Understanding and Responding to Self-Harm – by Dr. Allan House
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Whether it’s yourself, or (statistically much more likely) a loved one, it’s common to be faced with the deeply unpleasant reality of self-harm. This is a case where most definitely, “forewarned is forearmed”.
Dr. House covers not just the “what” and “why” of self-harm, but also the differences between suicidal and non-suicidal self-harm, as well as the impulsive and the planned.
Stylistically, the book is well-written, well-edited, and well-formatted. All this makes for easy reading and efficient learning.
Much of the book is, of course, given over to how to help in cases of self-harm. More specifically: how to approach things with both seriousness and compassion, and how to help in a way that doesn’t create undue pressure.
Because, as Dr. House explains and illustrates, a lot of well-meaning people end up causing more harm, by their botched attempts to help.
This book looks to avoid such tragedies.
Bottom line: if you’d rather know these things now, instead of wishing you’d known later, then this book is the one-stop guide it claims to be.
Click here to check out Understanding and Responding to Self-Harm, and be prepared!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:

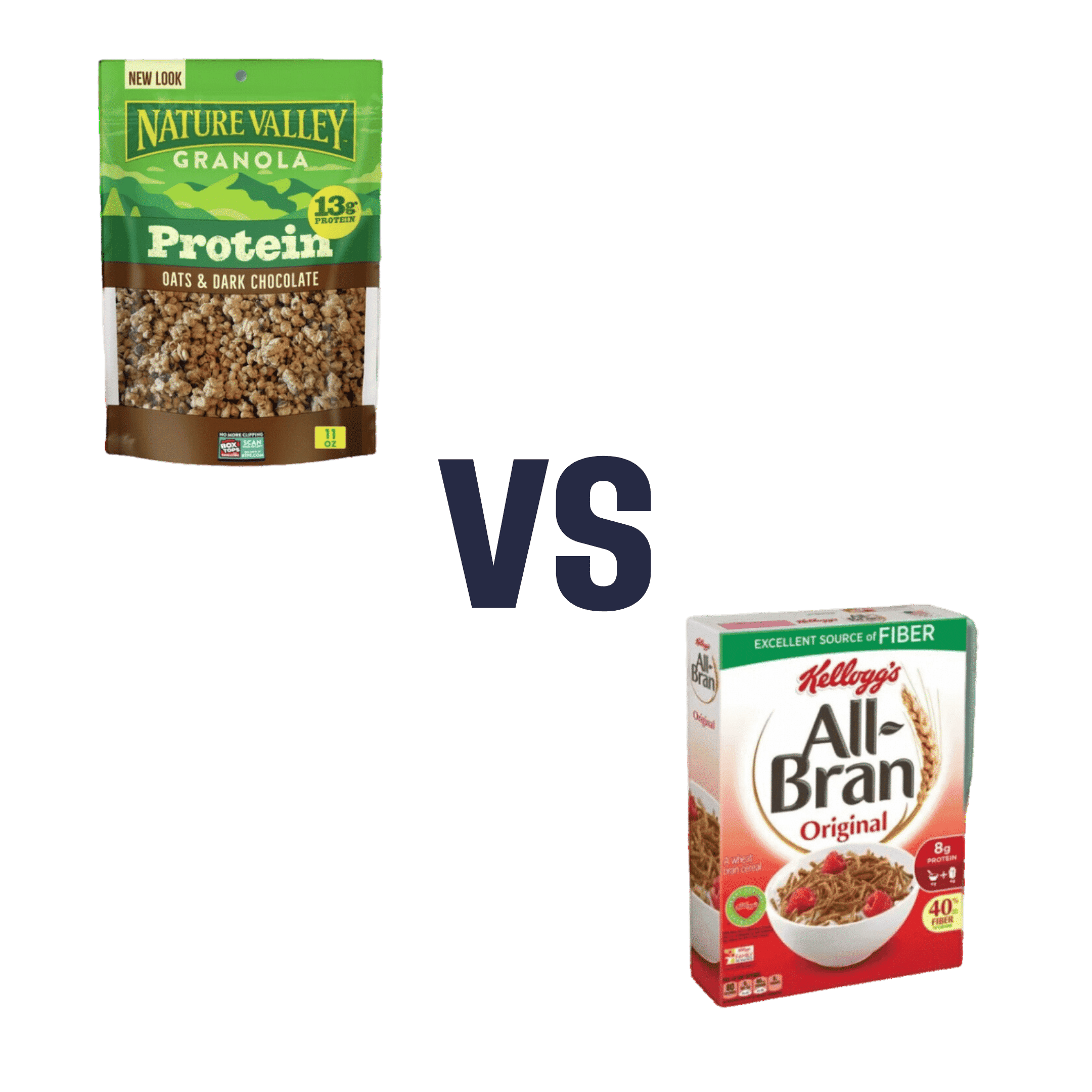
Nature Valley Protein Granola vs Kellog’s All-Bran – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing Nature Valley Protein Granola to Kellog’s All-Bran, we picked the All-Bran.
Why?
While the Protein Granola indeed contains more protein (13g/cup, compared to 5g/cup), it also contains three times as much sugar (18g/cup, compared to 9g/cup) and only ⅓ as much fiber (4g/cup, compared to 12g/cup)
Given that fiber is what helps our bodies to absorb sugar more gently (resulting in fewer spikes), this is extremely important, especially since 18g of sugar in one cup of Protein Granola is already most of the recommended daily allowance, all at once!
For reference: the AHA recommends no more than 25g added sugar for women, or 32g for men
Hence, we went for the option with 3x as much fiber and ⅓ of the sugar, the All-Bran.
For more about keeping blood sugars stable, see:
10 Ways To Balance Blood Sugars
Enjoy!
Share This Post

Synergistic Brain-Training
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Let The Games Begin (But It Matters What Kind)
Exercise is good for brain health; we’ve written about this before, for example:
How To Reduce Your Alzheimer’s Risk ← there are many advices here, but exercise, especially cardiovascular exercise in this case, is an important item on the list!
Today it’s Psychology Sunday though, and we’re going to talk about looking after brain health by means of brain-training, via games.
“Brain-training” gets a lot of hype and flak:
- Hype: do sudoku every day and soon you will have an IQ of 200 and still have a sharp wit at the age of 120
- Flak: brain-training is usually training only one kind of cognitive function, with limited transferability to the rest of life
The reality is somewhere between the two. Brain training really does improve not just outwardly measurable cognitive function, but also internally measurable improvements visible on brain scans, for example:
- Cognitive training modified age-related brain changes in older adults with subjective memory decline
- Functional brain changes associated with cognitive training in healthy older adults: A preliminary ALE meta-analysis
But what about the transferability?
Let us play
This is where game-based brain-training comes in. And, the more complex the game, the better the benefits, because there is more chance of applicability to life, e.g:
- Sudoku: very limited applicability
- Crosswords: language faculties
- Chess: spatial reasoning, critical path analysis, planning, memory, focus (also unlike the previous two, chess tends to be social for most people, and also involve a lot of reading, if one is keen)
- Computer games: wildly varied depending on the game. While an arcade-style “shoot-em-up” may do little for the brain, there is a lot of potential for a lot of much more relevant brain-training in other kinds of games: it could be planning, problem-solving, social dynamics, economics, things that mirror the day-to-day challenges of running a household, even, or a business.
- It’s not that the skills are useful, by the way. Playing “Stardew Valley” will not qualify you to run a real farm, nor will playing “Civilization” qualify you to run a country. But the brain functions used and trained? Those are important.
It becomes easily explicable, then, why these two research reviews with very similar titles got very different results:
- A Game a Day Keeps Cognitive Decline Away? A Systematic Review and Meta-Analysis of Commercially-Available Brain Training Programs in Healthy and Cognitively Impaired Older Adults
- Game-based brain training for improving cognitive function in community-dwelling older adults: A systematic review and meta-regression
The first review found that game-based brain-training had negligible actual use. The “games” they looked at? BrainGymmer, BrainHQ, CogMed, CogniFit, Dakim, Lumosity, and MyBrainTrainer. In other words, made-for-purpose brain-trainers, not actual computer games per se.
The second reviewfound that game-based training was very beneficial. The games they looked at? They didn’t name them, but based on the descriptions, they were actual multiplayer online turn-based computer games, not made-for-purpose brain-trainers.
To summarize the above in few words: multiplayer online turn-based computer games outperform made-for-purpose brain-trainers for cognitive improvement.
Bringing synergy
However, before you order that expensive gaming-chair for marathon gaming sessions (research suggests a tail-off in usefulness after about an hour of continuous gaming per session, by the way), be aware that cognitive training and (physical) exercise training combined, performed close in time to each other or simultaneously, perform better than the sum of either alone:
See also:
❝Simultaneous training was the most efficacious approach for cognition, followed by sequential combinations and cognitive training alone, and significantly better than physical exercise.
Our findings suggest that simultaneously and sequentially combined interventions are efficacious for promoting cognitive alongside physical health in older adults, and therefore should be preferred over implementation of single-domain training❞
~ Dr. Hanna Malmberg Gavelin et al.
Take care!
Share This Post

The Whys and Hows of Cutting Meats Out Of Your Diet
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it’s time to tell the meat to beat it…
Meat in general, and red meat and processed meat in particular, have been associated with so many health risks, that it’s very reasonable to want to reduce, if not outright eliminate, our meat consumption.
First, in case anyone’s wondering “what health risks?”
The aforementioned culprits tend to turn out to be a villain in the story of every second health-related thing we write about here. To name just a few:
- Processed Meat Consumption and the Risk of Cancer: A Critical Evaluation of the Constraints of Current Evidence from Epidemiological Studies
- Red Meat Consumption (Heme Iron Intake) and Risk for Diabetes and Comorbidities?
- Health Risks Associated with Meat Consumption: A Review of Epidemiological Studies
- Associations of Processed Meat, Unprocessed Red Meat, Poultry, or Fish Intake With Incident Cardiovascular Disease and All-Cause Mortality
- Meat consumption: Which are the current global risks? A review of recent (2010-2020) evidences
Seasoned subscribers will know that we rarely go more than a few days without recommending the very science-based Mediterranean Diet which studies find beneficial for almost everything we write about. The Mediterranean Diet isn’t vegetarian per se—by default it consists of mostly plants but does include some fish and a very small amount of meat from land animals. But even that can be improved upon:
- A Pesco-Mediterranean Diet With Intermittent Fasting
- Mediterranean, vegetarian and vegan diets as practical outtakes of EAS and ACC/AHA recommendations for lowering lipid profile
- A Mediterranean Low-Fat Vegan Diet to Improve Body Weight and Cardiometabolic Risk Factors: A Randomized, Cross-over Trial
So that’s the “why”; now for the “how”…
It’s said that with a big enough “why” you can always find a “how”, but let’s make things easy!
Meatless Mondays
One of the biggest barriers to many people skipping the meat is “what will we even eat?”
The idea of “Meatless Mondays” means that this question need only be answered once a week, and in doing that a few Mondays in a row, you’ll soon find you’re gradually building your repertoire of meatless meals, and finding it’s not so difficult after all.
Then you might want to expand to “meat only on the weekends”, for example.
Flexitarian
This can be met with derision, “Yes and I’m teetotal, apart from wine”, but there is a practical aspect here:
The idea is “I will choose vegetarian options, unless it’s really inconvenient for me to do so”, which wipes out any difficulty involved.
After doing this for a while, you might find that as you get more used to vegetarian stuff, it’s almost never inconvenient to eat vegetarian.
Then you might want to expand it to “I will choose vegan options, unless it’s really inconvenient for me to do so”
Like-for-like substitutions
Pretty much anything that can come from an animal, one can get a plant-based version of it nowadays. The healthiness (and cost!) of these substitutions can vary, but let’s face it, meat is neither the healthiest nor the cheapest thing out there these days either.
If you have the money and don’t fancy leaping to lentils and beans, this can be a very quick and easy zero-effort change-over. Then once you’re up and running, maybe you can—at your leisure—see what all the fuss is about when it comes to tasty recipes with lentils and beans!
That’s all we have time for today, but…
We’re thinking of doing a piece making your favorite recipes plant-based (how to pick the right substitutions so the meal still tastes and “feels” the same), so let us know if you’d like that? Feel free to mention your favorite foods/meals too, as that’ll help us know what there’s a market for!
You can do that by hitting reply to any of our emails, or using the handy feedback widget at the bottom!
Curious to know more while you wait?
Check out: The Vegan Diet: A Complete Guide for Beginners ← this is a well-sourced article from Healthline, who—just like us—like to tackle important health stuff in an easy-to-read, well-sourced format
Share This Post
Related Posts

The Osteoporosis Breakthrough – by Dr. Doug Lucas
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Osteoporosis” and “break” often don’t go well together, but here they do. So, what’s the breakthrough here?
There isn’t one, honestly. But if we overlook the marketing choices and focus on the book itself, the content here is genuinely good:
The book offers a comprehensive multivector approach to combatting osteoporosis, e.g:
- Diet
- Exercise
- Other lifestyle considerations
- Supplements
- Hormones
- Drugs
The author considers drugs a good and important tool for some people with osteoporosis, but not most. The majority of people, he considers, will do better without drugs—by tackling things more holistically.
The advice here is sound and covers all reasonable angles without getting hung up on the idea of there being a single magical solution for all.
Bottom line: if you’re looking for a book that’s a one-stop-shop for strategies against osteoporosis, this is a good option.
Click here to check out The Osteoporosis Breakthrough, and keep your bones strong!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:

Omega-3 Mushroom Spaghetti
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The omega-3 is not the only healthy fat in here; we’re also going to have medium-chain triglycerides, as well as monounsaturates. Add in the ergothioneine from the mushrooms and a stack of polyphenols from, well, most of the ingredients, not to mention the fiber, and this comes together as a very healthy dish. There’s also about 64g protein in the entire recipe, so you do the math for how much that is per serving, depending on how big you want the servings to be.
You will need
- 1lb wholewheat spaghetti (or gluten-free equivalent, such as a legume-based pasta, if avoiding gluten/wheat)
- 12oz mushrooms, sliced (any non-poisonous edible variety)
- ½ cup coconut milk
- ½ onion, finely chopped
- ¼ cup chia seeds
- ¼ bulb garlic, minced (or more, if you like)
- 2 tbsp extra virgin olive oil
- 1 tbsp black pepper, coarse ground
- 1 tbsp lime juice
Method
(we suggest you read everything at least once before doing anything)
1) Cook the spaghetti according to packet instructions, or your own good sense, aiming for al dente. When it’s done, drain it, and lastly rinse it (with cold water), and set it aside.
2) Heat the olive oil in a skillet and add the onion, cooking for 5 minutes
3) Add the garlic, mushrooms, and black pepper, cooking for another 8 minutes.
4) Add the coconut milk, lime juice, and chia seeds, stirring well and cooking for a further two minutes
5) Reheat the spaghetti by passing boiling water through it in a colander (the time it spent cold was good for it; it lowered the glycemic index)
6) Serve, adding the mushroom sauce to the spaghetti:

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- The Magic of Mushrooms: “The Longevity Vitamin” (That’s Not A Vitamin)
- The Many Health Benefits of Garlic
- Black Pepper’s Impressive Anti-Cancer Arsenal (And More)
- If You’re Not Taking Chia, You’re Missing Out
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
Margarine vs Butter – Which is Healthier
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing margarine to butter, we picked the butter.
Why?
Once upon a time, when margarines were filled with now-banned trans fats, this would have been an easy win for butter.
Nowadays, the macronutrient/lipid profiles are generally more similar (although margarine often has a little less saturated fat), except one thing that butter has in its favor:
More micronutrients. What exactly they are (and how much) depends on the diet and general health of the cows from whom the milk to make the butter came, but they’re not something found in plant-based butter alternatives at this time.
Nevertheless, because of the saturated fat content, it’s not advisable to use more than a very small amount of either (two tablespoons of butter would put one at the daily limit already, without eating any other saturated fat that day).
Read more: Butter vs Margarine
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: