The Menopause Brain – by Dr. Lisa Mosconi
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
With her PhD in neuroscience and nuclear medicine (a branch of radiology, used for certain types of brain scans, amongst other purposes), whereas many authors will mention “brain fog” as a symptom of menopause, Dr. Mosconi can (and will) point to a shadowy patch on a brain scan and say “that’s the brain fog, there”.
And so on for many other symptoms of menopause that are commonly dismissed as “all in your head”, notwithstanding that “in your head” is the worst place for a problem to be. You keep almost your entire self in there!
Dr. Mosconi covers how hormones influence not just our moods in a superficial way, but also change the structure of our brain over time.
Importantly, she also gives an outline of how to stay on the ball; what things to watch out for when your doctor probably won’t, and what things to ask for when your doctor probably won’t suggest them.
Bottom line: if menopause is a thing in your life (or honestly, even if it isn’t but you are running on estrogen rather than testosterone), then this is a book for you.
Click here to check out The Menopause Brain, and look after yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Sweet Spot for Brain Health – by Dr. Sui Wong

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
At 10almonds we often mention that “what’s good for the heart is good for the brain”, but at least in part, it’s because (as this book makes very clear), “what’s good for the blood is good for the brain”. After all, our brain uses about 25% of our energy, and that energy is delivered there by the blood. And if it doesn’t get enough nutrients, oxygen, etc, and detritus isn’t taken away, then problems happen.
Dr. Wong discusses Alzheimer’s as heavily driven by metabolic problems such as diabetes and even pre-diabetes, and sets out to put in our hands the guidebook to not only not doing that, but also, actually making sure our brain gets proper nourishment without delivering that as intermittent sugar spikes because we opted for a something with very fast-acting carbs to perk us up energetically.
More than most books on the topic, she talks a lot about the neurobiology of glucose metabolism, so that’s something that really sets this book apart from many of its genre.
The style is narrative, explaining the body’s processes in a clear fashion, without skimping on science. There are definitely words that your average layperson might not know, but they’re explained as we go, and there are frequent recaps of what we learned previously, making for ultimately easy reading.
After all the information is given, there’s also a guided “12-week challenge” with a theme-of-the-week for each week, to integrate a new lifestyle adjustment each week in a progressive fashion so that without needing to drastically change many things at once, we get where we need to be in terms of healthy habits.
Bottom line: if you’d like to do right by your brain and while you’re at it say goodbye to blood sugar highs and lows, then this book is an excellent guide for that.
Click here to check out Sweet Spot For Brain Health, and enjoy a consistently-energized brain!
Share This Post
-

Continuous Glucose Monitors Without Diabetes: Pros & Cons
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The “Glucose Goddess”, biochemist Jessie Inchauspé, gives us the low-down:
Knowledge is power (but watch out)
A continuous glucose monitor (CGM) is a device that continually monitors glucose levels, without the need to stab one’s finger every few hours to test blood.
It was designed for diabetics, especially for those with Type 1 Diabetes, where around-the-clock monitoring is necessary for appropriate insulin dosing.
For non-diabetics, they can be a good way of learning what our body’s response to various foods and activities is like, the better to be able to tweak our habits to avoid undue glucose spikes (which are harmful for our pancreas, liver, heart, brain, kidneys, and more).
How it works: there’s a sensor that sits on the arm (or elsewhere, but the arm is a popular placement) with a little probe that goes under the skin. It’s applied using a device that inserts it automatically using a needle (you only need to press a button, you don’t need to guide the needle yourself); the needle then retracts, leaving the soft, flexible probe in place. Having been attached, that sensor can now stay in place for 2 weeks (usually; depends on brand, but for example FreeStyle Libre, the most popular brand, the sensors last 2 weeks), and yes, it’s fine to bathe/shower/etc with it. When you want an update from your CGM, you scan it with your phone (or you can buy a dedicated reader, but that is more expensive and unnecessary), and it uploads the data since your last scan.
Pros: it’s convenient and gives a lot of data, so even if you only use it for a short period of time (for example, a month) you can get a very good idea of what affects your blood sugar levels and how. Also, because of the constant nature of the monitoring, it helps avoid accidental sample bias of the kind that can occur with manual testing, by testing a little too soon or too late, and missing a spike/dip.
Cons: it can be expensive, depending on where you live and what options are available for you locally, so you might not want to do it long-term (since that would require buying two sensors per month). It’s also, for all its wealth of data, slightly less accurate than fingerprick testing—that’s because it takes an interstitial reading instead of directly from the blood. For this reason, if you test both ways, you may find a discrepancy of about 3mg/dL. Given that the healthy range is about 70–140mg/dL, a discrepancy of 3mg/dL is probably not going to be important, but it is a thing to mention can (and probably will) happen.
Patterns to bear in mind (with any kind of blood sugar monitoring):
- Dawn phenomenon: a natural glucose rise upon waking.
- Exercise-induced spikes (normal due to energy demands).
- Fat in meals slowing glucose absorption.
- Different foods can sometimes cause a double-wave after dinner (because glucose from different foods is absorbed differently, and/or different foods affect insulin response independent of glucose)
- Steep, rapid spikes that are more harmful than gradual, sustained increases.
- Vitamin C spikes: temporary chemical interference with the sensor, not actual glucose rises.
- Nighttime glucose dips (often false readings caused by sleeping position).
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
10 Ways To Balance Blood Sugars
Take care!
Share This Post
-
Bell Pepper vs Sweetcorn – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing bell pepper to sweetcorn, we picked the corn.
Why?
If you’re thinking “but wait, which color bell pepper, don’t they have different nutritional properties?” then firstly, well-remembered, and secondly, it doesn’t matter in this case. The main things that it affects are vitamins A and C and various polyphenols, and even the weakest bell pepper for them wins on both of those vitamins (while the strongest bell peppers for them still lose on vitamins in total) and even the strongest bell pepper for them loses on polyphenols, so the results go the same with any color.
In terms of macros, the corn has more carbs, protein, and fiber; however, both are low in glycemic index, so we’ll go with the “more food per food” option, the corn.
In the category of vitamins, even green bell peppers (the least well-endowed) have more of vitamins A, B6, C, E, and K, while sweetcorn has more of vitamins B1, B2, B3, B5, B9, and choline, compared to even yellow or red bell peppers (which are the best peppers for vitamins). So, a moderate win for the corn.
When it comes to minerals, bell peppers have more calcium and copper, while sweetcorn has more iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. An easy win for sweetcorn.
In short, enjoy both, but the corn is the overall winner today!
Want to learn more?
You might like to read:
- Brain Food? The Eyes Have It! ← green bell peppers are a good source of lutein, as is sweetcorn
- A Spectrum Of Specialties: Which Bell Peppers To Pick?
Take care!
Share This Post
Related Posts
-
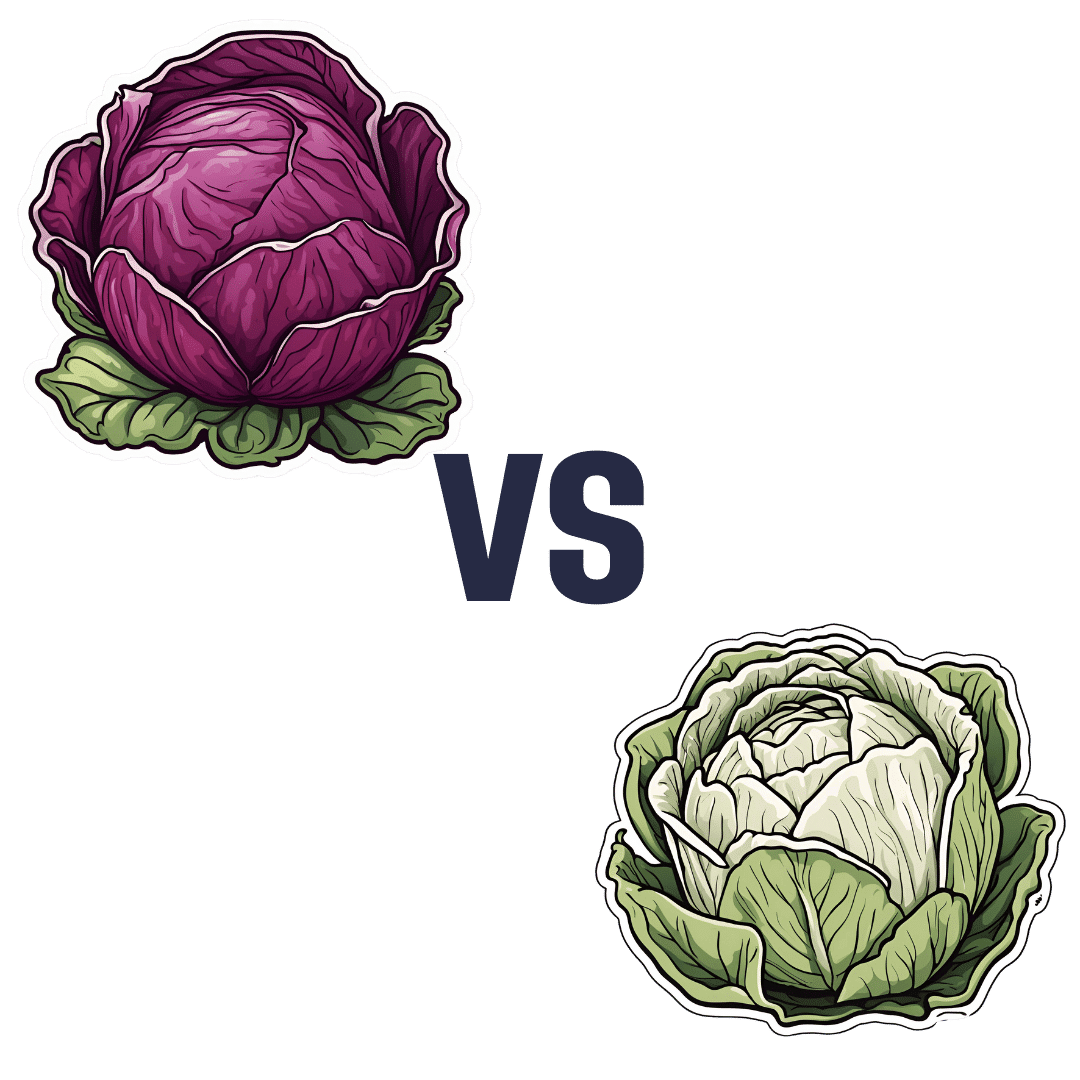
Red Cabbage vs White Cabbage – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing red cabbage to white cabbage, we picked the red.
Why?
Perhaps you guessed this one, based on the “darker and/or more colorful foods are usually more nutritionally dense” dictum. That’s not always true, by the way, but it is a good rule of thumb and it is correct here. In the case of cabbages, each type is a nutritional powerhouse, but red does beat white:
In terms of macros, they’re quite comparable. They’re both >90% water with just enough other stuff (carbs, fiber, protein) to hold them together, and the “other stuff” in question is quite similarly proportioned in both cases. Within the carbs, even the sugar breakdown is similar. There are slight differences, but the differences are not only tiny, but also they balance out in any case.
When it comes to vitamins, as you might expect, the colorful red cabbage does better with more of vitamins A, B1, B2, B3, B6, C, and choline, while white has more of vitamins B5, B9, E, and K. So, a 7:4 win for red.
In the category of minerals, it’s even more polarized; red cabbage has more calcium, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. On the other hand, white contains a tiny amount more copper.
In short, both are great (red just makes white look bad by standing next to it, but honestly, white has lots of all those same things too, just not quite as much as red), and this writer will continue to use white when making her favorite shchi, but if you’re looking for the most nutritionally dense option, it’s red.
Want to learn more?
You might like to read:
Enjoy Bitter Foods For Your Heart & Brain
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How To Reduce Your Alzheimer’s Risk
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Reduce Your Alzheimer’s Risk
Alzheimer’s is just one cause of dementia, but it’s a very notable one, not least of all because it’s
- a) the most common cause of dementia, and
- b) a measurably terminal disease.
For that reason we’re focusing on Alzheimer’s today, although most of the advice will go for avoiding dementia in general.
First, some things not everyone knows about Alzheimer’s:
- Alzheimer’s is a terminal disease.
- People who get a diagnosis at age 60 are typically given 4–8 years to live.
- Some soldier on for as many as 20, but those are rare outliers.
- Alzheimer’s begins 20 years or more before other symptoms start to develop.
- This makes this information very relevant for younger people approaching 40, for example.
- Alzheimer’s accounts for 60–80% of dementia, and affects around 6% of people over 60.
- By the age of 65, that figure is 10%. By the age of 70, however, the percentage is still about the same—this is because of the mortality rate preventing the accumulation of Alzheimer’s patients over time.
Want to know more? Read: 2023 Alzheimer’s Disease Facts And Figures Special Report ← this is a very comprehensive downloadablereference, by the way, including a lot of information about diagnosis, treatmentpathways, and earlyinterventions.
Speaking of diagnosis…
Know what the symptoms are… and aren’t!
Forgetting your car keys can be frustrating. Forgetting them frequently can be worrying.
But: there’s a difference between forgetting your car keys, and forgetting what car keys are used for. The latter is the kind of memory loss that’s more of a red flag for Alzheimer’s.
Similarly: forgetting someone’s name can be embarrassing. Forgetting someone’s name, asking them, forgetting asking them, asking them again, forgetting again (lather rinse repeat) is more of a red flag for Alzheimer’s.
There are other symptoms too, some of them less commonly known:
❝Difficulty remembering recent conversations, names or events; apathy; and depression are often early symptoms. Communication problems, confusion, poor judgment and behavioral changes may occur next. Difficulty walking, speaking, and swallowing are common in the late stages of the disease❞
If you or a loved one are experiencing worrying symptoms: when it comes to diagnosis and intervention, sooner is a lot better than later, so do talk to your doctor.
As for reducing your risk? First, the obvious stuff:
The usual 5 things that go for almost everything:
- Have a good diet—the Mediterranean Diet is once again recommended (we expect this will not be a surprise to regular readers!)
- Get regular exercise—in the case of avoiding Alzheimer’s and other dementias, typically the most important thing here is heart health, so getting regular cardiovascular exercise, such walking, running, or dancing is great. Cycling too. Swimming, not so much. Not that swimming’s bad or anything, it’s just that when your body is horizontal, the heart has less work to do, especially in the upper part of the body, because it’s not defying gravity. Similarly, yoga is great for the health but won’t particularly help with this, nor will weight training.
- Get good sleep—as we get older, we tend to need less sleep, and tend more towards the lower end of the standard “7–9 hours” prescription, but getting at least those 7 hours makes a huge difference.
- Cut down (or eliminate) alcohol consumption—and especially avoid binge-drinking. While “binge-drinking” is typically associated with young people, that Christmas party where that one uncle gets very drunk is also binge-drinking, for example. Plus, heavy drinking in early life has also been correlated with higher risk of Alzheimer’s later.
- Don’t smoke. It’s bad for everything, and Alzheimer’s risk is no exception.
How much do lifestyle changes alone make a difference?
They make a big difference. This 2022 population-based cohort study (so: huge sample size) looked at people who had 4–5 of the healthy lifestyle factors being studied, vs people who had 0–1 of them. They found:
❝A healthy lifestyle was associated with a longer life expectancy among men and women, and they lived a larger proportion of their remaining years without Alzheimer’s dementia.❞
The numbers of years involved by the way ranged between 3 and 20 years, in terms of life expectancy and years without or with Alzheimer’s, with the average increase of healthy life years being approximately the same as the average increase in years. This is important, because:
A lot of people think “well if I’m going to go senile, I might as well [unhealthy choice that shortens lifespan]”, but they misunderstand a critical factor:
The unhealthy choices will reduce their healthy life years, and simply bring the unhealthy ones (and subsequent death) sooner. If you’re going to spend your last few years in ill-health, it’s better to do so at 90 than 50.
The other thing you may already know… And a thing about it that not everyone considers:
Keeping cognitively active is important. This much is broadly known by the general public, and to clinicians, this was the fourth “healthy factor” in the list of five (instead of the sleep that we put there, because we were listing the 5 things that go for most preventable health issues).
Everyone leaps to mention sudoku at this point, so if that’s your thing, great, enjoy it! (This writer personally enjoys chess, which isn’t everyone’s cup of tea; if it yours though, you can come join her on Chess.com and we’ll keep sharp together)
But the more parts of your mental faculties you keep active, the better. Remember, brainpower (as with many things in health and life) is a matter of “use it or lose it” and this is on a “per skill” basis!
What this means: doing sudoku (a number-based puzzle game) or chess (great as it may be) won’t help as much for keeping your language skills intact, for example. Given that language skills are one of the most impactful and key faculties to get lost to Alzheimer’s disease, neglecting such would be quite an oversight!
Some good ways to keep your language skills tip-top:
- Read—but read something challenging, if possible. It doesn’t have to be Thomas Scanlon’s What We Owe To Each Other, but it should be more challenging than a tabloid, for example. In fact, on the topic of examples:
- This newsletter is written to be easy to read, while not shying away from complex ideas or hard science. Our mission is literally to “make [well-sourced, science-based] health and productivity crazy simple”.
- But the academic papers that we link? Those aren’t written to be easy to read. Go read them, or at least the abstracts (in academia, an abstract is essentially an up-front summary, and is usually the first thing you’ll see when you click a link to a study or such). Challenge yourself!
- Write—compared to reading/listening, producing language is a (related, but) somewhat separate skill. Just ask any foreign language learner which is more challenging: reading or writing!
- Journaling is great, but writing for others is better (as then you’ll be forced to think more about it)
- Learn a foreign language—in this case, what matters it that you’re practicing and learning, so in the scale of easy to hard, or doesn’t matter if it’s Esperanto or Arabic. Duolingo is a great free resource that we recommend for this, and they have a wide range of extensive courses these days.
Now for the least obvious things…
Social contact is important.
Especially in older age, it’s easy to find oneself with fewer remaining friends and family, and getting out and about can be harder for everyone. Whatever our personal inclinations (some people being more introverted or less social than others), we are fundamentally a social species, and hundreds of thousands of years of evolution have built us around the idea that we will live our lives alongside others of our kind. And when we don’t, we don’t do as well.
See for example: Associations of Social Isolation and Loneliness With Later Dementia
If you can’t get out and about easily:
- Online socialising is still socializing.
- Online community is still community.
- Online conversations between friends are still conversations between friends.
If you don’t have much (or anyone) in the category of friends and family, join Facebook groups related to your interests, for example.
Berries are surprisingly good
^This may read like a headline from 200,000 BCE, but it’s relevant here!
Particularly recommended are:
- blueberries
- blackberries
- raspberries
- strawberries
- cranberries
We know that many of these berries seem to have a shelf-life of something like 30 minutes from time of purchase, but… Frozen and dried are perfectly good nutritionally, and in many cases, even better nutritionally than fresh.
Read: Effect of berry-based supplements and foods on cognitive function: a systematic review
Turmeric’s health benefits appear to include protecting against Alzheimer’s
Again, this is about risk reduction, and turmeric (also called curcumin, which is not the same as cumin) significantly reduces the build-up of amyloid plaques in the brain. Amyloid plaques are part of the progression of Alzheimer’s.
See for yourself: Protective Effects of Indian Spice Curcumin Against Amyloid Beta in Alzheimer’s Disease
If you don’t like it as a spice (and even if you do, you probably don’t want to put it in your food every day), you can easily get it as a supplement in capsule form.
Lower your homocysteine levels
Lower our what now? Homocysteine is an amino acid used for making certain proteins, and it’s a risk factor for Alzheimer’s.
Foods high in folate (and possible other B-vitamins) seem to lower homocysteine levels. Top choices include:
- Leafy greens
- Cruciferous vegetables
- Tomatoes
Get plenty of lutein
We did a main feature about specifically this a little while ago, so we’ll not repeat our work here, but lutein is found in, well, the same things we just listed above, and lower levels of lutein are associated with Alzheimer’s disease. It’s not a proven causative factor—we don’t know entirely what causes Alzheimer’s, just a lot of factors that have a high enough correlation that it’d be remiss to ignore them.
Catch up on our previous article: Brain Food? The Eyes Have It
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Acid Reflux Diet Cookbook – by Dr. Harmony Reynolds
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Notwithstanding the title, this is far more than just a recipe book. Of course, it is common for health-focused recipe books to begin with a preamble about the science that’s going to be applied, but in this case, the science makes up a larger portion of the book than usual, along with practical tips about how to best implement certain things, at home and when out and about.
Dr. Reynolds also gives a lot of information about such things as medications that could be having an effect one way or the other, and even other lifestyle factors such as exercise and so forth, and yes, even stress management. Because for many people, what starts as acid reflux can soon become ulcers, and that’s not good.
The recipes themselves are diverse and fairly simple; they’re written solely with acid reflux in mind and not other health considerations, but they are mostly heathy in the generalized sense too.
The style is straight to the point with zero padding sensationalism, or chit-chat. It can make for a slightly dry read, but let’s face it, nobody is buying this book for its entertainment value.
Bottom line: if you have been troubled by acid reflux, this book will help you to eat your way safely out of it.
Click here to check out the Acid Reflux Diet Cookbook, and enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: