nothing seems to penetrate.”
Frank Annie is a researcher at CAMC specializing in cardiovascular diseases, a member of the Charleston City Council, and a proponent of syringe service programs. Research he co-authored found 462 cases of endocarditis in southern West Virginia associated with injection drug use, at a cost to federal, state, and private insurers of more than $17 million, of which less than $4 million was recovered.
Teague is further concerned for West Virginia’s rural counties, most of which don’t have a syringe service program.
Tasha Withrow, a harm reduction advocate in bordering rural Putnam County, said her sense is that HIV numbers aren’t alarmingly high there but said that, with little testing and heightened stigma in a rural community, it’s difficult to know.
In a January 2022 follow-up report, the CDC recommended increasing access to harm reduction services such as syringe service programs through expansion of mobile services, street outreach, and telehealth, using “patient-trusted” individuals, to improve the delivery of essential services to people who use drugs.
Teague would like every rural county to have a mobile unit, like the one operated by her organization, offering harm reduction supplies, medication, behavioral health care, counseling, referrals, and more. That’s an expensive undertaking. She suggested opioid settlement money through the West Virginia First Foundation could pay for it.
Pollini said she hopes state and local officials allow the experts to do their jobs.
“I would like to see them allow us to follow the science and operate these programs the way they’re supposed to be run, and in a broader geography,” she said. “Which means that it shouldn’t be a political decision; it should be a public health decision.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Fix Chronic Fatigue & Regain Your Energy, By Science

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Chronic fatigue is on the rise. A lot of it appears to be Long COVID-related, but whether that’s the case for you or not, one thing that will make a big difference to your energy levels is something that French biochemist Jessie Inchauspé is here to explain:
Mitochondrial management
Inchauspé explains it in terms of a steam train; to keep running, it must have coal burning in its furnace. However, if more coal is delivered to the engine room faster than it can be put in the furnace and burned, and the coal just keeps on coming, the worker there will soon be overwhelmed trying to find places to put it all; the engine room will be full of coal, and the furnace will sputter and go out because the worker can’t even reach it on account of being buried in coal.
So it is with our glucose metabolism also. If we get spikes of glucose faster than our body can deal with them, it will overload the body’s ability to process that energy at all. Just like the steam train worker, our body will try! It’ll stuff that extra glucose wherever it can (storing as glycogen in the liver is a readily available option that’s easy to do and/but also gives you non-alcoholic fatty liver disease and isn’t quickly broken down into useable energy), and meanwhile, your actual mitochondria aren’t getting what they need (which is: a reliable, but gentle, influx of glucose).
You can imagine that the situation we described in the steam train isn’t good for the engine’s longevity, and the corresponding situation in the human body isn’t good for our mitochondria either (or our pancreas, or our liver, or… the list goes on). Indeed, damaged mitochondria affect exercise capacity and stress resilience—as well as being a long-term driver of cancer.
The remedy, of course, is blood sugar management. Specifically, avoiding glucose spikes. She has a list of 10 ways to do this (small changes to how we eat; what things to eat with what, in which order, etc) that make a huge measurable difference. For your convenience, we’ve linked those ten ways below; first though, if you’d like to hear it from Inchauspé directly (her style is very pleasant), enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- 10 Ways To Balance Your Blood Sugars ← this is the longer list she’s referring to in the video!
- How To Unfatty A Fatty Liver ← also relevant
Take care!
Share This Post
-

Gluten: What’s The Truth?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Gluten: What’s The Truth?

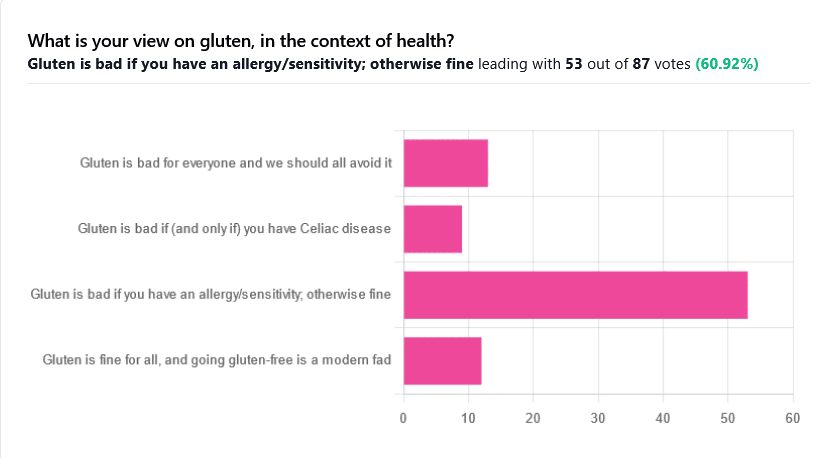
We asked you for your health-related view of gluten, and got the above spread of results. To put it simply:
Around 60% of voters voted for “Gluten is bad if you have an allergy/sensitivity; otherwise fine”
The rest of the votes were split fairly evenly between the other three options:
- Gluten is bad for everyone and we should avoid it
- Gluten is bad if (and only if) you have Celiac disease
- Gluten is fine for all, and going gluten-free is a modern fad
First, let’s define some terms so that we’re all on the same page:
What is gluten?
Gluten is a category of protein found in wheat, barley, rye, and triticale. As such, it’s not one single compound, but a little umbrella of similar compounds. However, for the sake of not making this article many times longer, we’re going to refer to “gluten” without further specification.
What is Celiac disease?
Celiac disease is an autoimmune disease. Like many autoimmune diseases, we don’t know for sure how/why it occurs, but a combination of genetic and environmental factors have been strongly implicated, with the latter putatively including overexposure to gluten.
It affects about 1% of the world’s population, and people with Celiac disease will tend to respond adversely to gluten, notably by inflammation of the small intestine and destruction of enterocytes (the cells that line the wall of the small intestine). This in turn causes all sorts of other problems, beyond the scope of today’s main feature, but suffice it to say, it’s not pleasant.
What is an allergy/intolerance/sensitivity?
This may seem basic, but a lot of people conflate allergy/intolerance/sensitivity, so:
- An allergy is when the body mistakes a harmless substance for something harmful, and responds inappropriately. This can be mild (e.g. allergic rhinitis, hayfever) or severe (e.g. peanut allergy), and as such, responses can vary from “sniffly nose” to “anaphylactic shock and death”.
- In the case of a wheat allergy (for example), this is usually somewhere between the two, and can for example cause breathing problems after ingesting wheat or inhaling wheat flour.
- An intolerance is when the body fails to correctly process something it should be able to process, and just ejects it half-processed instead.
- A common and easily demonstrable example is lactose intolerance. There isn’t a well-defined analog for gluten, but gluten intolerance is nonetheless a well-reported thing.
- A sensitivity is when none of the above apply, but the body nevertheless experiences unpleasant symptoms after exposure to a substance that should normally be safe.
- In the case of gluten, this is referred to as non-Celiac gluten sensitivity
A word on scientific objectivity: at 10almonds we try to report science as objectively as possible. Sometimes people have strong feelings on a topic, especially if it is polarizing.
Sometimes people with a certain condition feel constantly disbelieved and mocked; sometimes people without a certain condition think others are imagining problems for themselves where there are none.
We can’t diagnose anyone or validate either side of that, but what we can do is report the facts as objectively as science can lay them out.
Gluten is fine for all, and going gluten-free is a modern fad: True or False?
Definitely False, Celiac disease is a real autoimmune disease that cannot be faked, and allergies are also a real thing that people can have, and again can be validated in studies. Even intolerances have scientifically measurable symptoms and can be tested against nocebo.
See for example:
- Epidemiology and clinical presentations of Celiac disease
- Severe forms of food allergy that can precipitate allergic emergencies
- Properties of gluten intolerance: gluten structure, evolution, and pathogenicity
However! It may not be a modern fad, so much as a modern genuine increase in incidence.
Widespread varieties of wheat today contain a lot more gluten than wheat of ages past, and many other molecular changes mean there are other compounds in modern grains that never even existed before.
However, the health-related impact of these (novel proteins and carbohydrates) is currently still speculative, and we are not in the business of speculating, so we’ll leave that as a “this hasn’t been studied enough to comment yet but we recognize it could potentially be a thing” factor.
Gluten is bad if (and only if) you have Celiac disease: True or False?
Definitely False; allergies for example are well-evidenced as real; same facts as we discussed/linked just above.
Gluten is bad for everyone and we should avoid it: True or False?
False, tentatively and contingently.
First, as established, there are people with clinically-evidenced Celiac disease, wheat allergy, or similar. Obviously, they should avoid triggering those diseases.
What about the rest of us, and what about those who have non-Celiac gluten sensitivity?
Clinical testing has found that of those reporting non-Celiac gluten sensitivity, nocebo-controlled studies validate that diagnosis in only a minority of cases.
In the following study, for example, only 16% of those reporting symptoms showed them in the trials, and 40% of those also showed a nocebo response (i.e., like placebo, but a bad rather than good effect):
This one, on the other hand, found that positive validations of diagnoses were found to be between 7% and 77%, depending on the trial, with an average of 30%:
Re-challenge Studies in Non-celiac Gluten Sensitivity: A Systematic Review and Meta-Analysis
In other words: non-Celiac gluten sensitivity is a thing, and/but may be over-reported, and/but may be in some part exacerbated by psychosomatic effect.
Note: psychosomatic effect does not mean “imagining it” or “all in your head”. Indeed, the “soma” part of the word “psychosomatic” has to do with its measurable effect on the rest of the body.
For example, while pain can’t be easily objectively measured, other things, like inflammation, definitely can.
As for everyone else? If you’re enjoying your wheat (or similar) products, it’s well-established that they should be wholegrain for the best health impact (fiber, a positive for your health, rather than white flour’s super-fast metabolites padding the liver and causing metabolic problems).
Wheat itself may have other problems, for example FODMAPs, amylase trypsin inhibitors, and wheat germ agglutinins, but that’s “a wheat thing” rather than “a gluten thing”.
That’s beyond the scope of today’s main feature, but you might want to check out today’s featured book!
For a final scientific opinion on this last one, though, here’s what a respected academic journal of gastroenterology has to say:
From coeliac disease to noncoeliac gluten sensitivity; should everyone be gluten-free?
Share This Post
-

It’s OK to use paracetamol in pregnancy. Here’s what the science says about the link with autism
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
United States President Donald Trump has urged pregnant women to avoid paracetamol except in cases of extremely high fever, because of a possible link to autism.
Paracetamol – known as acetaminophen or by the brand name Tylenol in the US – is commonly used to relieve pain, such as back pain and headaches, and to reduce fever during pregnancy.
Australia’s Therapeutic Goods Administration today re-affirmed existing medical guidelines that it’s safe for pregnant women to take paracetamol at any stage of pregnancy.
Paracetamol is classified as a Category A drug. This means many pregnant women and women of childbearing age have long used it without increases in birth defects or harmful effects on the fetus.
It’s important to treat fevers in pregnancy. Untreated high fever in early pregnancy is linked to miscarriage, neural tube defects, cleft lip and palate, and heart defects. Infections in pregnancy have also been linked to greater risks of autism.
How has the research evolved in recent years?
In 2021 an international panel of experts looked at evidence from human and animal studies of paracetamol use in pregnancy. Their consensus statement warned that paracetamol use during pregnancy may alter fetal development, with negative effects on child health.
Last month a a group of researchers from Harvard University examined the association between paracetamol and neurodevelopmental disorders including autism and attention-deficit hyperactivity disorder (ADHD) in existing research.
They identified 46 studies and found 27 studies reported links between taking paracetamol in pregnancy and neurodevelopmental disorders in the offspring, nine showed no significant link, and four indicated it was associated with a lower risk.
The most notable study in their review, due to its sophisticated statistical analysis, covered almost 2.5 million children born in Sweden between 1995 and 2019, and was published in 2024.
The authors found there was a marginally increased risk of autism and ADHD associated with paracetamol use during pregnancy. However, when the researchers analysed matched-full sibling pairs, to account for genetic and environmental influences the siblings shared, the researchers found no evidence of an increased risk of autism, ADHD, or intellectual disability associated with paracetamol use.
Siblings of autistic children have a 20% chance of also being autistic. Environmental factors within a home can also affect the risk of autism. To account for these influences, the researchers compared the outcomes of siblings where one child was exposed to paracetamol in utero and the other wasn’t, or when the siblings had different levels of exposure.
The authors of the 2024 study concluded that associations found in other studies may be attributable to “confounding” factors: influences that can distort research findings.
A further review published in February examined the strengths and limitations of the published literature on the effect of paracetamol use in pregnancy on the child’s risk of developing ADHD and autism. The authors noted most studies were difficult to interpret because they had biases, including in selecting participants, and they didn’t for confounding factors.
When confounding factors among siblings were accounted for, they found any associations weakened substantially. This suggests shared genetic and environmental factors may have caused bias in the original observations.
Working out what causes or increases the risk of autism
A key piece to consider when assessing the risk of paracetamol and any link to neurodevelopmental disorders is how best to account for many other potentially relevant factors that may be important.
We still don’t know all the causes of autism, but several genetic and non-genetic factors have been implicated: the mother’s medication use, illnesses, body mass index, alcohol consumption, smoking status, pregnancy complications including pre-eclampsia and fetal growth restriction, the mother and father’s ages, whether the child is an older or younger sibling, the newborn’s Apgar scores to determine their state of health, breastfeeding, genetics, socioeconomic status, and societal characteristics.
It’s particularly hard to measure the last three characteristics, so they are often not appropriately taken into account in studies.
Other times, it may not be the use of paracetamol that is important but rather the mother’s underlying illness or reason paracetamol is being taken, such as the fever associated with an infection, that influences child development.
I’m pregnant, what does this mean for me?
There is no clear evidence that paracetamol has any harmful effects on an unborn baby.
But as with any medicine taken during pregnancy, paracetamol should be used at the lowest effective dose for the shortest possible time.
If you’re pregnant and develop a fever, it’s important to treat this fever, including with paracetamol.
If the recommended dose of paracetamol doesn’t control your symptoms or you’re in pain, contact your doctor, midwife or maternity hospital for further medical advice.
Remember, the advice for taking ibuprofen and other NSAIDS when you’re pregnant is different. Ibuprofen (sold under the brand name Nurofen) should not be taken during pregnancy.
Nicholas Wood, Professor, The Children’s Hospital at Westmead Clinical School, University of Sydney and Debra Kennedy, Conjoint Associate Professor, School of Women’s and Children’s Health, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post


-

The Complete Guide To Red Light Therapy – by Dr. Melanie Gray
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Red light therapy (RLT) is one of those things that sounds like it should be an ineffectual new-age fad that doesn’t do anything, but in fact, there’s a lot of evidence to show that it confers many benefits.
In particular, and to oversimply rather because this is a book review and not a scientific article (though we have written about RLT before and linked to various studies there), RLT is most noted for rejuvenating skin, and enhancing the healing of same, where applicable.
Dr. Gray explains not just what it does, but also some of how it does it, involving the stimulation of mitochondria, DNA-and-telomere repair, and more. She also talks the difference between RLT and near-infrared therapy, which are often delivered by the same devices, just, we can see part of the spectrum and not the other part.
She covers practical matters too, such as optimizing the frequency for different purposes (helpful when choosing a device, or when adjusting the settings on a multi-setting device), as well as optimal treatment duration, and other factors that can affect dosage (including the intensity of the light, and your skintone).
The style is… a little mixed, and can read a little like AI was involved. But on the bright side, it’s a perfectly easy read (and a short one, at 104 pages), and the author’s input includes a lot of niche technical knowledge, which makes it worthwhile. The bibliography is 12 items long and only 5 of those are scholarly articles, but honestly, she could have padded it with a lot more hard-science evidence for RLT’s benefits and it wouldn’t have actually increased the practical value of the book, so we don’t think this is a terrible thing.
Bottom line: this will probably not become anyone’s favorite book, but it is actually useful, and can help you to get the most out of RLT.
Click here to check out The Complete Guide To Red Light Therapy, and enjoy a healthy glow!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Science of Pilates – by Tracy Ward
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve reviewed other books in this series, “Science of Yoga” and “Science of HIIT” (they’re great too; check them out!). What does this one add to the mix?
Pilates is a top-tier “combination exercise” insofar as it checks a lot of boxes, e.g:
- Strength—especially core strength, but also limbs
- Mobility—range of motion and resultant reduction in injury risk
- Stability—impossible without the above two things, but Pilates trains this too
- Fitness—many dynamic Pilates exercises can be performed as cardio and/or HIIT.
The author, a physiotherapist, explains (as the title promises!) the science of Pilates, with:
- the beautifully clear diagrams we’ve come to expect of this series,
- equally clear explanations, with a great balance of simplicity of terms and depth where necessary, and
- plenty of citations for the claims made, linking to lots of the best up-to-date science.
Bottom line: if you are in a position to make a little time for Pilates (if you don’t already), then there is nobody who would not benefit from reading this book.
Click here to check out Science of Pilates, and keep your body well!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Over 50? Do These 3 Stretches Every Morning To Avoid Pain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Will Harlow, over-50s specialist physiotherapist, recommends these three stretches be done daily for cumulative benefits over time, especially if you have arthritis, stiff joints, or similar morning pain:
The good-morning routine
These stretches are designed for people with arthritis and stiff joints, but if you experience any extra pain, or are aware of having some musculoskeletal irregularity, do seek professional advice (such as from a local physiotherapist). Otherwise, the three stretches he recommends are:
Quad hip flexor stretch
This one is performed while lying on your side in bed:
- Bring the top leg up toward your body, grab the shin, and pull the leg backward to stretch.
- Feel the stretch in the front of the leg (quadriceps and hip flexor).
- Hold for 30 seconds and repeat on both sides.
- Use a towel or band if you can’t reach your shin.
Book-opener
This one helps improve mobility in the lower and mid-back:
- Lie on your side with arms at a 90-degree angle in front of your body.
- Roll backward, opening the top arm while keeping legs in place.
- Hold for 20–30 seconds or repeat the movement several times.
- Optionally, allow your head to rotate for a neck stretch.
Calf stretch with chest-opener
This one combines a calf and chest stretch:
- Stand in a lunged position, keeping the back leg straight and heel down for the calf stretch.
- Place hands behind your head, open elbows, and lift your head slightly for a chest stretch.
- Hold for 20–30 seconds, then switch legs.
For more on all the above plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: