The Best Exercise to Stop Your Legs From Giving Out
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Doug Weiss, seniors-specialist physio, has an exercise that stops your knees from being tricked into collapsing (which is very common) by a misfiring (also common) reflex.
Step up…
Setup to step up thus:
- Use a sturdy support like a countertop or chair.
- Have an aerobic step or similar firm surface to step onto.
When you’re ready:
- Stand facing away from the step.
- Place one hand on the support for stability.
- Step backwards up onto the step with your right leg, then your left leg, so both feet are on the step.
- Step forward to come back down.
Once you’re confident of the series of movements, do it without the support, and do it for a few minutes each day. Don’t worry about how easy it becomes; this is not, first and foremost, a strength-training exercise; you don’t have to start adding weights or anything (although of course you can if you want).
How it works: there’s a part of you called the Golgi tendon organ, and it can trigger a Golgi tendon reflex, which is one of the body’s equivalents of a steam valve. However, instead of letting off steam to avoid a boiler explosion, it collapses a joint to save it from overload. However, if not exercised regularly, it can get overly sensitive, causing it to mistake your mere bodyweight for an overload. So, it collapses, thinking it is saving you from snapping a tendon, but it’s not. By exercising in the way described, the Golgi tendon reflex will go back to only being triggered by an actual overload, not the mere act of stepping.
Meanwhile, for more on all of the above plus a visual demonstration, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
What Nobody Teaches You About Strengthening Your Knees
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Two Patients Faced Chemo. The One Who Survived Demanded a Test To See if It Was Safe

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
JoEllen Zembruski-Ruple, while in the care of New York City’s renowned Memorial Sloan Kettering Cancer Center, swallowed the first three chemotherapy pills to treat her squamous cell carcinoma on Jan. 29, her family members said. They didn’t realize the drug could kill her.
Six days later, Zembruski-Ruple went to Sloan Kettering’s urgent care department to treat sores in her mouth and swelling around her eyes. The hospital diagnosed oral yeast infection and sent her home, her sister and partner said. Two days later, they said, she returned in agony — with severe diarrhea and vomiting — and was admitted. “Enzyme deficiency,” Zembruski-Ruple texted a friend.
The 65-year-old, a patient advocate who had worked for the National Multiple Sclerosis Society and other groups, would never go home.
Covered in bruises and unable to swallow or talk, she eventually entered hospice care and died March 25 from the very drug that was supposed to extend her life, said her longtime partner, Richard Khavkine. Zembruski-Ruple was deficient in the enzyme that metabolizes capecitabine, the chemotherapy drug she took, said Khavkine and Susan Zembruski, one of her sisters. Zembruski-Ruple was among about 1,300 Americans each year who die from the toxic effects of that pill or its cousin, the IV drug fluorouracil known as 5-FU.
Doctors can test for the deficiency — and then either switch drugs or lower the dosage if patients have a genetic variant that carries risk. The FDA approved an antidote in 2015, but it’s expensive and must be administered within four days of the first chemotherapy treatment.
Newer cancer drugs sometimes include a companion diagnostic to determine whether a drug works with an individual patient’s genetics. But 5-FU went on the market in 1962 and sells for about $17 a dose; producers of its generic aren’t seeking approval for toxicity tests, which typically cost hundreds of dollars. Doctors have only gradually understood which gene variants are dangerous in which patients, and how to deal with them, said Alan Venook, a colorectal and liver cancer specialist at the University of California-San Francisco.
By the time Zembruski-Ruple’s doctors told her she had the deficiency, she had been on the drug for eight days, said Khavkine, who watched over his partner with her sister throughout the seven-week ordeal.
Khavkine said he “would have asked for the test” if he had known about it, but added “nobody told us about the possibility of this deficiency.” Zembruski-Ruple’s sister also said she wasn’t warned about the fatal risks of the chemo, or told about the test.
“They never said why they didn’t test her,” Zembruski said. “If the test existed, they should have said there is a test. If they said, ‘Insurance won’t cover it,’ I would have said, ‘Here’s my credit card.’ We should have known about it.”
Guidance Moves at a Glacial Pace
Despite growing awareness of the deficiency, and an advocacy group made up of grieving friends and relatives who push for routine testing of all patients before they take the drug, the medical establishment has moved slowly.
A panel of the National Comprehensive Cancer Network, or NCCN — specialists from Sloan Kettering and other top research centers — until recently did not recommend testing, and the FDA does not require it.
In response to a query from KFF Health News about its policy, Sloan Kettering spokesperson Courtney Nowak said the hospital treats patients “in accordance with NCCN guidelines.” She said the hospital would not discuss a patient’s care.
On Jan. 24, the FDA issued a warning about the enzyme deficiency in which it urged health care providers to “inform patients prior to treatment” about the risks of taking 5-FU and capecitabine.
On March 31 — six days after Zembruski-Ruple’s death — the network’s expert panel for most gastrointestinal cancers took a first step toward recommending testing for the deficiency.
Worried that President Donald Trump’s FDA might do nothing, Venook said, the panel — whose guidance shapes the practices of oncologists and health insurers — recommended that doctors consider testing before dosing patients with 5-FU or capecitabine.
However, its guidance stated that “no specific test is recommended at this time,” citing a lack of data to “inform dose adjustments.”
Sloan Kettering “will consider this guidance in developing personalized treatment plans for each patient,” Nowak told KFF Health News.
The new NCCN guidance was “not the blanket recommendation we were working toward, but it is a major step toward our ultimate goal,” said Kerin Milesky, a public health official in Brewster, Massachusetts, who’s part of an advocacy group for testing. Her husband, Larry, died two years ago at age 73 after a single treatment of capecitabine.
European drug regulators began urging oncologists to test patients for deficiency in May 2020. Patients with potentially risky genetics are started on a half-dose of the cancer drug. If they suffer no major toxicity, the dose is increased.
A Lifesaving Ultimatum?
Emily Alimonti, a 42-year-old biotech salesperson in upstate New York, chose that path before starting capecitabine treatment in December. She said her doctors — including an oncologist at Sloan Kettering — told her they didn’t do deficiency testing, but Alimonti insisted. “Nope,” she said. “I’m not starting it until I get the test back.”
The test showed that Alimonti had a copy of a risky gene variant, so doctors gave her a lower dose of the drug. Even that has been hard to tolerate; she’s had to skip doses because of low white blood cell counts, Alimonti said. She still doesn’t know whether her insurer will cover the test.
Around 300,000 people are treated with 5-FU or capecitabine in the United States each year, but its toxicity could well have prevented FDA approval were it up for approval today. Short of withdrawing a drug, however, U.S. regulators have little power to manage its use. And 5-FU and capecitabine are still powerful tools against many cancers.
At a January workshop that included FDA officials and cancer specialists, Venook, the NCCN panel’s co-chair, asked whether it was reasonable to recommend that doctors obtain a genetic test “without saying what to do with the result.”
But Richard Pazdur, the FDA’s top cancer expert, said it was time to end the debate and commence testing, even if the results could be ambiguous. “If you don’t have the information, how do you have counseling?” he asked.
Two months later, Venook’s panel changed course. The price of tests has fallen below $300 and results can be returned as soon as three days, Venook said. Doubts about the FDA’s ability to further confront the issue spurred the panel’s change of heart, he said.
“I don’t know if FDA is going to exist tomorrow,” Venook told KFF Health News. “They’re taking a wrecking ball to common sense, and that’s one of the reasons we felt we had to go forward.”
On May 20, the FDA posted a Federal Register notice seeking public input on the issue, a move that suggested it was considering further action.
Venook said he often tests his own patients, but the results can be fuzzy. If the test finds two copies of certain dangerous gene variants in a patient, he avoids using the drug. But such cases are rare — and Zembruski-Ruple was one of them, according to her sister and Khavkine.
Many more patients have a single copy of a suspect gene, an ambiguous result that requires clinical judgment to assess, Venook said.
A full-gene scan would provide more information but adds expense and time, and even then the answer may be murky, Venook said. He worries that starting patients on lower doses could mean fewer cures, especially for newly diagnosed colon cancer patients.
Power Should Rest With Patients
Scott Kapoor, a Toronto-area emergency room physician whose brother Anil, a much-loved urologist and surgeon, died of 5-FU toxicity at age 58 in 2023, views Venook’s arguments as medical paternalism. Patients should decide whether to test and what to do with the results, he said.
“What’s better — don’t tell the patient about the test, don’t test them, potentially kill them in 20 days?” he said. “Or tell them about the testing while warning that potentially the cancer will kill them in a year?”
“People say oncologists don’t know what to do with the information,” said Karen Merritt, whose mother died after an infusion of 5-FU in 2014. “Well, I’m not a doctor, but I can understand the Mayo Clinic report on it.”
The Mayo Clinic recommends starting patients on half a dose if they have one suspect gene variant. And “the vast majority of patients will be able to start treatment without delays,” Daniel Hertz, a clinical pharmacologist from the University of Michigan, said at the January meeting.
Some hospitals began testing after patients died because of the deficiency, said Lindsay Murray, of Andover, Massachusetts, who has advocated for widespread testing since her mother was treated with capecitabine and died in 2021.
In some cases, Venook said, relatives of dead patients have sued hospitals, leading to settlements.
Kapoor said his brother — like many patients of non-European origin — had a gene variant that hasn’t been widely studied and isn’t included in most tests. But a full-gene scan would have detected it, Kapoor said, and such scans can also be done for a few hundred dollars.
The cancer network panel’s changed language is disappointing, he said, though “better than nothing.”
In video tributes to Zembruski-Ruple, her friends, colleagues, and clients remembered her as kind, helpful, and engaging. “JoEllen was beautiful both inside and out,” said Barbara McKeon, a former colleague at the MS Society. “She was funny, creative, had a great sense of style.”
“JoEllen had this balance of classy and playful misbehavior,” psychotherapist Anastatia Fabris said. “My beautiful, vibrant, funny, and loving friend JoEllen.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Share This Post
-

The Complete Guide To Red Light Therapy – by Dr. Melanie Gray
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Red light therapy (RLT) is one of those things that sounds like it should be an ineffectual new-age fad that doesn’t do anything, but in fact, there’s a lot of evidence to show that it confers many benefits.
In particular, and to oversimply rather because this is a book review and not a scientific article (though we have written about RLT before and linked to various studies there), RLT is most noted for rejuvenating skin, and enhancing the healing of same, where applicable.
Dr. Gray explains not just what it does, but also some of how it does it, involving the stimulation of mitochondria, DNA-and-telomere repair, and more. She also talks the difference between RLT and near-infrared therapy, which are often delivered by the same devices, just, we can see part of the spectrum and not the other part.
She covers practical matters too, such as optimizing the frequency for different purposes (helpful when choosing a device, or when adjusting the settings on a multi-setting device), as well as optimal treatment duration, and other factors that can affect dosage (including the intensity of the light, and your skintone).
The style is… a little mixed, and can read a little like AI was involved. But on the bright side, it’s a perfectly easy read (and a short one, at 104 pages), and the author’s input includes a lot of niche technical knowledge, which makes it worthwhile. The bibliography is 12 items long and only 5 of those are scholarly articles, but honestly, she could have padded it with a lot more hard-science evidence for RLT’s benefits and it wouldn’t have actually increased the practical value of the book, so we don’t think this is a terrible thing.
Bottom line: this will probably not become anyone’s favorite book, but it is actually useful, and can help you to get the most out of RLT.
Click here to check out The Complete Guide To Red Light Therapy, and enjoy a healthy glow!
Share This Post
-

A Fresh Take On Hypothyroidism
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Three Rs To Boost Thyroid-Related Energy Levels

This is Dr. Izabella Wentz. She’s a doctor of pharmacology, and after her own diagnosis with Hashimoto’s thyroiditis, she has taken it up as her personal goal to educate others on managing hypothyroidism.
Dr. Wentz is also trained in functional medicine through The Institute for Functional Medicine, Kalish Functional Medicine, and the American Academy of Anti-Aging Medicine. She is a Fellow of the American Society of Consultant Pharmacists, and holds certifications in Medication Therapy Management as well as Advanced Diabetes Care through the American Pharmacists Association. In 2013, she received the Excellence in Innovation Award from the Illinois Pharmacists Association.
Dr. Wentz’s mission
Dr. Wentz was disenchanted by the general medical response to hypothyroidism in three main ways. She tells us:
- Thyroid patients are not diagnosed appropriately.
- For this, she criticises over-reliance on TSH tests that aren’t a reliable marker of thyroid function, especially if you have Hashimoto’s.
- Patients should be better optimized on their medications.
- For this, she criticizes many prescribed drugs that are actually pro-drugs*, that don’t get converted adequately if you have an underactive thyroid.
- Lifestyle interventions are often ignored by mainstream medicine.
- Medicines are great; they truly are. But medicating without adjusting lifestyle can be like painting over the cracks in a crumbling building.
*a “pro-drug” is what it’s called when the drug we take is not the actual drug the body needs, but is a precursor that will get converted to that actual drug we need, inside our body—usually by the liver, but not always. An example in this case is T4, which by definition is a pro-drug and won’t always get correctly converted to the T3 that a thyroid patient needs.
Well that does indeed sound worthy of criticism. But what does she advise instead?
First, she recommends a different diagnostic tool
Instead of (or at least, in addition to) TSH tests, she advises to ask for TPO tests (thyroid peroxidase), and a test for Tg antibodies (thyroglobulin). She says these are elevated for many years before a change in TSH is seen.
Next, identify the root cause and triggers
These can differ from person to person, but in countries that add iodine to salt, that’s often a big factor. And while gluten may or may not be a factor, there’s a strong correlation between celiac disease and Hashimoto’s disease, so it is worth checking too. Same goes for lactose.
By “checking”, here we mean testing eliminating it and seeing whether it makes a difference to energy levels—this can be slow, though, so give it time! It is best to do this under the guidance of a specialist if you can, of course.
Next, get to work on repairing your insides.
Remember we said “this can be slow”? It’s because your insides won’t necessarily bounce back immediately from whatever they’ve been suffering from for what’s likely many years. But, better late than never, and the time will pass anyway, so might as well get going on it.
For this, she recommends a gut-healthy diet with specific dietary interventions for hypothyroidism. Rather than repeat ourselves unduly here, we’ll link to a couple of previous articles of ours, as her recommendations match these:
She also recommends regular blood testing to see if you need supplementary TSH, TPO antibodies, and T3 and T4 hormones—as well as vitamin B12.
Short version
After diagnosis, she recommends the three Rs:
- Remove the causes and triggers of your hypothyroidism, so far as possible
- Repair the damage caused to your body, especially your gut
- Replace the thyroid hormones and related things in which your body has become deficient
Learn more
If you’d like to learn more about this, she offers a resource page, with resources ranging from on-screen information, to books you can get, to links to hook you up with blood tests if you need them, as well as recommended supplements to consider.
She also has a blog, which has an interesting relevant article added weekly.
Enjoy, and take care of yourself!
Share This Post
- Thyroid patients are not diagnosed appropriately.


Related Posts
-
How Most People Use Nasal Sprays Incorrectly
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Is this how you’ve been doing it? Here’s the right way:
Like a professional
5 key points to know:
- Proper position: sit upright with your head slightly forwards, not tipped backwards.
- Prime it first: when you first open a new bottle, pump it once or twice until it produces a fine mist; you do not need to prime it again while using that bottle.
- Aim at an angle: place the nozzle well into the nostril, aim backwards and slightly to the side (the nasal cavity goes back, not up).
- Spray correctly: press to release a spray, feel the medicine inside your nasal cavity, and let it sit there. Avoid strong sniffing because that sends the medicine down your throat; a gentle sniff is fine if it starts to run.
- Actually absorb it: keep your head in a neutral position for a few seconds so the spray can absorb, then repeat on the other nostril.
For more on this plus a visual demonstration, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Tips For Putting In Eye Drops (3 Techniques That Work!)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
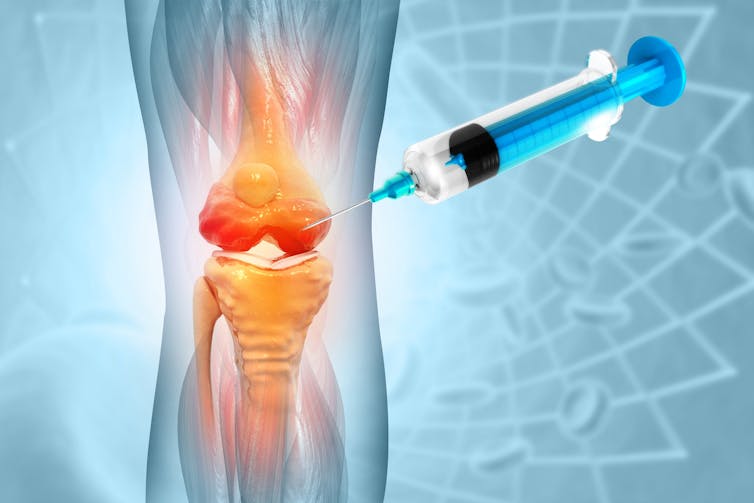
People are getting costly stem cell injections for knee osteoarthritis. But we don’t know if they work
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
More than 500 million people around the world live with osteoarthritis. The knee is affected more often than any other joint, with symptoms (such as pain, stiffness and reduced movement) affecting work, sleep, sport and daily activities.
Knee osteoarthritis is often thought of as thinning of the protective layer of cartilage within the joint. But we now understand it affects all the structures of the joint, including the bones, muscles and nerve endings.
While there are things that can be done to manage the symptoms of knee osteoarthritis, there is no cure, and many people experience persistent pain. As a result, an opportunity exists for as yet unproven treatments to enter the market, often before regulatory safeguards can be put in place.
Stem cell injections are one such treatment. A new review my colleagues and I published this week finds that evidence of their benefits and harms remains elusive.

Marinesea/Shutterstock Stem cell treatments
Stem cells are already established as treatments for some diseases – mostly disorders of the blood, bone marrow or immune system – which has led to suggestions they could be used for a much wider array of conditions.
Stem cells have been touted as promising treatments for osteoarthritis because they have special properties which allow them to replicate and develop into the mature healthy cells that make up our body’s organs and other tissues, including cartilage.
Stem cell treatments for osteoarthritis generally involve taking a sample of tissue from a site that is rich in stem cells (such as bone marrow or fat), treating it to increase the number of stem cells, then injecting it into the joint.
The hope is that if the right type of stem cells can be introduced into an osteoarthritic joint in the right way and at the right time, they may help to repair damaged structures in the joint, or have other effects such as reducing inflammation.
But no matter how convincing the theory, we need good evidence for effectiveness and safety before a new therapy is adopted into practice.
Stem cells have been touted as promising treatments for osteoarthritis. But what does the evidence say? crystal light/Shutterstock Stem cell injections have not been approved by Australia’s Therapeutic Goods Administration for the treatment of osteoarthritis. Nonetheless, some clinics in Australia and around the world still offer them.
Because of the regulatory restrictions, we don’t have reliable numbers on how many procedures are being done.
They’re not covered by Medicare, so the procedure can cost the consumer thousands of dollars.
And, as with any invasive procedure, both the harvest of stem cells and the joint injection procedure may carry the potential for harm, such as infection.
What we found
Our new review, published by the independent, international group the Cochrane Collaboration, looks at all 25 randomised trials of stem cell injections for knee osteoarthritis that have been conducted worldwide to date. Collectively, these studies involved 1,341 participants.
We found stem cell injections may slightly improve pain and function compared with a placebo injection, but the size of the improvement may be too small for the patient to notice.
The evidence isn’t strong enough to determine whether there is any improvement in quality of life following a stem cell injection, whether cartilage regrows, or to estimate the risk of harm.
This means we can’t confidently say yet whether any improvement that might follow a stem cell injection is worth the risk (or the cost).
Osteoarthritis of the knee is the most common type of osteoarthritis. michaelheim/Shutterstock Hope or hype?
It’s not surprising we invest hope in finding a transformative treatment for such a common and disabling condition. Belief in the benefits of stem cells is widespread – more than three-quarters of Americans believe stem cells can relieve arthritis pain and more than half believe this treatment to be curative.
But what happens if a new treatment is introduced to practice before it has been clearly proven to be safe and effective?
The use of an unproven, invasive therapy is not just associated with the risks of the intervention itself. Even if the treatment were harmless, there is the risk of unnecessary cost, inconvenience, and a missed opportunity for the patient to use existing therapies that are known to be effective.
What’s more, if we need to play catch-up to try to establish an evidence base for a treatment that’s already in practice, we risk diverting scarce research resources towards a therapy that may not prove to be effective, simply because the genie is out of the bottle.
There are some ways to manage the symptoms of knee osteoarthritis. PeopleImages.com – Yuri A/Shutterstock Working towards a clearer answer
Several more large clinical trials are currently underway, and should increase our understanding of whether stem cell injections are safe and effective for knee osteoarthritis.
Our review incorporates “living evidence”. This means we will continue to add the results of new trials as soon as they’re published, so the review is always up to date, and offers a comprehensive and trustworthy summary to help people with osteoarthritis and their health-care providers to make informed decisions.
In the meantime, there are a number of evidence-based treatment options. Non-drug treatments such as physiotherapy, regular exercise, maintaining a healthy weight, and cognitive behavioural therapy can be more effective than you think. Anti-inflammatory and pain medications can also play a supporting role.
Importantly, it’s not inevitable that osteoarthritic joints get worse with time. So, even though joint replacement surgery is often highly effective, it’s the last resort and fortunately, many people never need to take this step.
Samuel Whittle, ANZMUSC Practitioner Fellow, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Why is it so shameful to have missing or damaged teeth?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When your teeth and gums are in good condition, you might not even notice their impact on your day-to-day life. Good oral health helps us chew, taste, swallow, speak and convey emotions.
This means the state of your mouth can affect nutrition, confidence, forming relationships and maintaining overall good health and wellbeing.
People who have missing or damaged teeth, or other oral health issues such as gum disease, know this all too well.
They may not only live with pain that affects their sleep, speech and ability to enjoy certain foods, but often also face discrimination and stigma.
So, why is it so shameful to have missing teeth or gum disease? And what can we do about it?
Natalia Lebedinskaia/Getty The social and psychological impact
Oral health is deeply tied to social status. People who don’t have good teeth often face stereotypes about their health, wealth and even their intelligence.
For example, in one 2010 study from the United Kingdom, researchers showed young people photographs of the same person, modified with different levels of tooth decay.
Whenever decayed teeth were visible, participants rated the person lower in intelligence, social skills, confidence, self-esteem and whether they appeared happy – based only on the photo.
These stereotypes can lead to bullying and stigma that scar people for life.
In a recent study with colleagues, we looked at nationally representative data on 4,476 children from the Longitudinal Study of Australian Children.
We found losing teeth to decay or injury was relatively common, affecting one in ten children. These children then had a 42% higher risk of being bullied at school.
These stigmatising experiences can lead to feelings of shame, embarrassment and low self-esteem. In some cases, they can mean people are less likely to seek dental care, fearing further humiliation or blame that they have neglected themselves.
Dental care is often out of reach
Tooth decay and gum disease are the most common oral diseases in Australia and can lead to missing teeth. These conditions can occur at any age, from childhood to adulthood, but they usually worsen with age.
Yet the government’s Child Dental Benefits Schedule only covers dental care for children aged 17 and under whose parents receive government benefits.
Some states and territories also provide oral care for eligible older adults. But long waiting lists show the public system is stretched.
This means oral health care remains inaccessible and unaffordable for many Australians.
Poor oral health affects everyday life
Arguments for improving oral health almost always focus on preventing other physical health conditions. For example, one large study of 172,630 adults in New South Wales found those with missing teeth or poor oral health were more likely to die from heart disease.
Yet when people can’t afford to fix their own oral health issues or their children’s, there can be other serious flow-on effects for their day-to-day life and wellbeing, beyond physical health.
Research shows when people are in pain from tooth decay they are more likely to take days off work and school. This can have long-term negative effects, disrupting education and employment.
Parents may also need to take time off work to take children to the dentist or dental hygienist. They often face financial pressures due to high out-of-pocket costs for dental treatments.
Research shows when people can’t afford dental treatments they may feel powerless to control their circumstances. As a result, they may choose cheaper treatments, such as having a tooth extracted even when it could have been saved.
There has also been a recent surge in people using superannuation to pay for dental treatments, for largely preventable conditions. This will further entrench financial disadvantage.
So, what’s the fix?
Research I conducted with colleagues this year found 96% of working-aged adults in Australia believe oral health care is essential.
But there continue to be significant financial barriers in getting required treatment, particularly for people who are unemployed, have low incomes or those with disability.
So, making dental care more affordable and accessible is an important step. This will encourage timely care and make sure check-ups aren’t a luxury for those who can afford them.
But while dental visits are important, they can’t provide sustainable and long-term protection from oral diseases when the social conditions and behaviours that lead to poor oral health stay the same.
Experiencing stigma because of poor oral health can be highly personal and feel shameful. But the burden to fix this should not be on individuals.
The main causes of oral diseases are behaviours – such as having a lot of sugar, alcohol and tobacco, or poor oral hygiene – and high levels of stress.
We know these behaviours and stress are more common among people who experience social disadvantage.
So we need broader policies that address the social conditions in which people live, work, age and grow – for example, by making access to nutritious food more accessible and affordable.
Reducing disadvantage is the key to addressing both tooth decay and gum disease and the stigma attached to these oral health issues.
Ankur Singh, Chair of Lifespan Oral Health, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: