The Longevity Diet – by Dr. Valter Longo
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Another book with “The New Science” in its subtitle, so, is this one a new science?
Yes and no; some findings are new, many are not, what really sets this book apart from many of its genre though is that rather than focusing on fighting aging, it focuses on retaining youth. While this may seem like one and the same thing, there is a substantive difference beyond the ideological, which is: while anti-aging research focuses on what causes people to suffer age-related decline and fights each of those things, Dr. Longo’s research focuses on what is predominant in youthful bodies, cells, DNA, and looks to have more of that. Looking in a slightly different place means finding slightly different things, and knowledge is power indeed.
Dr. Longo bases his research and focus on his “5 pillars of longevity”. We’ll not keep them a mystery; they are:
- Juventology research
- Epidemiology
- Clinical studies
- Centenarian studies
- Study of complex systems
The first there (juventology research) may sound like needless jargon, but it is the counterpoint of the field of gerontology, and is otherwise something that didn’t have an established name.
You may wonder why “clinical studies” gets a separate item when the others already include studies; this is because many studies when it comes to aging and related topics are population-based studies, cohort studies, observational studies, or (as is often the case) multiple of the above at once.
Of course, all this discussion of academia is not itself practical information for the reader (unless we happen to work in the field), but it is interesting and does give confidence in the conclusions upon which the practical parts of the book are based.
And what are they? As the title suggests, it’s about diet, and specifically, it’s about Dr. Longo’s “fast-mimicking diet”, which boasts the benefits of intermittent fasting without intermittent fasting. This hinges, of course, on avoiding metabolic overload, which can be achieved with a fairly simple diet governed by the principles outlined in this book, based on the research referenced.
In the category of subjective criticism, there is quite a bit of fluff, much of it self-indulgently autobiographical and very complimentary, but its presence does not take anything away from the excellent content contained in the book.
Bottom line: if you’d like a fresh perspective on regaining/retaining youthfulness, then this is a great book to read.
Click here to check out The Longevity Diet, and stay younger!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How To Prevent And Reverse Type 2 Diabetes

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Turn back the clock on insulin resistance

This is Dr. Jason Fung. He’s a world-leading expert on intermittent fasting and low carbohydrate approaches to diet. He also co-founded the Intensive Dietary Management Program, later rebranded to the snappier title: The Fasting Method, a program to help people lose weight and reverse type 2 diabetes. Dr. Fung is certified with the Institute for Functional Medicine, for providing functional medicine certification along with educational programs directly accredited by the Accreditation Council for Continuing Medical Education (ACCME).
Why Intermittent Fasting?
Intermittent fasting is a well-established, well-evidenced, healthful practice for most people. In the case of diabetes, it becomes complicated, because if one’s blood sugars are too low during a fasting period, it will need correcting, thus breaking the fast.
Note: this is about preventing and reversing type 2 diabetes. Type 1 is very different, and sadly cannot be prevented or reversed in this fashion.
However, these ideas may still be useful if you have T1D, as you have an even greater need to avoid developing insulin resistance; you obviously don’t want your exogenous insulin to stop working.
Nevertheless, please do confer with your endocrinologist before changing your dietary habits, as they will know your personal physiology and circumstances in ways that we (and Dr. Fung) don’t.
In the case of having type 2 diabetes, again, please still check with your doctor, but the stakes are a lot lower for you, and you will probably be able to fast without incident, depending on your diet itself (more on this later).
Intermittent Fasting can be extra helpful for the body in the case of type 2 diabetes, as it helps give the body a rest from high insulin levels, thus allowing the body to become gradually re-sensitised to insulin.
Why low carbohydrate?
Carbohydrates, especially sugars, especially fructose*, cause excess sugar to be quickly processed by the liver and stored there. When the body’s ability to store glycogen is exceeded, the liver stores energy as fat instead. The resultant fatty liver is a major contributor to insulin resistance, when the liver can’t keep up with the demand; the blood becomes spiked full of unprocessed sugars, and the pancreas must work overtime to produce more and more insulin to deal with that—until the body starts becoming desensitized to insulin. In other words, type 2 diabetes.
There are other factors that affect whether we get type 2 diabetes, for example a genetic predisposition. But, our carb intake is something we can control, so it’s something that Dr. Fung focuses on.
*A word on fructose: actual fruits are usually diabetes-neutral or a net positive due to their fiber and polyphenols.
Fructose as an added ingredient, however, not so much. That stuff zips straight into your veins with nothing to slow it down and nothing to mitigate it.
The advice from Dr. Fung is simple here: cut the carbs. If you are already diabetic and do this with no preparation, you will probably simply suffer hypoglycemia, so instead:
- Enjoy a fibrous starter (a salad, some fruit, or perhaps some nuts)
- Load up with protein first, during your main meal—this will start to trigger your feelings of satedness
- Eat carbs last (preferably whole, unprocessed carbohydrates), and stop eating when 80% full.
Adapting Intermittent Fasting to diabetes
Dr. Fung advocates for starting small, and gradually increasing your fasting period, until, ideally, fasting 16 hours per day. You probably won’t be able to do this immediately, and that’s fine.
You also probably won’t be able to do this, if you don’t also make the dietary adjustments that help to give your liver a break, and thus by knock-on-effect, give your pancreas a break too.
With the dietary adjustments too, however, your insulin production-and-response will start to return to its pre-diabetic state, and finally its healthy state, after which, it’s just a matter of maintenance.
Want to hear more from Dr. Fung?
You may enjoy his blog, and for those who like videos, here is his YouTube channel:
Share This Post
-

Daily, Weekly, Monthly: Habits Against Aging
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Anil Rajani has advice on restoring/retaining youthfulness. Two out of three of the sections are on skincare specifically, which may seem a vanity, but it’s also worth remembering that our skin is a very large and significant organ, and makes a big difference for the rest of our physical health, as well as our mental health. So, it’s worthwhile to look after it:
The recommendations
Daily: meditation practice
Meditation reduces stress, which reduction in turn protects telomere length, slowing the overall aging process in every living cell of the body.
Weekly: skincare basics
Dr. Rajani recommends a combination of retinol and glycolic acid. The former to accelerate cell turnover, stimulate collagen production, and reduce wrinkles; the latter, to exfoliate dead cells, allowing the retinol to do its job more effectively.
We at 10almonds would like to add: wearing sunscreen with SPF50 is a very good thing to do on any day that your phone’s weather app says the UV index is “moderate” or higher.
Monthly: skincare extras
Here are the real luxuries; spa visits, microneedling (stimulates collagen production), and non-ablative laser therapy. He recommends creating a home spa if possible for monthly skincare treatments, investing in high-quality devices for long-term benefits.
For more on all of these things, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Age & Aging: What Can (And Can’t) We Do About It?
- No-Frills, Evidence-Based Mindfulness
- The Evidence-Based Skincare That Beats Product-Specific Hype
Take care!
Share This Post
-

Why We Get Sick – by Dr. Benjamin Bikman
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There’s a slightly buried lede here in that the title doesn’t offer this spoiler, but we will: the book is about insulin resistance.
However, unlike the books we’ve reviewed about blood sugar management, this time the focus is really and truly on insulin itself—and that makes some important differences:
Dr. Bikman makes the case that while indeed hyper- or hypoglycemia bring their problems, mostly these are symptoms rather than causes, and the real culprit is insulin resistance, and this is important for two main reasons:
- Insulin resistance occurs well before the other symptoms set in (which means: it is the thing that truly needs to be nipped in the bud; if your fasting blood sugars are rising, then you missed “nipping it in the bud” likely by a decade or more)
- Insulin resistance causes more problems than “mere” hyperglycemia (the most commonly-known result of insulin resistance) does, so again, it really needs to be considered separately from blood sugar management.
This latter, Dr. Bikman goes into in great detail, linking insulin resistance (even if blood sugar levels are normal) to all manner of diseases (hence the title).
You may be wondering: how can blood sugar levels be normal, if we have insulin resistance?
And the answer is that for as long as it is still able, your pancreas will just faithfully crank out more and more insulin to deal with the blood sugar levels that would otherwise be steadily rising. Since people measure blood sugar levels much more regularly than anyone checks for actual insulin levels, this means that one can be insulin resistant for years without knowing it, until finally the pancreas is no longer able to keep up with the demand—then that’s when people finally notice.
The book is divided into sections:
- The Problem: What Is Insulin Resistance
- The Cause: What Makes Us Insulin Resistant
- How We Can Fight Insulin Resistance
The first two parts are essential for the reader’s understanding, but the third part is the practical part, with appropriately practical advice on the most insulin-friendly ways to exercise, eat, fast, and more. He also talks drugs, and discusses the pros and cons of various interventions—but of course, far better is the lifestyle management of insulin.
The style is mostly very pop-science in overall presentation, and then occasionally gets very dense at times, but when that happens, he will then tend to follow it with an easier-to-understand explanation, to ensure that nothing remains opaque.
Bottom line: if you care about your metabolic health and don’t mind reading a book where you may have to read a paragraph or two twice sometimes, then this is a top-tier book on insulin resistance and how to prevent/reverse it.
Click here to check out Why We Get Sick, and stay well instead!
Share This Post


Related Posts
-

The Bitter Truth About Coffee (or is it?)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Bitter Truth About Coffee (or is it?)

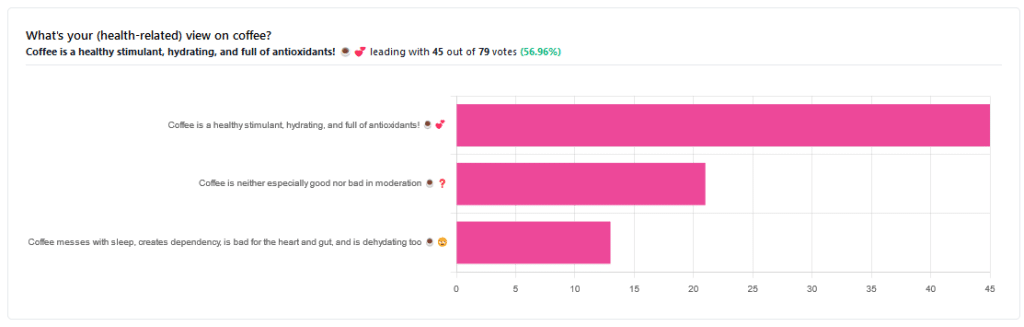
Yesterday, we asked you for your (health-related) views on coffee. The results were clear: if we assume the responses to be representative, we’re a large group of coffee-enthusiasts!
One subscriber who voted for “Coffee is a healthy stimulant, hydrating, and full of antioxidants” wrote:
❝Not so sure about how hydrating it is! Like most food and drink, moderation is key. More than 2 or 3 cups make me buzz! Just too much.❞
And that fine point brings us to our first potential myth:
Coffee is dehydrating: True or False?
False. With caveats…
Coffee, in whatever form we drink it, is wet. This may not come as a startling revelation, but it’s an important starting point. It’s mostly water. Water itself is not dehydrating.
Caffeine, however, is a diuretic—meaning you will tend to pee more. It achieves its diuretic effect by increasing blood flow to your kidneys, which prompts them to release more water through urination.
See: Effect of caffeine on bladder function in patients with overactive bladder symptoms
How much caffeine is required to have a diuretic effect? About 4.5 mg/kg.
What this means in practical terms: if you weigh 70kg (a little over 150lbs), 4.5×70 gives us 315.
315mg is about how much caffeine might be in six shots of espresso. We say “might” because while dosage calculations are an exact science, the actual amount in your shot of espresso can vary depending on many factors, including:
- The kind of coffee bean
- How and when it was roasted
- How and when it was ground
- The water used to make the espresso
- The pressure and temperature of the water
…and that’s all without looking at the most obvious factor: “is the coffee decaffeinated?”
If it doesn’t contain caffeine, it’s not diuretic. Decaffeinated coffee does usually contain tiny amounts of caffeine still, but with nearer 3mg than 300mg, it’s orders of magnitude away from having a diuretic effect.
If it does contain caffeine, then the next question becomes: “and how much water?”
For example, an Americano (espresso, with hot water added to make it a long drink) will be more hydrating than a ristretto (espresso, stopped halfway through pushing, meaning it is shorter and stronger than a normal espresso).
A subscriber who voted for “Coffee messes with sleep, creates dependency, is bad for the heart and gut, and is dehydrating too” wrote:
❝Coffee causes tachycardia for me so staying away is best. People with colon cancer are urged to stay away from coffee completely.❞
These are great points! It brings us to our next potential myth:
Coffee is bad for the heart: True or False?
False… For most people.
Some people, like our subscriber above, have an adverse reaction to caffeine, such as tachycardia. An important reason (beyond basic decency) for anyone providing coffee to honor requests for decaff.
For most people, caffeine is “heart neutral”. It doesn’t provide direct benefits or cause direct harm, provided it is enjoyed in moderation.
See also: Can you overdose on caffeine?
Some quick extra notes…
That’s all we have time for in myth-busting, but it’s worth noting before we close that coffee has a lot of health benefits; we didn’t cover them today because they’re not contentious, but they are interesting nevertheless:
- Coffee is the world’s biggest source of antioxidants
- 65% reduced risk of Alzheimer’s for coffee-drinkers
- 67% reduced risk of type 2 diabetes for coffee-drinkers
- 43% reduced risk of liver cancer for coffee-drinkers
- 53% reduced suicide risk for coffee-drinkers
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Syphilis Is Killing Babies. The U.S. Government Is Failing to Stop the Disease From Spreading.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
ProPublica is a Pulitzer Prize-winning investigative newsroom. Sign up for The Big Story newsletter to receive stories like this one in your inbox.
Karmin Strohfus, the lead nurse at a South Dakota jail, punched numbers into a phone like lives depended on it. She had in her care a pregnant woman with syphilis, a highly contagious, potentially fatal infection that can pass into the womb. A treatment could cure the woman and protect her fetus, but she couldn’t find it in stock at any pharmacy she called — not in Hughes County, not even anywhere within an hour’s drive.
Most people held at the jail where Strohfus works are released within a few days. “What happens if she gets out before I’m able to treat her?” she worried. Exasperated, Strohfus reached out to the state health department, which came through with one dose. The treatment required three. Officials told Strohfus to contact the federal Centers for Disease Control and Prevention for help, she said. The risks of harm to a developing baby from syphilis are so high that experts urge not to delay treatment, even by a day.
Nearly three weeks passed from when Strohfus started calling pharmacies to when she had the full treatment in hand, she said, and it barely arrived in time. The woman was released just days after she got her last shot.
Last June, Pfizer, the lone U.S. manufacturer of the injections, notified the Food and Drug Administration of an “impending stock out” that it anticipated would last a year. The company blamed “an increase in syphilis infection rates as well as competitive shortages.”
Across the country, physicians, clinic staff and public health experts say that the shortage is preventing them from reining in a surge of syphilis and that the federal government is downplaying the crisis. State and local public health authorities, which by law are responsible for controlling the spread of infectious diseases, report delays getting medicine to pregnant people with syphilis. This emergency was predictable: There have been shortages of this drug in eight of the last 20 years.
Yet federal health authorities have not prevented the drug shortages in the past and aren’t doing much to prevent them in the future.
Syphilis, which is typically spread during sex, can be devastating if it goes untreated in pregnancy: About 40% of babies born to women with untreated syphilis can be stillborn or die as newborns, according to the CDC. Infants that survive can suffer from deformed bones, excruciating pain or brain damage, and some struggle to hear, see or breathe. Since this is entirely preventable, a baby born with syphilis is a shameful sign of a failing public health system.
In 2022, the most recent year for which the CDC has data available, more than 3,700 babies were infected with syphilis, including nearly 300 who were stillborn or died as infants. More than 50% of these cases occurred because, even though the pregnant parent was diagnosed with syphilis, they were never properly treated.
That year, there were 200,000 cases identified in the U.S., a 79% increase from five years before. Infection rates among pregnant people and babies increased by more than 250% in that time; South Dakota, where Strohfus works, had the highest rates — including a more than 400% increase among pregnant women. Statewide, the rate of babies born with the disease, a condition known as congenital syphilis, jumped more than 40-fold in just five years.
And that was before the current shortage of shots.
In Mississippi, the state with the second highest rate of syphilis in pregnant women, Dr. Caroline Weinberg started having trouble this summer finding treatments for her clinic’s patients, most of whom are uninsured, live in poverty or lack transportation. She began spending hours each month scouring medicine suppliers’ websites for available doses of the shots, a form of penicillin sold under the brand name Bicillin L-A.
“The way people do it for Taylor Swift, that’s how I’ve been with the Bicillin shortage,” Weinberg said. “Desperately checking the websites to see what I can snag.”
The shortage is driving up infection rates even further.
In a November survey by the National Coalition of STD Directors, 68% of health departments that responded said the drug shortage will cause syphilis rates in their area to increase, further crushing the nation’s most disadvantaged populations.
“This is the most basic medicine,” said Meghan O’Connell, chief public health officer for the Great Plains Tribal Leaders’ Health Board, which represents 18 tribal communities in South Dakota and three other states. “We allow ourselves to continue to not have enough, and it impacts so many people.”
ProPublica examined what the federal government has done to manage the crisis and the ways in which experts say it has fallen short.
The government could pressure Pfizer to be more transparent.
Twenty years ago, there were at least three manufacturers of the syphilis shot. Then Pfizer, one of the manufacturers, purchased the other two companies and became the lone U.S. supplier.
Pfizer’s supply has fallen short since then. In 2016, the company announced a shortage due to a manufacturing issue; it lasted two years. Even during times when Pfizer had not notified the FDA of an official shortage, clinics across the country told ProPublica, the shots were often hard to get.
Several health officials said they would like to see the government use its power as the largest purchaser of the drug to put pressure on Pfizer to produce adequate supplies and to be more transparent about how much of the drug they have on hand, when it will be widely available and how stable the supply will be going forward.
In response to questions, Pfizer said there are two reasons its supply is falling short. One, the company said, was a surge in use of the pediatric form of the drug after a shortage of a different antibiotic last winter. Pfizer also blamed a 70% increase in demand for the adult shots since last February, which it described as unexpected.
Public health experts say the increase in cases and subsequent rise in demand was easy to see coming. Officials have been raising the alarm about skyrocketing syphilis cases for years. “If Pfizer was truly caught completely off guard, it raises significant questions about the competency of the company to forecast obvious infectious disease trends,” a coalition of organizations wrote to the White House Drug Shortage Task Force in September.
Pfizer said it is consistently communicating with the CDC and FDA about its supply and that it has been transparent with public health groups and policymakers.
The FDA has a group dedicated to addressing drug shortages. But Valerie Jensen, associate director of that staff, said the FDA can’t force manufacturers to make more of a drug. “It is up to manufacturers to decide how to respond to that increased demand.” she said. “What we’re here to do is help with those plans.”
Pfizer said it had a target of increasing production by about 20% in 2023 but faced delays toward the end of the year. The company did not explain the reason for those delays.
The company said it has invested $38 million in the last five years in the Michigan facility where it makes the shots and that it is increasing production capacity. It also said it is adding evening shifts at the facility and actively recruiting and training new workers. Pfizer said it also reduced manufacturing time from 110 to 50 days. By the end of June, the company expects the supply to recover, which it described as having eight weeks of inventory based on its forecast demands with no disruptions in sight.
The government could manufacture the drug itself.
Having only one supplier for a drug, especially one of public health importance, makes the country vulnerable to shortages. With just one manufacturer, any disruption — contamination at a plant, a shortage of raw materials, a severe weather event or a flawed prediction of demand — can put lives at risk. What’s ultimately needed, public health experts say, is another manufacturer.
Congressional Democrats recently introduced a bill that would authorize the U.S. Department of Health and Human Services to manufacture generic drugs in exactly this scenario, when there are few manufacturers and regular shortages. Called the Affordable Drug Manufacturing Act, it would also establish an office of drug manufacturing.
This same bill was introduced in 2018, but it didn’t have bipartisan support and was never taken up for a vote. Sen. Elizabeth Warren, the Massachusetts Democrat who introduced the bill in the Senate, said she’s hopeful this time will be different. Lawmakers from both parties understand the risks created by drug shortages, and COVID-19 helped everyone understand the role the government can play to boost manufacturing.
Still, it’s unlikely to be passed with the current gridlock in Congress.
The government could reserve syphilis drugs for infected patients.
Responding to the shortage of shots to treat the disease, the CDC in July asked health care providers nationwide to preserve the scarce remaining doses for people who are pregnant. The shots are considered the gold standard treatment for anyone with syphilis, faster and with fewer side effects than an alternative pill regimen. And for people who are pregnant, the pills are not an option; the shots are the only safe treatment.
Despite that call, the military is giving shots to new recruits who don’t have syphilis, to prevent outbreaks of severe bacterial respiratory infections. The Army has long administered this treatment at boot camps held at Fort Leonard Wood, Fort Moore and Fort Sill. The Army has been unable to obtain the shots several times in the past few years, according to the U.S. Army Center for Initial Military Training. But the Defense Health Agency’s pharmacy operations center has been working with Pfizer to ensure military sites can get them, a spokesperson for the Defense Health Agency said.
“Until we think about public health the way we think about our military, we’re not going to see a difference,” said Dr. John Vanchiere, chief of pediatric infectious diseases at Louisiana State University Health Shreveport.
Some public health officials, including Alaska’s chief medical officer, Dr. Anne Zink, questioned whether the military should be using scarce shots for prevention.
“We should ask if that’s the best use,” she said.
Using antibiotics to prevent streptococcal outbreaks is a well-established, evidence-based public health practice that’s also used by other branches of the armed services, said Lt. Col. Randy Ready, a public affairs officer with the Army’s Initial Military Training center. “The Army continues to work with the CDC and the entire medical community in regards to public health while also taking into account the unique missions and training environments our Soldiers face,” including basic training, Ready said in a written statement.
The government isn’t stockpiling syphilis drugs.
In rare instances, the federal government has created stockpiles of drugs considered key to public health. In 2018, confronting shortages of various drugs to treat tuberculosis, the CDC created a small stockpile of them. And the federal Administration for Strategic Preparedness and Response keeps a national stockpile of supplies necessary for public health emergencies, including vaccines, medical supplies and antidotes needed in case of a chemical warfare attack.
In November, the Biden administration announced it was creating a new syphilis task force. When asked why the federal government doesn’t stockpile syphilis treatments, Adm. Rachel Levine, the HHS official who leads the task force, said officials don’t routinely stockpile drugs, because they have expiration dates.
In a written statement, an HHS spokesperson said that Bicillin has a shelf life of two years and that the Strategic National Stockpile “does not deploy products that are commercially available.” In general, the spokesperson wrote, stockpiles are most effective before a national shortage begins and can’t overcome the problems of limited suppliers or fragile supply chains. “There is also a risk that stockpiles can exacerbate shortages, particularly when supply is already low, by removing drugs from circulation that would have otherwise been available,” the spokesperson wrote.
Stephanie Pang, a senior director with the coalition of STD directors, said that given the critical role of this drug and the severe access concerns, she thinks a stockpile is necessary. “I don’t have another solution that actually gets drugs to patients,” Pang said.
The government could declare a federal emergency.
Some public health officials say the federal government needs to treat the syphilis crisis the way it did Ebola or monkeypox.
Declare a federal emergency, said Dr. Michael Dube, an infectious disease specialist for more than 30 years. That would free up money for more public health staff and fund more creative approaches that could lead to a long-term solution to the near-constant shortages, he said. “I’d hate to have to wait for some horrible anecdotes to get out there in order to get the public’s and the policymakers’ minds on it,” said Dube, who oversees medical care for AIDS Healthcare Foundation wellness clinics across the country.
Citing an alarming surge in syphilis cases, the Great Plains Tribes wrote to the HHS secretary last week asking that the agency declare a public health emergency in their areas. In the request, they asked HHS to work globally to find adequate syphilis treatment and send the needed medicine to the Great Plains region.
During the 2014 outbreak of Ebola in West Africa, Congress gave hundreds of millions of dollars to HHS to help develop new rapid tests and vaccines. Facing a global outbreak of monkeypox in 2022, a White House task force deployed more than a million vaccines, regularly briefed the public and sent extra resources to Pride parades and other places where people at risk were gathered.
Levine, leader of the federal syphilis task force, countered that declaring an emergency wouldn’t make much of a difference. The government, she said, already has a “dramatic and coordinated response” involving several agencies.
The FDA recently approved an emergency import of a similar syphilis treatment made by a French manufacturer that had plenty on hand. According to the company, Provepharm, the imported shots are enough to cover approximately one or two months of typical use by all people in the U.S. (The FDA would not say how many doses Provepharm sent, and the company said it was not allowed to reveal that number under the federal rules governing such emergency imports.)
Clinics applaud that development. But many of them can’t afford the imported shots.
The government could do more to rein in the cost.
Clinics and hospitals that primarily serve low-income patients often qualify for a federal program that allows them to purchase drugs at steeply discounted prices. Pharmaceutical companies that want Medicaid to cover their outpatient drugs must participate in the program.
One factor in determining the discount price is whether a pharmaceutical company has raised the price of a drug by more than the rate of inflation. Because Pfizer has hiked the price of its Bicillin shots significantly over the years, the government requires that it be sold to qualifying clinics for just pennies a dose. Otherwise, a single Pfizer shot can retail for upwards of $500. The French shots are comparable in retail price and not eligible for the discount program.
Several clinic directors also said they worried that drug distributors were reserving the limited supply of the Pfizer shot for organizations that could pay full price. For several days in January, for example, the website of Henry Schein, a medical supplier, showed doses of the shot available at full price, while doses at the penny pricing were out of stock, according to screenshots shared with ProPublica. When asked whether it was only selling shots at full price, a spokesperson for Henry Schein did not respond to the question.
Local health departments that qualify for the discount program told ProPublica they’ve had to pay full price at other distributors, because it was the only stock available.
The Health Resources and Services Administration, the federal agency that regulates the discount program, said that a drug manufacturer is ultimately responsible for ensuring that when supplies are available, they are available at the discounted price. When asked about this, Pfizer said that it has “one inventory that is distributed to our trade partners” and that hospitals and clinics that qualify for the discount program are “responsible for ensuring compliance with the program and orders through the wholesaler accordingly.” The company added, “Pfizer plays no part in this process.”
In October, on Weinberg’s regular search for shots for her Mississippi clinic, she found doses of Bicillin for sale at the discounted price and purchased 40. “The idea that we’re supposed to be hoarding treatment is a horrific compact,” she said. Word got out that the clinic, called Plan A, has some shots, and other clinics began sending pregnant patients there.
The clinic’s supply is dwindling. Weinberg is happy to get the shots to patients who need them. But she’s not sure how much longer her reserve will last — or if she’ll be able to find more when they’re gone.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Intelligence Trap – by David Robson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’re including this one under the umbrella of “general wellness”, because it happens that a lot of very intelligent people make stunningly unfortunate choices sometimes, for reasons that may baffle others.
The author outlines for us the various reasons that this happens, and how. From the famous trope of “specialized intelligence in one area”, to the tendency of people who are better at acquiring knowledge and understanding to also be better at acquiring biases along the way, to the hubris of “I am intelligent and therefore right as a matter of principle” thinking, and many other reasons.
Perhaps the greatest value of the book is the focus on how we can avoid these traps, narrow our bias blind spots, and play to our strengths while paying full attention to our weaknesses.
The style is very readable, despite having a lot of complex ideas discussed along the way. This is entirely to be expected of this author, an award-winning science writer.
Bottom line: if you’d like to better understand the array of traps that disproportionately catch out the most intelligent people (and how to spot such), then this is a great book for you.
Click here to check out The Intelligence Trap, and be more wary!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: