Want the health benefits of strength training but not keen on the gym? Try ‘exercise snacking’
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The science is clear: resistance training is crucial to ageing well. Lifting weights (or doing bodyweight exercises like lunges, squats or push-ups) can help you live independently for longer, make your bones stronger, reduce your risk of diseases such as diabetes, and may even improve your sleep and mental health.
But not everyone loves the gym. Perhaps you feel you’re not a “gym person” and never will be, or you’re too old to start. Being a gym-goer can be expensive and time-consuming, and some people report feeling unwelcome or awkward at the gym.
The good news is you don’t need the gym, or lots of free time, to get the health benefits resistance training can offer.
You can try “exercise snacking” instead.

What is exercise snacking?
Exercise snacking involves doing multiple shorter bouts (as little as 20 seconds) of exercise throughout the day – often with minimal or no equipment. It’s OK to have several hours of rest between.
You could do simple bodyweight exercises such as:
- chair sit-to-stand (squats)
- lunges
- box step-ups
- calf raises
- push-ups.
Exercise snacking like this can help improve muscle mass, strength and physical function.
It’s OK to hold onto a nearby object for balance, if you need. And doing these exercises regularly will also improve your balance. That, in turn, reduces your risk of falls and fractures.
OK I have done all those, now what?
Great! You can also try using resistance bands or dumbbells to do the previously mentioned five exercises as well as some of the following exercises:
When using resistance bands, make sure you hold them tightly and that they’re securely attached to an immovable object.
Exercise snacking works well when you pair it with an activity you do often throughout the day. Perhaps you could:
- do a few extra squats every time you get up from a bed or chair
- do some lunges during a TV ad break
- chuck in a few half squats while you’re waiting for your kettle to boil
- do a couple of elevated push-ups (where you support your body with your hands on a chair or a bench while doing the push-up) before tucking into lunch
- sneak in a couple of calf raises while you’re brushing your teeth.

What does the evidence say about exercise snacking?
One study had older adults without a history of resistance training do exercise snacks at home twice per day for four weeks.
Each session involved five simple bodyweight exercises (chair sit-to-stand, seated knee extension, standing knee bends, marching on the spot, and standing calf raises). The participants did each exercise continuously for one minute, with a one-minute break between exercises.
These short and simple exercise sessions, which lasted just nine minutes, were enough to improve a person’s ability to stand up from a chair by 31% after four weeks (compared to a control group who didn’t exercise). Leg power and thigh muscle size improved, too.
Research involving one of us (Jackson Fyfe) has also shown older adults found “exercise snacking” feasible and enjoyable when done at home either once, twice, or three times per day for four weeks.
Exercise snacking may be a more sustainable approach to improve muscle health in those who don’t want to – or can’t – lift heavier weights in a gym.
A little can yield a lot
We know from other research that the more you exercise, the more likely it is you will keep exercising in future.
Very brief resistance training, albeit with heavier weights, may be more enjoyable than traditional approaches where people aim to do many, many sets.
We also know brief-and-frequent exercise sessions can break up periods of sedentary behaviour (which usually means sitting too much). Too much sitting increases your risk of chronic diseases such as diabetes, whereas exercise snacking can help keep your blood sugar levels steady.
Of course, longer-term studies are needed. But the evidence we do have suggests exercise snacking really helps.

Why does any of this matter?
As you age, you lose strength and mass in the muscles you use to walk, or stand up. Everyday tasks can become a struggle.
All this contributes to disability, hospitalisation, chronic disease, and reliance on community and residential aged care support.
By preserving your muscle mass and strength, you can:
- reduce joint pain
- get on with activities you enjoy
- live independently in your own home
- delay or even eliminate the need for expensive health care or residential aged care.
What if I walk a lot – is that enough?
Walking may maintain some level of lower body muscle mass, but it won’t preserve your upper body muscles.
If you find it difficult to get out of a chair, or can only walk short distances without getting out of breath, resistance training is the best way to regain some of the independence and function you’ve lost.
It’s even more important for women, as muscle mass and strength are typically lower in older women than men. And if you’ve been diagnosed with osteoporosis, which is more common in older women than men, resistance exercise snacking at home can improve your balance, strength, and bone mineral density. All of this reduces the risk of falls and fractures.
You don’t need heavy weights or fancy equipment to benefit from resistance training.
So, will you start exercise snacking today?
Justin Keogh, Associate Dean of Research, Faculty of Health Sciences and Medicine, Bond University and Jackson Fyfe, Senior Lecturer, Strength and Conditioning Sciences, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Getting COMFY – by Jordan Gross

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s easy to see how good “morning people” seem to have it; it’s harder, it seems, to become one.
And, if we’re forced by circumstance to be the morning person we’re not? We all-too-easily find ourselves greeting each coming day without the joy that, in an ideal world, we might.
So, is it possible to learn this power? Jordan Gross has it mapped out for it us…
The “COMFY” of the title is indeed an acronym, and it stands for:
- Calm
- Openness
- Movement
- Funny
- You
There’s a chapter explaining each in detail, and they’re bookended with other chapters explaining more about the whys and the hows.
As you might expect, the key to a good morning starts the night before, but there’s also a formula to follow. Of course, you can change it up, mix and match if you like… but this book provides a base framework to build from, which is something that can make a huge difference!
Bottom line: it’s a highly enjoyable book to read, and also provides genuine powerful help to bring us the brighter happier mornings we deserve—the set-up to the perfect day!
Click here to check out “Getting COMFY” and perk up your mornings—you deserve it!
Share This Post
-

Why Everyone You Don’t Like Is A Narcissist
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve written before about how psychiatry tends to name disorders after how they affect other people, rather than how they affect the bearer, and this is most exemplified when it comes to personality disorders. For example:
“You have a deep insecurity about never being good enough, and you constantly mess up in your attempt to overcompensate? You may have Evil Bastard Disorder!”
“You have a crippling fear of abandonment and that you are fundamentally unloveable, so you do all you can to try to keep people close? You must have Manipulative Bitch Disorder!”
See also: Miss Diagnosis: Anxiety, ADHD, & Women
Antisocial DiagnosesThese days, it is easy to find on YouTube countless videos of how to spot a narcissist, with a list of key traits that all mysteriously describe exactly the exes of everyone in the comments.
And these days it is mostly “narcissist”, because “psychopath” and “sociopath” have fallen out of popular favor a bit:
- perhaps for coming across as overly sensationalized, and thus lacking credibility
- perhaps because “Narcissistic Personality Disorder (NPD)” exists in the DSM-5 (the US’s latest “Diagnostic and Statistical Manual of Mental Disorders”), while psychopathy and sociopathy are not mentioned as existing.
You may be wondering: what do “psychopathy” and “sociopathy” mean?
And the answer is: they mean whatever the speaker wants them to mean. Their definitions and differences/similarities have been vigorously debated by clinicians and lay enthusiasts alike for long enough that the scientific world has pretty much given up on them and moved on.
Stigma vs pathology
Because of the popular media (and social media) representation of NPD, it is easy to armchair diagnose one’s relative/ex/neighbor/in-law/boss/etc as being a narcissist, because the focus is on “narcissists do these bad things that are mean to people”.
If the focus were instead on “narcissists have cripplingly low self-esteem, and are desperate to not show weakness in a world they have learned is harsh and predatory”, then there may not be so many armchair diagnoses—or at the very least, the labels may be attached with a little more compassion, the same way we might with other mental health issues such as depression.
Not that those with depression get an easy time of it socially either—society’s response is generally some manner of “aren’t you better yet, stop being lazy”—but at the very least, depressed people are not typically viewed with hatred.
A quick aside: if you or someone you know is struggling with depression, here are some things that actually help:
The Mental Health First-Aid You’ll Hopefully Never Need
The disorder is not the problem
Maybe your relative, ex, neighbor, etc really is clinically diagnosable as a narcissist. There are still two important things to bear in mind:
- After centuries of diagnosing people with mental health maladies that we now know don’t exist per se (madness, hysteria, etc), and in recent decades countless revisions to the DSM and similar tomes, thank goodness we now have the final and perfect set of definitions that surely won’t be re-written in the next few years or so ← this is irony; it will absolutely be re-written numerous times yet because of course it’s still not a magically perfect descriptor of the broad spectrum of human nature
- The disorder is not the problem; the way they treat (or have treated) you is the problem.
For example, let’s take a key thing generally attributed to narcissists: a lack of empathy
Now, empathy can be divided into:
- affective empathy: the ability to feel what other people are feeling
- cognitive empathy: the ability to intellectually understand what other people are feeling (akin to sympathy, which is the same but with the requisite of having experienced the thing in question oneself)
A narcissist (as well as various other people without NPD) will typically have negligible affective empathy, and their cognitive empathy may be a little sluggish too.
Sluggish = it may take them a beat longer than most people, to realize what an external signifier of emotions means, or correctly guess how something will be felt by others. This can result in gravely misspeaking (or inappropriately emoting), after failing to adequately quickly “read the room” in terms of what would be a socially appropriate response. To save face, they may then either deny/minimize the thing they just said/did, or double-down on it and go on [what for them feels like] the counterattack.
As to why this shutting off of empathy happens: they have learned that the world is painful, and that people are sources of pain, and so—to avoid further pain—have closed themselves off to that, often at a very early age. This will also apply to themselves; narcissists typically have negligible self-empathy too, which is why they will commonly make self-destructive decisions, even while trying to put themselves first.
Important note on how this impacts other people: the “Golden Rule” of “treat others as you would wish to be treated” becomes intangible, as they have no more knowledge of their own emotional needs than they do of anyone else’s, so cannot make that comparison.
Consider: if instead of being blind to empathy, they were colorblind… You would probably not berate them for buying green apples when you asked for red. They were simply incapable of seeing that, and consequently made a mistake. So it is when it’s a part of the brain that’s not working normally.
So… Since the behavior does adversely affect other people, what can be done about it? Even if “hate them for it and call for their eradication from the face of the Earth” is not a reasonable (or compassionate) option, what is?
Take the bull by the horns
Above all, and despite all appearances, a narcissist’s deepest desire is simply to be accepted as good enough. If you throw them a life-ring in that regard, they will generally take it.
So, communicate (gently, because a perceived attack will trigger defensiveness instead, and possibly a counterattack, neither of which are useful to anyone) what behavior is causing a problem and why, and ask them to do an alternative thing instead.
And, this is important, the alternative thing has to be something they are capable of doing. Not merely something that you feel they should be capable of doing, but that they are actually capable of doing.
- So not: “be a bit more sensitive!” because that is like asking the colorblind person to “be a bit more observant about colors”; they are simply not capable of it and it is folly to expect it of them, because no matter how hard they try, they can’t.
- But rather: “it upsets me when you joke about xyz; I know that probably doesn’t make sense to you and that’s ok, it doesn’t have to. I am asking, however, if you will please simply refrain from joking about xyz. Would you do that for me?”
Presented with such, it’s much more likely that the narcissist will drop their previous attempt to be good enough (by joking, because everyone loves someone with a sense of humor, right?) for a new, different attempt to be good enough (by showing “behold, look, I am a good person and doing the thing you asked, of which I am capable”).
That’s just one example, but the same methodology can be applied to most things.
For tricks pertaining to how to communicate such things without causing undue resistance, see:
Seriously Useful Communication Skills
Take care!
Share This Post
-

The Lost Art of Silence – by Sarah Anderson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
From “A Room Of One’s Own” to “Silent Mondays”, from spiritual retreats to noise-cancelling headphones, this book covers the many benefits of silence—and a couple of downsides too.
In an age where most things are available at the touch of a button, a little peaceful solitude can come at quite a premium, but what it offers can effect all manner of physical changes, from reduced stress responses to increased neurogenesis (growing new brain cells).
The tone throughout is a combination of personal and pop-science, and it’s very motivating to find a little more space-between-the-things in life.
The book is best enjoyed in a quiet room.
Bottom line: if you get the feeling sometimes that you could rest and recover fully and properly if you could just find the downtime, this book will help you find exactly that.
Click here to check out the Lost Art of Silence, and find peace and strength in it!
Share This Post

Related Posts
-
What Your Eyes Say About Your Health (If You Have A Mirror, You Can Do This Now!)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In an age when doctors are increasingly pressed to get you out of their office quickly and not take the time to do thorough tests, having a good basic knowledge of signs and symptoms of disease has become more important than ever for all of us:
The eyes have it:
Dr. Siobhan Deshauer is back, this time working with Dr. Maria Howard, a Canadian optometrist, who advised behind-the-scenes to ensure the best information about these signs and symptoms and what they tell us:
- Color blindness test: Ishihara color test identifies color blindness; in the version in the video, seeing “74” is normal, “12” indicates red-green color blindness, and no numbers suggest complete color blindness due to genetics or retinal/optic nerve issues.
- Yellow sclera (scleral icterus): yellow sclera indicates high bilirubin from excessive red blood cell breakdown, liver damage, bile duct blockage, or Gilbert syndrome.
- Blue sclera: indicates thin collagen in the sclera, which can be linked to osteogenesis imperfecta, Ehlers-Danlos syndrome, and Marfan syndrome.
- Pink eye: caused by infections, autoimmune diseases, or trauma; persistent symptoms or associated pain/vision changes need medical evaluation.
- Physiologic diplopia (double vision): normal test where fingers appear doubled when focusing on different planes; absence may indicate amblyopia.
- Pinhole test (visual acuity): looking through a small pinhole can determine if glasses are needed for clearer vision.
- Nearsighted vs farsighted: nearsightedness risks retinal tears and night vision issues, while farsightedness increases the risk of glaucoma.
- Eye color and health: brown eyes lower cancer risk but higher cataract risk; light eyes higher cancer risk but lower cataract risk; sudden changes may indicate a condition.
- Kayser-Fleischer rings: golden-brown rings around the iris suggest copper buildup from Wilson disease, treatable with chelation therapy.
- Corneal arcus: gray/white ring around the iris indicates cholesterol buildup, normal with aging but concerning in younger individuals, signaling hypercholesterolemia or artery narrowing.
- Limbal rings: dark rings around the iris are generally aesthetic and not health-related.
- Red desaturation test: a difference in red color perception between eyes may indicate optic nerve or retinal issues.
- Eye twitching: often linked to stress, sleep deprivation, or caffeine; persistent twitching or muscle involvement requires medical attention.
- Pupillary reflex: pupil constriction in light; abnormal responses suggest trauma, overdose, or poisoning.
- Cataracts: lens cloudiness due to age, UV exposure, smoking, diabetes, or prednisone; also occurs sometimes in youth due to conditions like diabetes.
- Yellow spots (pinguecula and pterygium): sun damage, wind, and dust exposure cause yellow spots; protect with sunglasses to prevent progression impacting vision.
- Dark spots in the eye: includes freckles, moles (nevi), and melanoma; changes require medical evaluation.
- Hypnotic induction profile: eye roll test assesses susceptibility to hypnosis.
- Floaters: normal clumps in the eye; sudden increases, flashes, or curtain-like effects may signal retinal detachment.
- Retinal detachment: caused by aging-related vitreous shrinkage; treated with lasers, gas bubbles, or retinal buckles.
- Macular degeneration (Amsler grid test): wavy, fuzzy lines or missing vision spots may indicate this condition.
- Giant cell arteritis: no, that’s not a typo: rather it is about blood vessel inflammation that can cause blindness; treated with prednisone, symptoms include headaches and vision changes.
- Near point of convergence: focus test to detect convergence issues common with excessive screen time.
- Blepharitis: eyelid inflammation causing itchiness, burning, or flaky skin; treated with hygiene, antibiotics, or tea tree oil.
- Proptosis (Graves’ disease): bulging eyes due to hyperthyroidism; treatable with medications, radiation, or surgery.
- Ptosis (droopy eyelids): indicates myasthenia gravis, temporarily improved with the ice pack test.
- Night vision issues: caused by retinal problems or high myopia, not typically vitamin A deficiency in developed countries.
- Dry eyes: caused by screen time, smoking, medications, or autoimmune diseases; managed with lubricating drops, reduced screen time, and adjustments.
- Watery eyes: caused by irritation or blocked tear ducts; treated with lubricating drops or surgery.
- Retinoblastoma: rare childhood cancer detectable through flash photography showing one white pupil; early detection enables treatment.
For more on all of these plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
What Your Hands Can Tell You About Your Health
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Coach’s Plan – by Mike Kavanagh
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A sports coach’s job is to prepare a plan, give it to the player(s), and hold them accountable to it. Change the strategy if needs be, call the shots. The job of the player(s) is then to follow those instructions.
If you have trouble keeping yourself accountable, Kavanagh argues that it can be good to separate how you approach things.
Not just “coach yourself”, but put yourself entirely in the coach’s shoes, as though you were a separate person, then switch back, and follow those instructions, trusting in your coach’s guidance.
The book also provides illustrative examples and guides the reader through some potential pitfalls—for example, what happens when morning you doesn’t want to do the things that evening you decided would be best?
The absolute backbone of this method is that it takes away the paralysing self-doubt that can occur when we second-guess ourselves mid-task.
In short, this book will fire up your enthusiasm and give you a reliable fall-back for when your motivation’s flagging.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
I’ve recovered from a cold but I still have a hoarse voice. What should I do?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cold, flu, COVID and RSV have been circulating across Australia this winter. Many of us have caught and recovered from one of these common upper respiratory tract infections.
But for some people their impact is ongoing. Even if your throat isn’t sore anymore, your voice may still be hoarse or croaky.
So what happens to the voice when we get a virus? And what happens after?
Here’s what you should know if your voice is still hoarse for days – or even weeks – after your other symptoms have resolved.
Why does my voice get croaky during a cold?
A healthy voice is normally clear and strong. It’s powered by the lungs, which push air past the vocal cords to make them vibrate. These vibrations are amplified in the throat and mouth, creating the voice we hear.
The vocal cords are two elastic muscles situated in your throat, around the level of your laryngeal prominence, or Adam’s apple. (Although everyone has one, it tends to be more pronounced in males.) The vocal cords are small and delicate – around the size of your fingernail. Any small change in their structure will affect how the voice sounds.
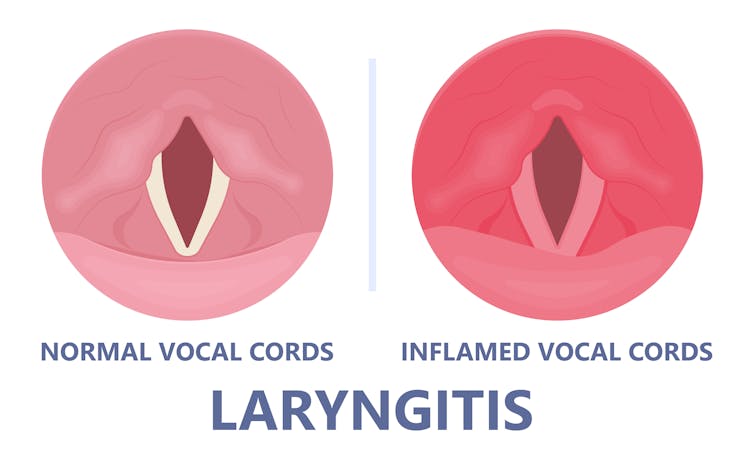
When the vocal cords become inflamed – known as laryngitis – your voice will sound different. Laryngitis is a common part of upper respiratory tract infections, but can also be caused through misuse.

Viruses such as the common cold can inflame the vocal cords. Pepermpron/Shutterstock Catching a virus triggers the body’s defence mechanisms. White blood cells are recruited to kill the virus and heal the tissues in the vocal cords. They become inflamed, but also stiffer. It’s harder for them to vibrate, so the voice comes out hoarse and croaky.
In some instances, you may find it hard to speak in a loud voice or have a reduced pitch range, meaning you can’t go as high or loud as normal. You may even “lose” your voice altogether.
Coughing can also make things worse. It is the body’s way of trying to clear the airways of irritation, including your own mucus dripping onto your throat (post-nasal drip). But coughing slams the vocal cords together with force.
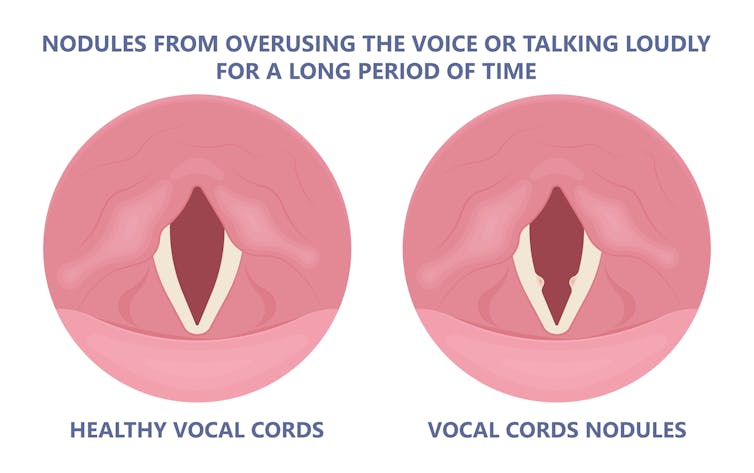
Chronic coughing can lead to persistent inflammation and even thicken the vocal cords. This thickening is the body trying to protect itself, similar to developing a callus when a pair of new shoes rubs.
Thickening on your vocal cords can lead to physical changes in the vocal cords – such as developing a growth or “nodule” – and further deterioration of your voice quality.
Coughing and exertion can cause inflamed vocal cords to thicken and develop nodules. Pepermpron/Shutterstock How can you care for your voice during infection?
People who use their voices a lot professionally – such as teachers, call centre workers and singers – are often desperate to resume their vocal activities. They are more at risk of forcing their voice before it’s ready.
The good news is most viral infections resolve themselves. Your voice is usually restored within five to ten days of recovering from a cold.
Occasionally, your pharmacist or doctor may prescribe cough suppressants to limit additional damage to the vocal cords (among other reasons) or mucolytics, which break down mucus. But the most effective treatments for viral upper respiratory tract infections are hydration and rest.
Drink plenty of water, avoid alcohol and exposure to cigarette smoke. Inhaling steam by making yourself a cup of hot water will also help clear blocked noses and hydrate your vocal cords.
Rest your voice by talking as little as possible. If you do need to talk, don’t whisper – this strains the muscles.
Instead, consider using “confidential voice”. This is a soft voice – not a whisper – that gently vibrates your vocal cords but puts less strain on your voice than normal speech. Think of the voice you use when communicating with someone close by.
During the first five to ten days of your infection, it is important not to push through. Exerting the voice by talking a lot or loudly will only exacerbate the situation. Once you’ve recovered from your cold, you can speak as you would normally.
What should you do if your voice is still hoarse after recovery?
If your voice hasn’t returned to normal after two to three weeks, you should seek medical attention from your doctor, who may refer you to an ear nose and throat specialist.
If you’ve developed a nodule, the specialist would likely refer you to a speech pathologist who will show you how to take care of your voice. Many nodules can be treated with voice therapy and don’t require surgery.
You may have also developed a habit of straining your vocal cords, if you forced yourself to speak or sing while they were inflamed. This can be a reason why some people continue to have a hoarse voice even when they’ve recovered from the cold.
In those cases, a speech pathologist may play a valuable role. They may teach you to exercises that make voicing more efficient. For example, lip trills (blowing raspberries) are a fun and easy way you can learn to relax the voice. This can help break the habit of straining your voice you may have developed during infection.
Yeptain Leung, Postdoctoral Research and Lecturer of Speech Pathology, School of Health Sciences, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: