The Mental Health Dangers Of Oversharing
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Oversharers can be fun and amiable; the life of the party. In and of itself, this something that can be considered “pro-social” and thus healthy.
But the problem for one’s mental health in the long-run lies in the “over” part of oversharing. Sometimes, if not checking in with the other person’s comfort, oversharing can be “trauma-dumping”, and push people away. Alternatively, if the oversharing exposes an unmet need, it can make the other person feel obliged to try to help in some fashion, which in the long run may also cause awkwardness and withdrawal.
Some potential problems are purely internal, such the feelings of shame or anxiety that can come afterwards; “I should not have been so vulnerable”, “What if my friends think badly of me now?”, etc.
And of course, sometimes those fears are then validated by reality, if “friends” indeed take advantage of that, or withdraw their friendship. That’s a minority occurrence, but it doesn’t make it any less of a crushing thing if it happens.
Sometimes people overshare because of being a bad judge of what’s a socially-approved appropriate amount of sharing; sometimes people overshare out of a need for closeness, and perhaps the hope of hearing what one needed to hear previously.
The dangers of oversharing don’t mean that we should never speak about our experiences and feelings; in fact sometimes, it is the most healthy thing to do—be it because it’s something that needs communicating to a specific person, or because it’s something we just need to “get off our chest”.
In short, it can be good to share! It can also be good to do so judiciously, by conscious decision and not in response to a spur-of-the-moment impulse, and remember to prioritize our own safety.
Below, Alain de Botton explains more of the psychodynamics of this:
Click Here If The Embedded Video Doesn’t Load Automatically!
10almonds tip, not included in the video: unsure whether your urge to share is too impulsive or not? Write a letter/email, and wait until the next day to decide whether or not to send it.
Want to read more?
Check out:
Breathe; Don’t Vent (At Least In The Moment)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Lucid Dreaming – by Stephen LaBerge Ph.D.

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For any unfamiliar: lucid dreaming means being aware that one is dreaming, while dreaming, and exercising a degree of control over the dream. Superficially, this is fun. But if one really wants to go deeper into it, it can be a lot more:
Dr. Stephen LaBerge takes a science-based approach to lucid dreaming, and in this work provides not only step-by-step instructions of several ways of inducing lucid dreaming, but also, opens the reader’s mind to things that can be done there beyond the merely recreational:
In lucid dreams, he argues and illustrates, it’s possible to talk to parts of one’s own subconscious (Inception, anyone? Yes, this book came first) and get quite an amount of self-therapy done. And that hobby you wish you had more time to practice? The possibilities just became limitless. And who wouldn’t want that?
Share This Post
-

Stop Cancer 20 Years Ago
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Get Abreast And Keep Abreast

This is Dr. Jenn Simmons. Her specialization is integrative oncology, as she—then a breast cancer surgeon—got breast cancer, decided the system wasn’t nearly as good from the patients’ side of things as from the doctors’ side, and took to educate herself, and now others, on how things can be better.
What does she want us to know?
Start now
If you have breast cancer, the best time to start adjusting your lifestyle might be 20 years ago, but the second-best time is now. We realize our readers with breast cancer (or a history thereof) probably have indeed started already—all strength to you.
What this means for those of us without breast cancer (or a history therof) is: start now
Even if you don’t have a genetic risk factor, even if there’s no history of it in your family, there’s just no reason not to start now.
Start what, you ask? Taking away its roots. And how?
Inflammation as the root of cancer
To oversimplify: cancer occurs because an accidentally immortal cell replicates and replicates and replicates and takes any nearby resources to keep on going. While science doesn’t know all the details of how this happens, it is a factor of genetic mutation (itself a normal process, without which evolution would be impossible), something which in turn is accelerated by damage to the DNA. The damage to the DNA? That occurs (often as not) as a result of cellular oxidation. Cellular oxidation is far from the only genotoxic thing out there, and a lot of non-food “this thing causes cancer” warnings are usually about other kinds of genotoxicity. But cellular oxidation is a big one, and it’s one that we can fight vigorously with our lifestyle.
Because cellular oxidation and inflammation go hand-in-hand, reducing one tends to reduce the other. That’s why so often you’ll see in our Research Review Monday features, a line that goes something like:
“and now for those things that usually come together: antioxidant, anti-inflammatory, anticancer, and anti-aging”
So, fight inflammation now, and have a reduced risk of a lot of other woes later.
See: How to Prevent (or Reduce) Inflammation
Don’t settle for “normal”
People are told, correctly but not always helpfully, such things as:
- It’s normal to have less energy at your age
- It’s normal to have a weaker immune system at your age
- It’s normal to be at a higher risk of diabetes, heart disease, etc
…and many more. And these things are true! But that doesn’t mean we have to settle for them.
We can be all the way over on the healthy end of the distribution curve. We can do that!
(so can everyone else, given sufficient opportunity and resources, because health is not a zero-sum game)
If we’re going to get a cancer diagnosis, then our 60s are the decade where we’re most likely to get it. Earlier than that and the risk is extant but lower; later than that and technically the risk increases, but we probably got it already in our 60s.
So, if we be younger than 60, then now’s a good time to prepare to hit the ground running when we get there. And if we missed that chance, then again, the second-best time is now:
See: Focusing On Health In Our Sixties
Fast to live
Of course, anything can happen to anyone at any age (alas), but this is about the benefits of living a fasting lifestyle—that is to say, not just fasting for a 4-week health kick or something, but making it one’s “new normal” and just continuing it for life.
This doesn’t mean “never eat”, of course, but it does mean “practice intermittent fasting, if you can”—something that Dr. Simmons strongly advocates.
See: Intermittent Fasting: We Sort The Science From The Hype
While this calls back to the previous “fight inflammation”, it deserves its own mention here as a very specific way of fighting it.
It’s never too late
All of the advices that go before a cancer diagnosis, continue to stand afterwards too. There is no point of “well, I already have cancer, so what’s the harm in…?”
The harm in it after a diagnosis will be the same as the harm before. When it comes to lifestyle, preventing a cancer and preventing it from spreading are very much the same thing, which is also the same as shrinking it. Basically, if it’s anticancer, it’s anticancer, no matter whether it’s before, during, or after.
Dr. Simmons has seen too many patients get a diagnosis, and place their lives squarely in the hands of doctors, when doctors can only do so much.
Instead, Dr. Simmons recommends taking charge of your health as best you are able, today and onwards, no matter what. And that means two things:
- Knowing stuff
- Doing stuff
So it becomes our responsibility (and our lifeline) to educate ourselves, and take action accordingly.
Want to know more?
We recently reviewed her book, and heartily recommend it:
The Smart Woman’s Guide to Breast Cancer – by Dr. Jenn Simmons
Enjoy!
Share This Post
-

Pomegranate vs Apricot – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing pomegranate to apricot, we picked the pomegranate.
Why?
Both are great! Top tier fruits. But ultimately, pomegranate does have more to offer:
In terms of macros, pomegranate has more protein, carbs, and fiber (and even a little healthy fat—it’s the seeds); the main deciding factor on macros for fruits is almost always the fiber, and that’s the case here, which is why we hand the win to pomegranates in this category.
In the category of vitamins, pomegranates have more of vitamins B1, B2, b5, B6, B7, B9, K, and choline, while apricots have more of vitamins A, B3, and E. A clear win for pomegranates here.
When it comes to minerals, pomegranate has more copper, calcium, magnesium, manganese, phosphorus, selenium, and zinc, while apricots boast just a little more calcium and iron. Another easy win for pomegranates.
Looking at polyphenols, apricots finally win a category, with greater overall polyphenol coverage.
Which is good, but not enough to overcome the other three categories all being in pomegranates’ favor—hence the overall win for pomegranates here!
Of course, the solution is to enjoy both! Diversity is good, for exactly such reasons as this.
Want to learn more?
You might like to read:
Pomegranate’s Health Gifts Are Mostly In Its Peel ← in other words, the one part of the fruit you don’t normally eat. However! It can be dried and ground into a powder supplement, or else made in pomegranate tea.
Enjoy!
Share This Post
Related Posts
-

ADHD medication – can you take it long term? What are the risks and do benefits continue?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Attention deficit hyperactivity disorder (ADHD) is a condition that can affect all stages of life. Medication is not the only treatment, but it is often the treatment that can make the most obvious difference to a person who has difficulties focusing attention, sitting still or not acting on impulse.
But what happens once you’ve found the medication that works for you or your child? Do you just keep taking it forever? Here’s what to consider.
What are ADHD medications?
The mainstay of medication for ADHD is stimulants. These include methylphenidate (with brand names Ritalin, Concerta) and dexamfetamine. There is also lisdexamfetamine (branded Vyvanse), a “prodrug” of dexamfetamine (it has a protein molecule attached, which is removed in the body to release dexamfetamine).
There are also non-stimulants, in particular atomoxetine and guanfacine, which are used less often but can also be highly effective. Non-stimulants can be prescribed by GPs but this may not always be covered by the Pharmaceutical Benefits Scheme and could cost more.
How stimulants work
Some stimulants prescribed for ADHD are “short acting”. This means the effect comes on after around 20 minutes and lasts around four hours.
Longer-acting stimulants give a longer-lasting effect, usually by releasing medication more slowly. The choice between the two will be guided by whether the person wants to take medication once a day or prefers to target the medication effect to specific times or tasks.
For the stimulants (with the possible exception of lisdexamfetamine) there is very little carry-over effect to the next day. This means the symptoms of ADHD may be very obvious until the first dose of the morning takes effect.
One of the main aims of treatment is the person with ADHD should live their best life and achieve their goals. In young children it is the parents who have to consider the risks and benefits on behalf of the child. As children mature, their role in decision making increases.
What about side effects?
The most consistent side effects of the stimulants are they suppress appetite, resulting in weight loss. In children this is associated with temporary slowing of the growth rate and perhaps a slight delay in pubertal development. They can also increase the heart rate and may cause a rise in blood pressure. Stimulants often cause insomnia.
These changes are largely reversible on stopping medication. However, there is concern the small rises in blood pressure could accelerate the rate of heart disease, so people who take medication over a number of years might have heart attacks or strokes slightly sooner than would have happened otherwise.
This does not mean older adults should not have their ADHD treated. Rather, they should be aware of the potential risks so they can make an informed decision. They should also make sure high blood pressure and attacks of chest pain are taken seriously.
Stimulants can be associated with stomach ache or headache. These effects may lessen over time or with a reduction in dose. While there have been reports about stimulants being misused by students, research on the risks of long-term prescription stimulant dependence is lacking.
Will medication be needed long term?
Although ADHD can affect a person’s functioning at all stages of their life, most people stop medication within the first two years.
People may stop taking it because they don’t like the way it makes them feel, or don’t like taking medication at all. Their short period on medication may have helped them develop a better understanding of themselves and how best to manage their ADHD.
In teenagers the medication may lose its effectiveness as they outgrow their dose and so they stop taking it. But this should be differentiated from tolerance, when the dose becomes less effective and there are only temporary improvements with dose increases.
Tolerance may be managed by taking short breaks from medication, switching from one stimulant to another or using a non-stimulant.

Medication is usually prescribed by a specialist but rules differ around Australia.
Ground Picture/ShutterstockToo many prescriptions?
ADHD is becoming increasingly recognised, with more people – 2–5% of adults and 5–10% of children – being diagnosed. In Australia stimulants are highly regulated and mainly prescribed by specialists (paediatricians or psychiatrists), though this differs from state to state. As case loads grow for this lifelong diagnosis, there just aren’t enough specialists to fit everyone in.
In November, a Senate inquiry report into ADHD assessment and support services highlighted the desperation experienced by people seeking treatment.
There have already been changes to the legislation in New South Wales that may lead to more GPs being able to treat ADHD. Further training could help GPs feel more confident to manage ADHD. This could be in a shared-care arrangement or independent management of ADHD by GPs like a model being piloted at Nepean Blue Mountains Local Health District, with GPs training within an ADHD clinic (where I am a specialist clinician).
Not every person with ADHD will need or want to take medication. However, it should be more easily available for those who could find it helpful.

Alison Poulton, Senior Lecturer, Brain Mind Centre Nepean, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
How we can prepare for future public health emergencies
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The U.S. is experiencing an increasing number of disease outbreaks and extreme weather events. While state and national preparedness for public health emergencies has improved in some areas, dangerous gaps remain, says a recent report from Trust for America’s Health.
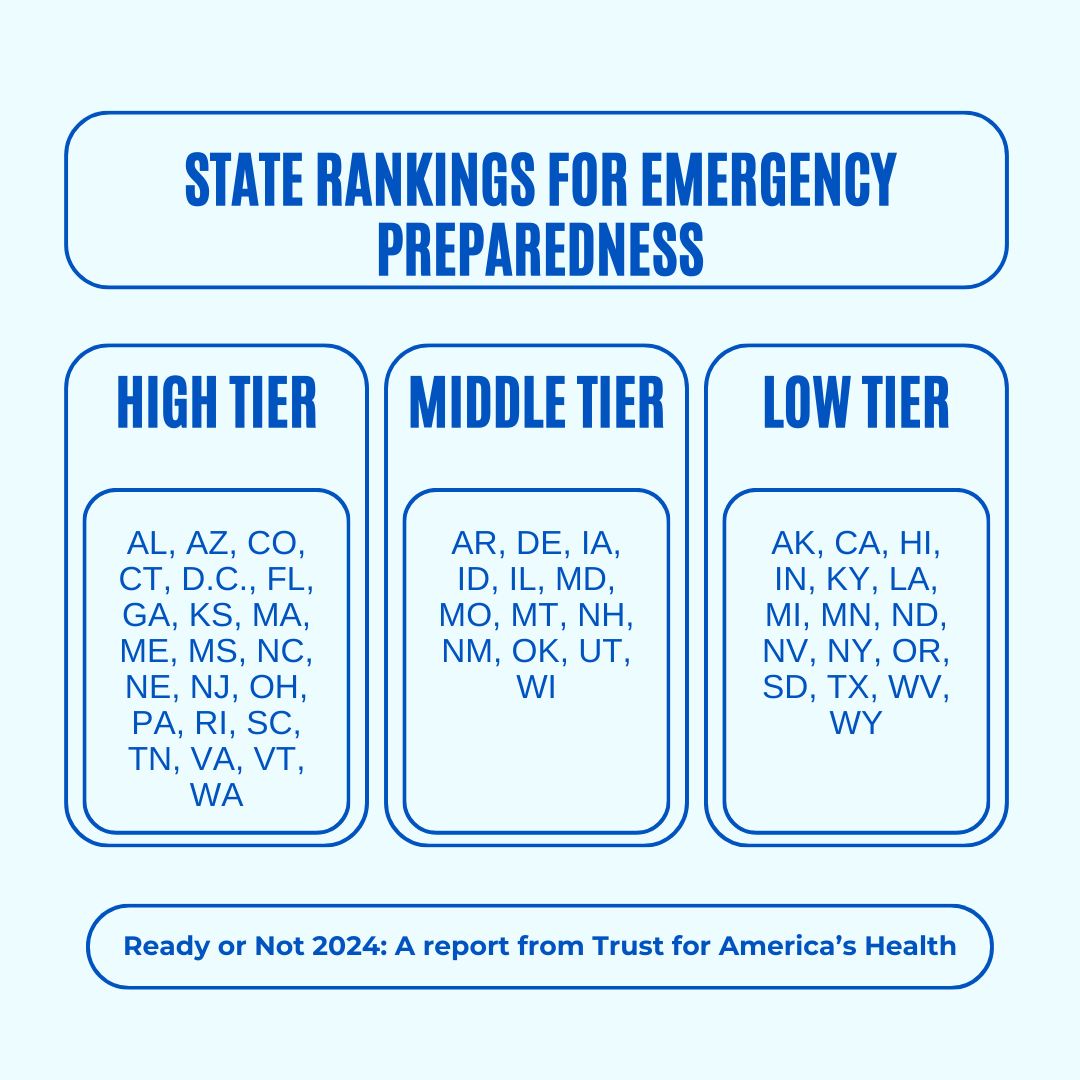
Titled, “Ready or Not 2024: Protecting the Public’s Health from Diseases, Disasters, and Bioterrorism,” the report identifies gaps in national and state preparedness for public health emergencies and provides recommendations for improvement.
Using nine key indicators, the report categorizes all U.S. states and the District of Columbia into three readiness levels: high, medium, and low. The writers hope the report will help policymakers in under-performing states improve public health infrastructure.
Read on to learn more about what the research found and how we can individually prepare for future public health emergencies.
There’s work to be done
The report highlights areas with strong performance as well as those that need improvement.
Some areas with strong performance:
- State public health funding: Most states and the District of Columbia either maintained or increased their public health funding during the 2023 fiscal year.
- Health care labor force preparedness: Most states have started expanding the health care labor force for improved emergency response. As of 2023, 39 states participated in the Nurse Licensure Compact, which allows nurses to work in multiple member states without the need for additional state licenses.
Some areas that need improvement:
- Hospital safety scores: Only 25 percent of acute care hospitals earned the highest patient safety grade in fall 2023. These scores measure health care-associated infection rates, intensive care unit capacity, and other metrics. More high-scoring hospitals would improve preparedness for future public health emergencies.
- Access to paid time off: From March 2018 to March 2023, only 55 percent of U.S. workers used paid time off. Access to paid time off is important for reducing the spread of infectious diseases.
We can all do our part by staying up to date on vaccines
While the report focuses on policy changes that would improve emergency preparedness, Trust for America’s Health’s research identifies one way that we can individually prepare for future public health emergencies: staying up to date on vaccines.
The report found that during the 2022-2023 flu season, only 49 percent of those eligible for the flu vaccine received it. Public health experts are concerned that false claims about COVID-19 vaccines have resulted in overall vaccine hesitancy.
A decline in vaccination rates has led to an uptick in life-threatening, vaccine-preventable diseases, such as measles. Increasing vaccine uptake would prevent the spread of vaccine-preventable diseases and reduce strain on hospital systems during public health crises.
Make sure that you and your children have received all recommended vaccines to prevent severe illness, hospitalization, and death. Learn more about recommended vaccines for adults and children from the CDC.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

When Carbs, Proteins, & Fats Switch Metabolic Roles
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Strange Things Happening In The Islets Of Langerhans
It is generally known and widely accepted that carbs have the biggest effect on blood sugar levels (and thus insulin response), fats less so, and protein least of all.
And yet, there was a groundbreaking study published yesterday which found:
❝Glucose is the well-known driver of insulin, but we were surprised to see such high variability, with some individuals showing a strong response to proteins, and others to fats, which had never been characterized before.
Insulin plays a major role in human health, in everything from diabetes, where it is too low*, to obesity, weight gain and even some forms of cancer, where it is too high.
These findings lay the groundwork for personalized nutrition that could transform how we treat and manage a range of conditions.❞
*saying ”too low” here is potentially misleading without clarification; yes, Type 1 Diabetics will have too little [endogenous] insulin (because the pancreas is at war with itself and thus isn’t producing useful quantities of insulin, if any). Type 2, however, is more a case of acquired insulin insensitivity, because of having too much at once too often, thus the body stops listening to it, “boy who cried wolf”-style, and the pancreas also starts to get fatigued from producing so much insulin that’s often getting ignored, and does eventually produce less and less while needing more and more insulin to get the same response, so it can be legitimately said “there’s not enough”, but that’s more of a subjective outcome than an objective cause.
Back to the study itself, though…
What they found, and how they found it
Researchers took pancreatic islets from 140 heterogenous donors (varied in age and sex; ostensibly mostly non-diabetic donors, but they acknowledge type 2 diabetes could potentially have gone undiagnosed in some donors*) and tested cell cultures from each with various carbs, proteins, and fats.
They found the expected results in most of the cases, but around 9% responded more strongly to the fats than the carbs (even more strongly than to glucose specifically), and even more surprisingly 8% responded more strongly to the proteins.
*there were also some known type 2 diabetics amongst the donors; as expected, those had a poor insulin response to glucose, but their insulin response to proteins and fats were largely unaffected.
What this means
While this is, in essence, a pilot study (the researchers called for larger and more varied studies, as well as in vivo human studies), the implications so far are important:
It appears that, for a minority of people, a lot of (generally considered very good) antidiabetic advice may not be working in the way previously understood. They’re going to (for example) put fat on their carbs to reduce the blood sugar spike, which will technically still work, but the insulin response is going to be briefly spiked anyway, because of the fats, which very insulin response is what will lower the blood sugars.
In practical terms, there’s not a lot we can do about this at home just yet—even continuous glucose monitors won’t tell us precisely, because they’re monitoring glucose, not the insulin response. We could probably measure everything and do some math and work out what our insulin response has been like based on the pace of change in blood sugar levels (which won’t decrease without insulin to allow such), but even that is at best grounds for a hypothesis for now.
Hopefully, more publicly-available tests will be developed soon, enabling us all to know our “insulin response type” per the proteome predictors discovered in this study, rather than having to just blindly bet on it being “normal”.
Ironically, this very response may have hidden itself for a while—if taking fats raised insulin response without raising blood sugar levels, then if blood sugar levels are the only thing being measured, all we’ll see is “took fats at dinner; blood sugars returned to normal more quickly than when taking carbs without fats”.
You can read the study in full here:
Proteomic predictors of individualized nutrient-specific insulin secretion in health and disease
Want to know more about blood sugar management?
You might like to catch up on:
- 10 Ways To Balance Your Blood Sugars
- Track Your Blood Sugars For Better Personalized Health
- How To Turn Back The Clock On Insulin Resistance
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: