To Pee Or Not To Pee
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Is it “strengthening” to hold, or are we doing ourselves harm if we do? Dr. Heba Shaheed explains in this short video:
A flood of reasons not to hold
Humans should urinate 4–6 times daily, but for many people, the demands of modern life often lead to delaying urination, raising questions about its effects on the body.
So first, let’s look at how it all works: the bladder is part of the urinary system, which includes the kidneys, ureters, urethra, and sphincters. Urine is produced by the kidneys and transported via the ureters into the bladder, a hollow organ with a muscular wall. This muscle (called the detrusor) allows the bladder to inflate as it fills with urine (bearing in mind, the main job of any muscle is to be able to stretch and contract).
As the bladder fills, stretch receptors in that muscle signal fullness to the spinal cord. This triggers the micturition reflex, causing the detrusor to contract and the internal urethral sphincter to open involuntarily. Voluntary control over the external urethral sphincter allows a person to delay or release urine as needed.
So, at what point is it best to go forth and pee?
For most people, bladder fullness is first noticeable at around 150-200ml, with discomfort occurring at 400-500ml (that’s about two cups*). Although the bladder can stretch to hold up to a liter, exceeding this capacity can cause it to rupture, a rare but serious condition requiring surgical intervention.
*note, however, that this doesn’t necessarily mean that drinking two cups will result in two cups being in your bladder; that’s not how hydration works. Unless you are already perfectly hydrated, most if not all of the water will be absorbed into the rest of your body where it is needed. Your bladder gets filled when your body has waste products to dispose of that way, and/or is overhydrated (though overhydration is not very common).
Habitually holding urine and/or urinating too quickly (note: not “too soon”, but literally, “too quickly”, we’re talking about the velocity at which it exits the body) can weaken pelvic floor muscles over time. This can lead to bladder pain, urgency, incontinence, and/or a damaged pelvic floor.
In short: while the body’s systems are equipped to handle occasional delays, holding it regularly is not advisable. For the good of your long-term urinary health, it’s best to avoid straining the system and go whenever you feel the urge.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Keeping your kidneys happy: it’s more than just hydration!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Happy Mind, Happy Life – by Dr. Rangan Chatterjee

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Let’s start with a “why”. If happiness doesn’t strike you as a worthwhile goal in and of itself, Dr. Chatterjee discusses the health implications of happiness/unhappiness.
And, yes, including in studies where other factors were controlled for, so he shows how happiness/unhappiness does really have a causal role in health—it’s not just a matter of “breaking news: sick people are less happy”.
The author, a British GP (General Practitioner, the equivalent of what the US calls a “family doctor”) with decades of experience, has found a lot of value in the practice of holistic medicine. For this reason, it’s what he recommends to his patients at work, in his books, his blog, and his regular spot on a popular BBC breakfast show.
The writing style is relaxed and personable, without skimping on information density. Indeed, Dr. Chatterjee offers many pieces of holistic health advice, and dozens of practical exercises to boost your happiness and proof you against adversity.
Because, whatever motivational speakers may say, we can’t purely “think ourselves happy”; sometimes we have real external threats and bad things in life. But, we can still improve our experience of even these things, not to mention suffer less, and get through it in better shape with a smile at the end of it.
Bottom line: if you’d like to be happier and healthier (who wouldn’t?), then this book is a sure-fire way to set you on that path.
Click here to check out Happy Mind, Happy Life and upgrade yours!
Share This Post
-

Natto vs Tofu – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing nattō to tofu, we picked the nattō.
Why?
In other words, in the comparison of fermented soy to fermented soy, we picked the fermented soy. But the relevant difference here is that nattō is fermented whole soybeans, while tofu is fermented soy milk of which the coagulated curds are then compressed into a block—meaning that the nattō is the one that has “more food per food”.
Looking at the macros, it’s therefore no surprise that nattō has a lot more fiber to go with its higher carb count; it also has slightly more protein. You may be wondering what tofu has more of, and the answer is: water.
In terms of vitamins, nattō has more of vitamins B2, B4, B6, C, E, K, and choline, while tofu has more of vitamins A, B3, and B9. So, a 7:3 win for nattō, even before considering that that vitamin C content of nattō is 65x more than what tofu has.
When it comes to minerals, nattō has more copper, iron, magnesium, manganese, potassium, and zinc, while tofu has more calcium, phosphorus, and selenium. So, a 6:3 win for nattō, and yes, the margins of difference are comparable (being 2–3x more for most of these minerals).
In short, both of these foods are great, but nattō is better.
Want to learn more?
You might like to read:
21% Stronger Bones in a Year at 62? Yes, It’s Possible (No Calcium Supplements Needed!)
Take care!
Share This Post
-
Why do I need to take some medicines with food?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Have you ever been instructed to take your medicine with food and wondered why? Perhaps you’ve wondered if you really need to?
There are varied reasons, and sometimes complex science and chemistry, behind why you may be advised to take a medicine with food.
To complicate matters, some similar medicines need to be taken differently. The antibiotic amoxicillin with clavulanic acid (sold as Amoxil Duo Forte), for example, is recommended to be taken with food, while amoxicillin alone (sold as Amoxil), can be taken with or without food.
Different brands of the same medicine may also have different recommendations when it comes to taking it with food.

Ron Lach/Pexels Food impacts drug absorption
Food can affect how fast and how much a drug is absorbed into the body in up to 40% of medicines taken orally.
When you have food in your stomach, the makeup of the digestive juices change. This includes things like the fluid volume, thickness, pH (which becomes less acidic with food), surface tension, movement and how much salt is in your bile. These changes can impair or enhance drug absorption.
Eating a meal also delays how fast the contents of the stomach move into the small intestine – this is known as gastric emptying. The small intestine has a large surface area and rich blood supply – and this is the primary site of drug absorption.
Eating a meal with medicine will delay its onset. Farhad/Pexels Eating a larger meal, or one with lots of fibre, delays gastric emptying more than a smaller meal. Sometimes, health professionals will advise you to take a medicine with food, to help your body absorb the drug more slowly.
But if a drug can be taken with or without food – such as paracetamol – and you want it to work faster, take it on an empty stomach.
Food can make medicines more tolerable
Have you ever taken a medicine on an empty stomach and felt nauseated soon after? Some medicines can cause stomach upsets.
Metformin, for example, is a drug that reduces blood glucose and treats type 2 diabetes and polycystic ovary syndrome. It commonly causes gastrointestinal symptoms, with one in four users affected. To combat these side effects, it is generally recommended to be taken with food.
The same advice is given for corticosteroids (such as prednisolone/prednisone) and certain antibiotics (such as doxycycline).
Taking some medicines with food makes them more tolerable and improves the chance you’ll take it for the duration it’s prescribed.
Can food make medicines safer?
Ibuprofen is one of the most widely used over-the-counter medicines, with around one in five Australians reporting use within a two-week period.
While effective for pain and inflammation, ibuprofen can impact the stomach by inhibiting protective prostaglandins, increasing the risk of bleeding, ulceration and perforation with long-term use.
But there isn’t enough research to show taking ibuprofen with food reduces this risk.
Prolonged use may also affect kidney function, particularly in those with pre-existing conditions or dehydration.
The Australian Medicines Handbook, which guides prescribers about medicine usage and dosage, advises taking ibuprofen (sold as Nurofen and Advil) with a glass of water – or with a meal if it upsets your stomach.
If it doesn’t upset your stomach, ibuprofen can be taken with water. Tbel Abuseridze/Unsplash A systematic review published in 2015 found food delays the transit of ibuprofen to the small intestine and absorption, which delays therapeutic effect and the time before pain relief. It also found taking short courses of ibuprofen without food reduced the need for additional doses.
To reduce the risk of ibuprofen causing damage to your stomach or kidneys, use the lowest effective dose for the shortest duration, stay hydrated and avoid taking other non-steroidal anti-inflammatory medicines at the same time.
For people who use ibuprofen for prolonged periods and are at higher risk of gastrointestinal side effects (such as people with a history of ulcers or older adults), your prescriber may start you on a proton pump inhibitor, a medicine that reduces stomach acid and protects the stomach lining.
How much food do you need?
When you need to take a medicine with food, how much is enough?
Sometimes a full glass of milk or a couple of crackers may be enough, for medicines such as prednisone/prednisolone.
However, most head-to-head studies that compare the effects of a medicine “with food” and without, usually use a heavy meal to define “with food”. So, a cracker may not be enough, particularly for those with a sensitive stomach. A more substantial meal that includes a mix of fat, protein and carbohydrates is generally advised.
Your health professional can advise you on which of your medicines need to be taken with food and how they interact with your digestive system.
Mary Bushell, Clinical Associate Professor in Pharmacy, University of Canberra
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



-

Healing Trauma – by Dr. Peter Levine
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Levine’s better-selling book about trauma, Waking The Tiger, laid the foundations for this one, but the reason we’re skipping straight into Healing Trauma, is that while the former book is more about the ideas that led him to what he currently believes is the best approach to healing trauma, this book is the one that explains how to actually do it.
The core thesis is that trauma is a natural, transient response, and is not inherently pathological, but that it can become so if not allowed to do its thing.
This book outlines exercises, trademarked as “somatic experiencing”, which allow the body to go through the physiological processes it needs to, to facilitate healing. If you buy the physical book, there is also an audio CD, which this reviewer has not listened to and cannot comment on, but the exercises are clearly described in the book in any case.
The physical aspects of the exercises are similar to the principles of progressive relaxation, while the mental aspects of the exercises are about re-experiencing trauma in a safer fashion, in small doses.
Any kind of dealing with trauma is not going to be comfortable, so this book is not an enjoyable read.
As for how useful the exercises are, your mileage may vary. Like many books about trauma, the expectation is that once upon a time you were in a situation that was unsafe, and now you are safe. If that describes your trauma, you will get the most out of this. However, if your trauma is unrelated to your personal safety, or if it is about your personal safety but the threat still remains extant, then a lot of this may not help and may even make things worse.
In terms of discussing sexual trauma specifically, it was probably not a good choice to favorably quote Woody Allen, and little things like that may be quite jarring for a lot of readers.
Bottom line: if your trauma is PTSD of the kind “you faced an existential threat and now it is gone”, then chances are that this book can help you a lot. If your trauma is different, then your mileage may vary widely on this one.
Click here to check out Healing Trauma, if it seems right for you!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What’s the difference between shyness and social anxiety?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
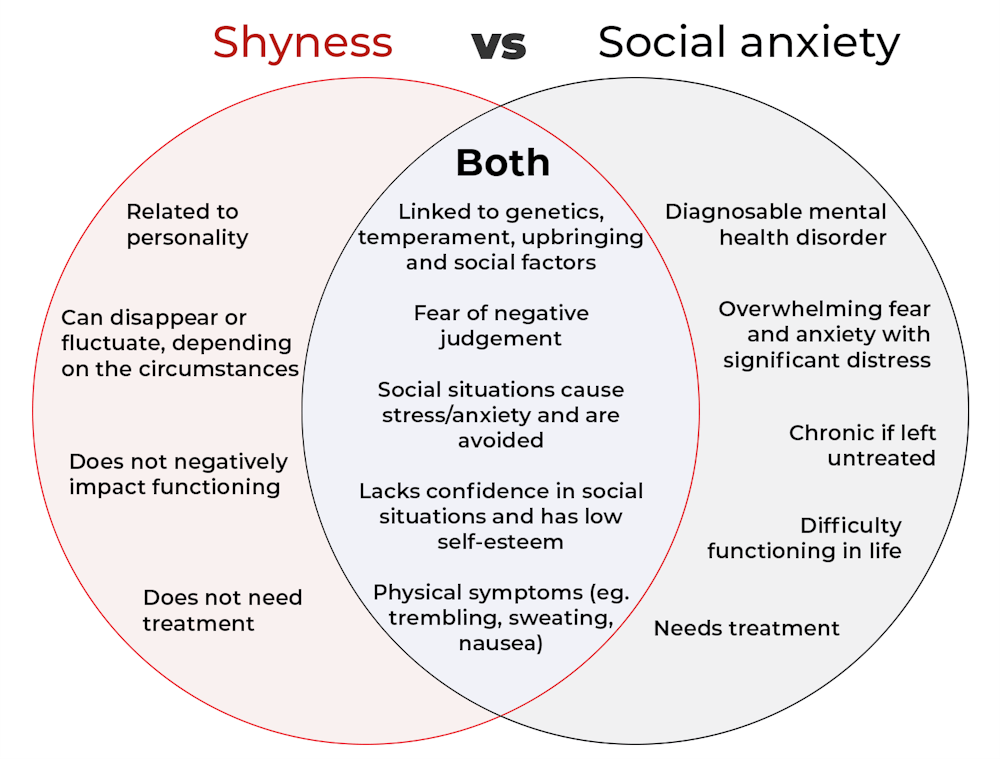
The terms “shyness” and “social anxiety” are often used interchangeably because they both involve feeling uncomfortable in social situations.
However, feeling shy, or having a shy personality, is not the same as experiencing social anxiety (short for “social anxiety disorder”).
Here are some of the similarities and differences, and what the distinction means.
pathdoc/Shutterstock How are they similar?
It can be normal to feel nervous or even stressed in new social situations or when interacting with new people. And everyone differs in how comfortable they feel when interacting with others.
For people who are shy or socially anxious, social situations can be very uncomfortable, stressful or even threatening. There can be a strong desire to avoid these situations.
People who are shy or socially anxious may respond with “flight” (by withdrawing from the situation or avoiding it entirely), “freeze” (by detaching themselves or feeling disconnected from their body), or “fawn” (by trying to appease or placate others).
A complex interaction of biological and environmental factors is also thought to influence the development of shyness and social anxiety.
For example, both shy children and adults with social anxiety have neural circuits that respond strongly to stressful social situations, such as being excluded or left out.
People who are shy or socially anxious commonly report physical symptoms of stress in certain situations, or even when anticipating them. These include sweating, blushing, trembling, an increased heart rate or hyperventilation.
How are they different?
Social anxiety is a diagnosable mental health condition and is an example of an anxiety disorder.
For people who struggle with social anxiety, social situations – including social interactions, being observed and performing in front of others – trigger intense fear or anxiety about being judged, criticised or rejected.
To be diagnosed with social anxiety disorder, social anxiety needs to be persistent (lasting more than six months) and have a significant negative impact on important areas of life such as work, school, relationships, and identity or sense of self.
Many adults with social anxiety report feeling shy, timid and lacking in confidence when they were a child. However, not all shy children go on to develop social anxiety. Also, feeling shy does not necessarily mean a person meets the criteria for social anxiety disorder.
People vary in how shy or outgoing they are, depending on where they are, who they are with and how comfortable they feel in the situation. This is particularly true for children, who sometimes appear reserved and shy with strangers and peers, and outgoing with known and trusted adults.
Individual differences in temperament, personality traits, early childhood experiences, family upbringing and environment, and parenting style, can also influence the extent to which people feel shy across social situations.
Not all shy children go on to develop social anxiety. 249 Anurak/Shutterstock However, people with social anxiety have overwhelming fears about embarrassing themselves or being negatively judged by others; they experience these fears consistently and across multiple social situations.
The intensity of this fear or anxiety often leads people to avoid situations. If avoiding a situation is not possible, they may engage in safety behaviours, such as looking at their phone, wearing sunglasses or rehearsing conversation topics.
The effect social anxiety can have on a person’s life can be far-reaching. It may include low self-esteem, breakdown of friendships or romantic relationships, difficulties pursuing and progressing in a career, and dropping out of study.
The impact this has on a person’s ability to lead a meaningful and fulfilling life, and the distress this causes, differentiates social anxiety from shyness.
Children can show similar signs or symptoms of social anxiety to adults. But they may also feel upset and teary, irritable, have temper tantrums, cling to their parents, or refuse to speak in certain situations.
If left untreated, social anxiety can set children and young people up for a future of missed opportunities, so early intervention is key. With professional and parental support, patience and guidance, children can be taught strategies to overcome social anxiety.
Why does the distinction matter?
Social anxiety disorder is a mental health condition that persists for people who do not receive adequate support or treatment.
Without treatment, it can lead to difficulties in education and at work, and in developing meaningful relationships.
Receiving a diagnosis of social anxiety disorder can be validating for some people as it recognises the level of distress and that its impact is more intense than shyness.
A diagnosis can also be an important first step in accessing appropriate, evidence-based treatment.
Different people have different support needs. However, clinical practice guidelines recommend cognitive-behavioural therapy (a kind of psychological therapy that teaches people practical coping skills). This is often used with exposure therapy (a kind of psychological therapy that helps people face their fears by breaking them down into a series of step-by-step activities). This combination is effective in-person, online and in brief treatments.
Treatment is available online as well as in-person. ImYanis/Shutterstock For more support or further reading
Online resources about social anxiety include:
- This Way Up’s online program for managing excessive shyness and fear of social situations
- Beyond Blue’s resources on social anxiety
- a guide to looking after yourself if you have social anxiety, from the Western Australian health department
- social anxiety online program for children and teens from the University of Queensland
- inroads, a self-guided online program for young adults who drink alcohol to manage their anxiety.
We thank the Black Dog Institute Lived Experience Advisory Network members for providing feedback and input for this article and our research.
Kayla Steele, Postdoctoral research fellow and clinical psychologist, UNSW Sydney and Jill Newby, Professor, NHMRC Emerging Leader & Clinical Psychologist, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
How to survive extreme cold
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cold weather can be deadly, especially in places not used to extreme cold. A December 2024 study found that cold-related deaths have more than doubled between 1999 and 2022, with over 3,500 deaths reported in 2022.
Climate change doesn’t only mean rising temperatures; it also causes extreme weather, including extreme cold.
The Cybersecurity and Infrastructure Security Agency defines extreme cold as “temperatures that are lower than historical averages to the point that it creates a dangerous environment for people, animals, and critical infrastructure.”
“There’s rightfully been a focus on heat deaths because of the context of global warming. But both can be true,” said Michael Liu, the study’s lead author, in a Washington Post article. “Cold-related deaths are still a public health risk.”
Cold weather-related injuries and deaths are preventable. Preparing ahead of time ensures you can stay safe when cold weather hits.
Stay informed
Following local news and weather reports will keep you aware of extreme weather in your area so you can plan accordingly. Many state and local governments provide emergency text and mobile app alert services.
The National Weather Service automatically sends English and Spanish Wireless Emergency Alerts related to weather emergencies to compatible cell phones. Although iPhones, Androids, and most smartphones are WEA-compatible, you may need to check your device’s settings to ensure they are turned on.
Make a cold weather kit
When planning for cold weather, prepare for the worst-case scenario. Extremely cold temperatures, snow, and ice can cause power outages, frozen or burst pipes, loss of wireless and cell signals, and hazardous driving conditions.
A cold weather kit for your home should include:
- A flashlight with extra batteries
- A first-aid kit
- Extra water and non-perishable food to last a few days
- Baby supplies, such as diapers and formula to last a few days
- Pet supplies, such as food and litter to last a few days
- Warm clothes and blankets
- Sufficient amounts of your prescription medications and special medical equipment
You may also wish to add a battery-powered NOAA weather radio in your kit. These radios, which can be purchased for as little as $20, allow you to receive weather updates during power and internet outages.
Experts recommend staying indoors and avoiding driving in extreme cold. If you must drive, make sure your car has a cold weather kit before the winter. In addition to the equipment in a home cold weather kit, the National Weather Service suggests that a winter car survival kit also include:
- Jumper cables
- Cat litter or sand for tire traction
- Shovel
- Ice scraper
- Blankets/sleeping bag and warm clothes
- Hand warmers
- Charged cell phone with a spare charger
- Basic tool kit
Become familiar with warming centers
Many cities offer warming centers for people who need short-term shelter during cold weather. Check nearby centers’ locations, operating hours, and pet policies in advance. If your local warming centers don’t accept pets, other locations, like kennels and vet clinics, may temporarily board pets.
Learn how to use heating and power devices safely
Many deaths in cold weather are not from cold temperatures but from fires and carbon monoxide poisoning from improper use of heaters and generators.
All living spaces should be equipped with working smoke and carbon monoxide detectors, which should be tested monthly. Some fire departments provide free and low-cost detectors.
According to the Federal Emergency Management Agency, heaters are the second leading cause of house fires.
“Space heaters are involved in more than 1,000 home fires across the country every year and factor into the vast majority of home heating-related deaths,” said former Department Of Homeland Security Secretary Alejandro Mayorkas at FEMA’s 2024 #WinterReady Extreme Cold Summit.
Space heaters should never be left unattended, used around unsupervised children or pets, or left on overnight. They should be plugged directly into a power outlet, not power strips and extension cords. Additionally, they shouldn’t be operated on unstable or uneven surfaces.
The U.S. Fire Administration also recommends that you “keep anything that can burn at least 3 feet from all heat sources including fireplaces, wood stoves, radiators, space heaters or candles.”
Generators and portable coal- or gasoline-powered power stations can help you stay warm and maintain power during outages. However, these devices should never be used indoors, as they produce deadly carbon monoxide. Generators should be set up outdoors, at least 20 feet from vents, windows, and doors.
Carbon monoxide poisoning can also be a risk when trying to stay warm inside a vehicle. To avoid this, never leave your car running inside a garage, even if the door and windows are open.
For more information about cold weather resources, check with your local government and FEMA and the National Weather Service.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: