The Rise Of The Machines
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In this week’s health science news, several pieces of technology caught our eye. Let’s hope these things roll out widely!
When it comes to UTIs, antimicrobial resistance is taking the p—
This has implications far beyond UTIs—though UTIs can be a bit of a “canary in the coal mine” for antimicrobial resistance. The more people are using antibiotics (intentionally, or because they are in the food chain), the more killer bugs are proliferating instead of dying when we give them something to kill them. And yes: they do proliferate sometimes when given antibiotics, not because the antibiotics did anything directly good for them, but because they killed their (often friendly bacteria) competition. Thus making for a double-whammy of woe.
This development tackles that, by using AI modelling to crunch the numbers of a real-time data-driven personalized approach to give much more accurate treatment options, in a way that a human couldn’t (or at least, couldn’t at anything like the same speed, and most family physicians don’t have a mathematician locked in the back room to spend the night working on a patient’s data).
Read in full: AI can help tackle urinary tract infections and antimicrobial resistance
Related: AI: The Doctor That Never Tires?
When it comes to CPR and women, people are feint of heart
When CPR is needed, time is very much of the essence. And yet, bystanders are much less likely to give CPR to a woman than to a man. Not only that, but CPR-training is part of what leads to this reluctance when it comes to women: the mannequins used are very homogenous, being male (94%) and lean (99%). They’re also usually white (88%) even in countries where the populations are not, but that is less critical. After all, a racist person is less likely to give CPR to a person of color regardless of what color the training mannequin was.
However, the mannequins being male and lean is an issue, because it means people suddenly lack confidence when faced with breasts and/or abundant body fat. Both can prompt the bystander to wonder if some different technique is needed (it isn’t), and breasts can also prompt the bystander to fear doing something potentially “improper” (the proper course of action is: save a person’s life; do not get distracted by breasts).
Read in full: Women are less likely to receive CPR than men. Training on manikins with breasts could help ← there are also CPR instructions (and a video demonstration) there, for anyone who wants a refresher, if perhaps your last first-aid course was a while ago!
Related: Heart Attack: His & Hers (Be Prepared!)
When technology is a breath of fresh air
A woman with COPD and COVID has had her very damaged lungs replaced using a da Vinci X robot to perform a minimally-invasive surgery (which is quite a statement, when it comes to replacing someone’s lungs).
Not without human oversight though—surgeon Dr. Stephanie Chang was directing the transplant. Surgery is rarely fun for the person being operated on, but advances like this make things go a lot more smoothly, so this kind of progress is good to see.
Read in full: Woman receives world’s first robotic double-lung transplant
Related: Why Chronic Obstructive Pulmonary Disease (COPD) Is More Likely Than You Think
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Which Tea Is Best, By Science?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What kind of tea is best for the health?
It’s popular knowledge that tea is a healthful drink, and green tea tends to get the popular credit for “healthiest”.
Is that accurate? It depends on what you’re looking for…
Black
Its strong flavor packs in lots of polyphenols, often more than other kinds of tea. This brings some great benefits:
As well as effects beyond the obvious:
…and its cardioprotective benefits aren’t just about lowering blood pressure; it improves triglyceride levels as well as improving the LDL to HDL ratio:
The effect of black tea on risk factors of cardiovascular disease in a normal population
Finally (we could say more, but we only have so much room), black tea usually has the highest caffeine content, compared to other teas.
That’s good or bad depending on your own physiology and preferences, of course.
White
White tea hasn’t been processed as much as other kinds, so this one keeps more of its antioxidants, but that doesn’t mean it comes out on top; in this study of 30 teas, the white tea options ranked in the mid-to-low 20s:
White tea is also unusual in its relatively high fluoride content, which is consider a good thing:
White tea: A contributor to oral health
In case you were wondering about the safety of that…
Water Fluoridation: Is It Safe, And How Much Is Too Much?
Green
Green tea ranks almost as high as black tea, on average, for polyphenols.
Its antioxidant powers have given it a considerable anti-cancer potential, too:
- Green tea consumption and breast cancer risk or recurrence: a meta-analysis
- Green tea consumption and prostate cancer risk: a prospective study
…and many others, but you get the idea. Notably:
Green Tea Catechins: Nature’s Way of Preventing and Treating Cancer
…or to expand on that:
About green tea’s much higher levels of catechins, they also have a neuroprotective effect:
Green tea of course is also a great source of l-theanine, which we could write a whole main feature about, and we did:
Red
Also called “rooibos” or (literally translated from Afrikaans to English) “redbush”, it’s quite special in that despite being a “true tea” botanically and containing many of the same phytochemicals as the other teas, it has no caffeine.
There’s not nearly as much research for this as green tea, but here’s one that stood out:
However, in the search for the perfect cup of tea (in terms of phytochemical content), another set of researchers found:
❝The optimal cup was identified as sample steeped for 10 min or longer. The rooibos consumers did not consume it sufficiently, nor steeped it long enough. ❞
Read in full: Rooibos herbal tea: an optimal cup and its consumers
Bottom line
Black, white, green, and red teas all have their benefits, and ultimately the best one for you will probably be the one you enjoy drinking, and thus drink more of.
If trying to choose though, we offer the following summary:
- 🖤 Black tea: best for total beneficial phytochemicals
- 🤍 White tea:best for your oral health
- 💚 Green tea: best for your brain
- ❤️ Red tea: best if you want naturally caffeine-free
Enjoy!
Share This Post
-

Dealing With Hearing Loss
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hearing is important, not only for convenience, but also for cognitive health—as an inability to participate in what for most people is an important part of social life, has been shown to accelerate cognitive decline:
14 Powerful Strategies To Prevent Dementia ← one of them is looking after your hearing
To this end, we’ve written before about ways to retain (or at least slow the loss of) your hearing, here:
But, what if, despite our best efforts, your hearing is declining regardless, or is already impaired in some way?
Working with the hand we’ve been dealt
So, your hearing is bad and/or deteriorating. Assuming you’ve ruled out possibilities of fixing it, the next step is how to manage this new state of affairs.
One thing to seriously consider, sooner than you think you need to, is using hearing aids. This is because they will not only help you in the obvious practical way, but also, they will slow the associated decline of the parts of your brain that process the language you hear:
ACHIEVE study finds hearing aids cut cognitive decline by 48%
…and here’s the paper itself:
Furthermore, hearing aid use can significantly reduce all-cause mortality:
Your ears are not the only organs
Remember, today’s about dealing with hearing loss, not preventing it (for preventing it, see the second link we dropped up top).
With this in mind: do not underestimate the usefulness of learning to lipread.
Lipreading is not a panacea; it has its limitations:
- You can’t lipread an audio-only phonecall, or a podcast, or the radio
- You can’t lipread a video call if the video quality is poor
- You can’t lipread if someone is wearing a mask (as in many healthcare settings)
- You can’t lipread multiple people at once; you have to choose whose mouth to watch (or at least, you will miss the first word(s) each time while switching)
- You can’t lipread during sex if your/their face is somewhere else (may seem like a silly example, but actually communication can be important in sex, and the number of times this writer has had to say “Say again?” in intimate moments is ridiculous)
However, it can also make a huge difference the rest of the time, and can even be a superpower in times/places when other people’s hearing is nullified, such as a noisy environment, or a video call in which someone’s mic isn’t working.
The good news is, it’s really very easy to learn to lipread. There are many valid ways (often involving consciously memorizing mouth-shapes from charts, and then putting them together one by one to build a vocabulary), but this writer recommends a more organic, less effort-intensive approach:
- Choose a video of someone who speaks clearly, and for which video you already know what is being said (such as by using subtitles first, or a transcript, or perhaps the person is delivering a famous speech or reciting a poem that you know well, or it’s your favorite movie that you’ve watched many times).
- Now watch it with the sound off (assuming you do normally have some hearing; if you don’t, then you’re probably ahead of the game here) and just pay close attention to the lips. Do this on repeat; soon you’ll be able to “hear” the sounds as you see them made.
- Now choose a video of someone who speaks clearly, for which video you do not already know what is being said. You’ll probably only get parts of it at first; that’s ok.
- Now learn the rest of what they said in that video (by reading a transcript or such), and use it like you used the first video.
- Now repeat steps 3 and 4 until you are lipreading most people easily unless there is some clear obfuscation preventing you.
This process should not take long, as there are only about 44 phonemes (distinct sounds) in English, and once you’ve learned them, you’re set. If you speak more languages, those same 44 phonemes should cover most of most of them, but if not, just repeat the above process with the next language.
Remember, if you have at least some hearing, then most of the time your lipreading and your hearing are going to be working together, and neither will be as strong without the other—but if necessary, well-practised lipreading can indeed often stand in for hearing when hearing isn’t available.
A note on sign language:
Sign language is great, and cool, and useful. However, it’s only as useful as the people who know it, which means that it’s top-tier in the Deaf community (where people will dodge hearing-related cognitive decline entirely, because their social interaction is predominantly signed rather than spoken), and can be useful with close friends or family members who learn it (or at least learn some), but isn’t as useful in most of the wider world when people don’t know it. But if you do want to learn it, don’t let that hold you back—be the change you want to see!
Most of our readers are American, so here’s a good starting place for American Sign Language ← this is a list of mostly-free resources
Enjoy!
Share This Post
-
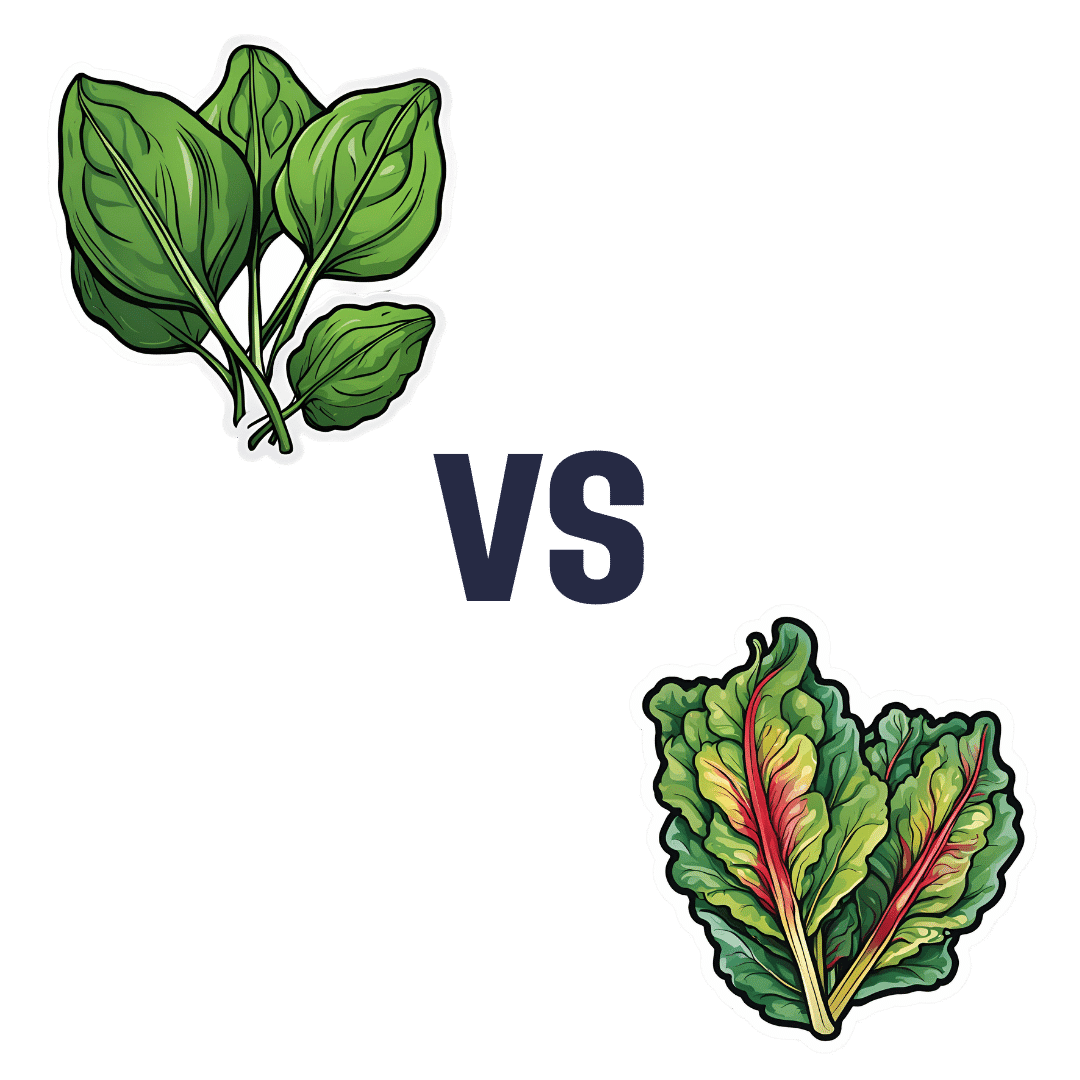
Spinach vs Chard – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing spinach to chard, we picked the spinach.
Why?
In terms of macros, spinach has slightly more fiber and protein, while chard has slightly more carbs. Now, those carbs are fine; nobody is getting metabolic disease from eating greens. But, by the numbers, this is a clear, albeit marginal, win for spinach.
In the category of vitamins, spinach has more of vitamins A, B1, B2, B3, B5, B6, B9, E, and K, while chard has more of vitamins C and choline. An even clearer victory for spinach this time.
When it comes to minerals, spinach has more calcium, copper, iron, magnesium, manganese, phosphorus, selenium, and zinc, while chard has more potassium. Once again, a clear win for spinach.
You may be wondering about oxalates, in which spinach is famously high. However, chard is nearly 2x higher in oxalates. In practical terms, this doesn’t mean too much for most people. If you have kidney problems or a family history of such, it is recommended to avoid oxalates. For everyone else, the only downside is that oxalates diminish calcium bioavailability, which is a pity, as spinach is (by the numbers) a good source of calcium.
However, oxalates are broken down by heat, so this means that cooked spinach (lightly steamed is fine; you don’t need to do anything drastic) will be much lower in oxalates (if you have kidney problems, do still check with your doctor/dietician, though).
All in all, spinach beats chard by most metrics, and by a fair margin. Still, enjoy either or both, unless you have kidney problems, in which case maybe go for kale or collard greens instead!
Want to learn more?
You might like to read:
Make Your Vegetables Work Better Nutritionally ← includes a note on breaking down oxalates, and lots of other information besides!
Enjoy!
Share This Post

Related Posts
-
Banana Bread vs Bagel – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing banana bread to bagel, we picked the bagel.
Why?
Unlike most of the items we compare in this section, which are often “single ingredient” or at least highly standardized, today’s choices are rather dependent on recipe. Certainly, your banana bread and your bagels may not be the same as your neighbor’s. Nevertheless, to compare averages, we’ve gone with the FDA’s Food Central Database for reference values, using the most default average recipes available. Likely you could make either or both of them a little healthier, but as it is, this is how we’ve gone about making it a fair comparison. With that in mind…
In terms of macros, bagels have more than 2x the protein and about 4x the fiber, while banana bread has slightly higher carbs and about 7x more fat. You may be wondering: are the fats healthy? And the answer is, it could be better, could be worse. The FDA recipe went with margarine rather than butter, which lowered the saturated fat to being only ¼ of the total fat (it would have been higher, had they used butter) whereas bagels have no saturated fat at all—which characteristic is quite integral to bagels, unless you make egg bagels, which is rather a different beast. All in all, the macros category is a clear win for bagels, especially when we consider the carb to fiber ratio.
In the category of vitamins, bagels have on average more vitamin B1, B3, B5, and B9, while banana bread has on average more of vitamins A and C. A modest win for bagels.
When it comes to minerals, bagels are the more nutrient dense with more copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while banana bread is not higher in any minerals. An obvious and easy win for bagels.
Closing thoughts: while the micronutrient profile quite possibly differs wildly from one baker to another, something that will probably stay more or less the same regardless is the carb to fiber ratio, and protein to fat. As a result, we’d weight the macros category as the more universally relevant. Bagels won in all categories today, as it happened, but it’s fairly safe to say that, on average, a baker who makes bagels and banana bread with the same levels of conscientiousness for health (or lack thereof) will tend to make bagels that are healthier than banana bread, based on the carb to fiber ratio, and the protein to fat ratio.
Enjoy!
Want to learn more?
You might like to read:
- Should You Go Light Or Heavy On Carbs?
- Why You’re Probably Not Getting Enough Fiber (And How To Fix It)
- Wholewheat Bread vs Seeded White – Which is Healthier?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Counterintuitive Dos and Don’ts of Nail Health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝I take a vitamin supplement for strengthening my nails (particularly one of my big toes!) – but they are running out! What do you recommend for strengthening nails? What is/are the key ingredient(s)?❞
Vitamin-wise, biotin (vitamin B7) is an underrated and very important one. As a bonus, it’s really good for your hair too (hair and nails being made of fundamentally the same “stuff”. Because it has exceptionally low toxicity, it can be taken up to 10,000% of the NRV, so if shopping for supplements, a high biotin content is better than a low one.
A lot of products marketed as for “skin, hair, and nails” focus on vitamins A and E, which are good for the skin but aren’t so relevant for nails.
Nutritionally, getting plenty of protein (whatever form you normally take it is fine) is also important since keratin (as nails are made of) is a kind of protein.
Outside of nutritional factors, a few other considerations:
- Testosterone strengthens nails, and declining testosterone levels (as experienced by most men over the age of 45) can result in weaker nails. So for men over 45 especially, a diet that favors testosterone (think foods rich in magnesium and zinc) is good.
- Because estrogen doesn’t do for women’s nails what testosterone does for men’s nails, increasing our magnesium and zinc intake won’t help our nails (but it’s still good for other things, including energy levels in the day and good sleep at night, and most people are deficient in magnesium anyway)
- Those of us who enjoy painted nails would do well to let our nails go without polish sometimes, as it can dry them out. And, acrylic nails are truly ruinous to nail health, as are gel nails (the kind that use a UV lamp to harden them—which is also bad for the skin)
- When nails are brittle, it can be tempting to soak them to reduce their brittleness. However, this is actually counterproductive, as the water will leech nutrients from the nails, and by the time you’ve been out of the footbath (for example) for about an hour, your nails will bemore brittle than before you soaked them.
- Use a moisturizing lotion or nail-oil instead—bonus if it contains biotin, keratin, and/or other helpful nutrients.
- Keep yourself hydrated, too! Hydration that comes to your nails from the inside will deliver nutrients, rather than removing them.
About those supplements: we don’t sell them (or anything else) but for your convenience, here are some great ones (this writer takes pretty much the same, just a different brand because I’m in a different country):
Magnesium Gummies (600mg) & Biotin Gummies (10,000µg)
Enjoy!
❝I was wondering whether there were very simple, clear bullet points or instructions on things to be wary of in Yoga.❞
That’s quite a large topic, and not one that lends itself well to being conveyed in bullet points, but first we’ll share the article you sent us when sending this question:
Tips for Avoiding Yoga Injuries
…and next we’ll recommend the YouTube channel @livinleggings, whose videos we feature here from time to time. She (Liv) has a lot of good videos on problems/mistakes/injuries to avoid.
Here’s a great one to get you started:
! Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

10 Ways To Balance Blood Sugars
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Let Them Eat Cake”, She Said…

This is Jessie Inchauspé, a French biochemist and author. She’s most known for her best-selling “Glucose Revolution: The Life-Changing Power Of Balancing Your Blood Sugar”.
It’s a great book (which we reviewed recently) and you absolutely should read it, but meanwhile, we’re going to distill at least the most critical core ideas, 10almonds style. In this case, her “ten hacks”:
Eat foods in the right order
The order is:
- Fiber first
- Protein and fat second
- Starches and sugars last
What happens here is… the fiber perks up the gut bacteria, the protein and fat will then be better-digested next, and the starches and sugars will try to jump the line, but they can’t because the fiber is a physical speedbump and the proteins and fats are taking the prime place for being digested. So instead, the starches and sugars—usually responsible for blood sugar spikes—get processed much more gradually, resulting in a nice even curve.
Add a green starter to all your meals
We know what you’re thinking: “that’s just the first one again”, but no. This is an extra starter, before you get to that. If you’re the cook of the household, this can absolutely simply mean snacking on green ingredients while cooking.
Stop counting calories
Especially, she advises: stop worrying about extra calories from fats, such as if doing an oil-and-vinegar dressing for salad—which she also recommends, because all three components (the oil, the vinegar, and the salad) help even out blood sugar levels.
Flatten your breakfast curve
For many, breakfast is the starchiest meal of the day, if not the sugariest. Inchauspé recommends flipping this (ideally) or softening it (if you really must have a carb-based breakfast):
- Top choices include: a warm vegetable salad, fish, or eggs (or tofu if you don’t do animal products).
- Next-best include: if you must have toast, make sure to have butter (and/or the aforementioned egg/tofu, for example) to give your digestion an extra thing to do.
- Also: she recommends skipping the juice in favour of home-made breakfast smoothies. That way, instead of basically just sugar with some vitamins, you’re getting a range of nutrients that, if you stack it right, can constitute a balanced meal itself, with fiber + protein + fat + carbs.
Have any type of sugar—they’re all the same
They’re technically not, but the point is that your body will immediately take them apart and then they will be just the same. Whether it’s the cheapest white sugar or the most expensive organic lovingly hand-reared free-range agave nectar, your body is going to immediately give it the chop-shop treatment (a process so quick as to be practically instantaneous) and say “this is now glucose”.
Pick a dessert over a sweet snack
Remember that about the right order for foods? A dessert, when your body is already digesting dinner, is going to make much less of a glucose spike than, say, a blueberry muffin when all you’ve had this morning is coffee and juice.
Reach for the vinegar before you eat
We recently did a whole main feature about this, so we’ll not double up today!
After you eat, move
The glucose you eat will be used to replace lost muscle glycogen, before any left over is stored as fat… and, while it’s waiting to be stored as fat, just sitting in your bloodstream being high blood sugars. So, this whole thing will go a lot better if you are actively using muscle glycogen (by moving your body).
Inchauspé gives a metaphor: imagine a steam train worker, shoveling coal into the furnace. Meanwhile, other workers are bringing more coal. If the train is moving quickly, the coal can be shoveled into the furnace and burned and won’t build up so quickly. But if the train is moving slowly or not at all, that coal is just going to build up and build up, until the worker can shovel no more because of being neck-deep in coal.
Same with your blood sugars!
If you want to snack, go low-sugar
In the category of advice that will shock nobody: sugary snacks aren’t good for avoiding blood sugar spikes! This one probably didn’t need a chapter devoted to it, but anyway: low sugar is indeed the way to go for snacks.
Put some clothes on your carbs
This is about olive oil on pasta, butter on potatoes, and so forth. Basically, anything starchy is going to be broken down quickly to sugar and sent straight into the bloodstream, if there’s nothing to slow it down. If you’re wondering what to do with rice: adding a tablespoon of chia seeds to the rice while cooking (so they’re cooked together) will add very healthy fats to your rice, and (because they’ve been cooked) will not seem like eating seeds, by the way. In terms of texture and appearance, it’ll be as though you threw some black pepper in*
*which you should also do for many reasons, but that’s beyond the scope of this “about blood sugars” feature!
Wanting to know more about the science of this?
We’ve done all we have room for here today, but Inchauspé is, as ever, happy to explain it herself:
Prefer text? Check out:
The Science Behind Glucose GoddessDon’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: