Staring At The Sun – by Dr. Irvin Yalom
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A quick note first: there are two editions of this book; the content is the same, but the cover is different. So if in your region it has a bright yellow cover and the subtitle is the excitable “Overcoming The Terror Of Death” rather than the more measured “Being At Peace With Your Own Mortality”, that is why; different regional publishers made different choices.
For most of us, dying is the last thing we want to do. We may fear it; we may ignore it; we may try to beat it—but it’s a constant existential threat whether we want it or not.
This book is about “death anxiety”, either direct (conscious fear of impending death) or sublimated (not necessarily realising what we’re avoiding thinking about it). In its broadest sense, the fear of death can be described as rational. But angst about it probably won’t help, so this book looks to help us overcome that.
The style of the book is largely anecdotal, in which the author uses examples from his therapeutic practice to illustrate ways in which the fear of death can manifest, and ways in which it can be managed healthily.
Subjective criticism: while this author developed existential therapy, many of the ideas in this book lean heavily on the psychodynamic approach derived from Freud, and this reviewer isn’t a fan of that. But nevertheless, many of the examples here are thought-provoking and useful, so it is not too strong a criticism.
Bottom line: there are many ways to manage one’s mortality, and this book brings attention to a range of possibilities.
Click here to check out Staring At The Sun, and manage your mortality!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

With Medical Debt Burdening Millions, a Financial Regulator Steps In to Help

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When President Barack Obama signed legislation in 2010 to create the Consumer Financial Protection Bureau, he said the new agency had one priority: “looking out for people, not big banks, not lenders, not investment houses.”
Since then, the CFPB has done its share of policing mortgage brokers, student loan companies, and banks. But as the U.S. health care system turns tens of millions of Americans into debtors, this financial watchdog is increasingly working to protect beleaguered patients, adding hospitals, nursing homes, and patient financing companies to the list of institutions that regulators are probing.
In the past two years, the CFPB has penalized medical debt collectors, issued stern warnings to health care providers and lenders that target patients, and published reams of reports on how the health care system is undermining the financial security of Americans.
In its most ambitious move to date, the agency is developing rules to bar medical debt from consumer credit reports, a sweeping change that could make it easier for Americans burdened by medical debt to rent a home, buy a car, even get a job. Those rules are expected to be unveiled later this year.
“Everywhere we travel, we hear about individuals who are just trying to get by when it comes to medical bills,” said Rohit Chopra, the director of the CFPB whom President Joe Biden tapped to head the watchdog agency in 2021.
“American families should not have their financial lives ruined by medical bills,” Chopra continued.
The CFPB’s turn toward medical debt has stirred opposition from collection industry officials, who say the agency’s efforts are misguided. “There’s some concern with a financial regulator coming in and saying, ‘Oh, we’re going to sweep this problem under the rug so that people can’t see that there’s this medical debt out there,’” said Jack Brown III, a longtime collector and member of the industry trade group ACA International.
Brown and others question whether the agency has gone too far on medical billing. ACA International has suggested collectors could go to court to fight any rules barring medical debt from credit reports.
At the same time, the U.S. Supreme Court is considering a broader legal challenge to the agency’s funding that some conservative critics and financial industry officials hope will lead to the dissolution of the agency.
But CFPB’s defenders say its move to address medical debt simply reflects the scale of a crisis that now touches some 100 million Americans and that a divided Congress seems unlikely to address soon.
“The fact that the CFPB is involved in what seems like a health care issue is because our system is so dysfunctional that when people get sick and they can’t afford all their medical bills, even with insurance, it ends up affecting every aspect of their financial lives,” said Chi Chi Wu, a senior attorney at the National Consumer Law Center.
CFPB researchers documented that unpaid medical bills were historically the most common form of debt on consumers’ credit reports, representing more than half of all debts on these reports. But the agency found that medical debt is typically a poor predictor of whether someone is likely to pay off other bills and loans.
Medical debts on credit reports are also frequently riddled with errors, according to CFPB analyses of consumer complaints, which the agency found most often cite issues with bills that are the wrong amount, have already been paid, or should be billed to someone else.
“There really is such high levels of inaccuracy,” Chopra said in an interview with KFF Health News. “We do not want to see the credit reporting system being weaponized to get people to pay bills they may not even owe.”
The aggressive posture reflects Chopra, who cut his teeth helping to stand up the CFPB almost 15 years ago and made a name for himself going after the student loan industry.
Targeting for-profit colleges and lenders, Chopra said he was troubled by an increasingly corporate higher-education system that was turning millions of students into debtors. Now, he said, he sees the health care system doing the same thing, shuttling patients into loans and credit cards and reporting them to credit bureaus. “If we were to rewind decades ago,” Chopra said, “we saw a lot less reliance on tools that banks used to get people to pay.”
The push to remove medical bills from consumer credit reports culminates two years of intensive work by the CFPB on the medical debt issue.
The agency warned nursing homes against forcing residents’ friends and family to assume responsibility for residents’ debts. An investigation by KFF Health News and NPR documented widespread use of lawsuits by nursing homes in communities to pursue friends and relatives of nursing home residents.
The CFPB also has highlighted problems with how hospitals provide financial assistance to low-income patients. Regulators last year flagged the dangers of loans and credit cards that health care providers push on patients, often saddling them with more debt.
And regulators have gone after medical debt collectors. In December, the CFPB shut down a Pennsylvania company for pursuing patients without ensuring the debts were accurate.
A few months before that, the agency fined an Indiana company working with medical debt for violating collection laws. Regulators said the company had “risked harming consumers by pressuring or inducing them to pay debts they did not owe.”
With their business in the crosshairs, debt collectors are warning that cracking down on credit reporting and other collection tools may prompt more hospitals and doctors to demand patients pay upfront for care.
There are some indications this is happening already, as hospitals and clinics push patients to enroll in loans or credit cards to pay their medical bills.
Scott Purcell, CEO of ACA International, said it would be wiser for the federal government to focus on making medical care more affordable. “Here we’re coming up with a solution that only takes money away from providers,” Purcell said. “If Congress was involved, there could be more robust solutions.”
Chopra doesn’t dispute the need for bigger efforts to tackle health care costs.
“Of course, there are broader things that we would probably want to fix about our health care system,” he said, “but this is having a direct financial impact on so many Americans.”
The CFPB can’t do much about the price of a prescription or a hospital bill, Chopra continued. What the federal agency can do, he said, is protect patients if they can’t pay their bills.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-

The Real Benefit Of Genetic Testing
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Genetic Testing: Health Benefits & Methods
Genetic testing is an oft-derided American pastime, but there’s a lot more to it than finding out about your ancestry!
Note: because there are relatively few companies offering health-related genetic testing services, and we are talking about the benefits of those services, some of this main feature may seem like an advert.
It’s not; none of those companies are sponsoring us, and if any of them become a sponsor at some point, we’ll make it clear and put it in the clearly-marked sponsor segment.
As ever, our only goal here is to provide science-backed information, to enable you to make your own, well-informed, decisions.
Health genomics & genetic testing
The basic goal of health genomics and genetic testing is to learn:
- What genetic conditions you have
- Clearcut genetic conditions, such as Fragile X syndrome, or Huntington’s disease
- What genetic predispositions you have
- Such as an increased/decreased risk for various kinds of cancer, diabetes, heart conditions, and so forth
- What genetic traits you have
- These may range from “blue eyes” to “superathlete muscle type”
- More specifically, pharmacogenomic information
- For example, “fast caffeine metabolizer” or “clopidogrel (Plavix) non-responder” (i.e., that drug simply will not work for you)
Wait, what’s the difference between health genomics and genetic testing?
- Health genomics is the science of how our genes affect our health.
- Genetic testing can be broadly defined as the means of finding out which genes we have.
A quick snippet…
More specifically, a lot of these services look at which single nucleotide polymorphisms (SNPs, pronounced “snips”) we have. While we share almost all of our DNA with each other (and indeed, with most vertebrates), our polymorphisms are the bits that differ, and are the bits that, genetically speaking, make us different.
So, by looking just at the SNPs, it means we “only” need to look at about 3,000,000 DNA positions, and not our entire genome. For perspective, those 3,000,000 DNA positions make up about 0.1% of our whole genome, so without focusing on SNPs, the task would be 1000x harder.
For example, the kind of information that this sort of testing may give you, includes (to look at some “popular” SNPs):
- rs53576 in the oxytocin receptor influences social behavior and personality
- rs7412 and rs429358 can raise the risk of Alzheimer’s disease by more than 10x
- rs6152 can influence baldness
- rs333 resistance to HIV
- rs1800497 in a dopamine receptor may influence the sense of pleasure
- rs1805007 determines red hair and sensitivity to anesthetics
- rs9939609 triggers obesity and type-2 diabetes
- rs662799 prevents weight gain from high fat diets
- rs12255372 linked to type-2 diabetes and breast cancer
- rs1799971 makes alcohol cravings stronger
- rs17822931 determines earwax, sweating and body odor
- rs1333049 coronary heart disease
- rs1051730 and rs3750344 nicotine dependence
- rs4988235 lactose intolerance
(You can learn about these and more than 100,000 other SNPs at SNPedia.com)
I don’t know what SNPs I have, and am disinclined to look them up one by one!
The first step to knowing, is to get your DNA out of your body and into a genetic testing service. This is usually done by saliva or blood sample. This writer got hers done many years ago by 23andMe and was very happy with that service, but there are plenty of other options.
Healthline did an independent review of the most popular companies, so you might like to check out:
Healthline: Best DNA Testing Kits of 2023
Those companies will give you some basic information, such as “6x higher breast cancer risk” or “3x lower age-related macular degeneration risk” etc.
However, to really get bang-for-buck, what you want to do next is:
- Get your raw genetic data (the companies above should provide it); this will probably look like a big text file full of As, Cs, Gs, and Ts, but it make take another form.
- Upload it to Promethease. When this writer got hers done , the cost was $2; that price has now gone up to a whopping $12.
- You will then get a report that will cross-reference your data with everything known about SNPs, and give a supremely comprehensive, readable-to-the-human-eye, explanation of what it all means for you—from much more specific health risk prognostics, to more trivial things like whether you can roll your tongue or smell decomposed asparagus metabolites in urine.
A note on privacy: anything you upload to Promethease will be anonymized, and/but in doing so, you consent to it going into the grand scientific open-source bank of “things we know about the human genome”, and thus contribute to the overall sample size of genetic data.
In our opinion, it means you’re doing your bit for science, without personal risk. But your opinion may differ, and that’s your decision to make.
Lastly, on the pros and cons of pharmacogenetic testing specifically:
Share This Post
- What genetic conditions you have
-

The Case Against Sugar – by Gary Taubes
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We generally already know that sugar is bad for the health. Most people don’t know how bad.
Taubes makes, as the title goes, “the case against sugar”. Implicated in everything from metabolic syndrome to cancer to Alzheimer’s, sugar is ruinous to the health.
It’s hard to review this book without making a comparison to William Duffy’s 1975 bestseller, “Sugar Blues“. Stylistically it’s very similar, and the general gist is certainly the same.
However! Where this book beats Sugar Blues is in content; Duffy’s book often makes bold claims without scientific backing. Some of those claims didn’t stand the test of time and are now disproven. Instead, Taubes’ book leans on actual up-to-date science, and talks more about what we actually know, than what we imagine.
If this book has a weak point, it’s when it veers away from its main topic and starts talking about, for example, saturated fat. In this side-topic, the book makes some good points, but is less well-considered, cherry-picks data, and lacks nuance.
On its main topic, though, the investigation of sugar, it is rather more thorough.
Bottom line: if you want a next-level motivation to reduce or eliminate dietary sugar, this book may certainly provide that.
Click here to check out The Case Against Sugar and reduce a lot of your health risks!
Share This Post
Related Posts
-

The FIRST Program: Fighting Insulin Resistance with Strength Training – by Dr. William Shang
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A lot of advice about fighting insulin resistance focuses on diet. And, that’s worthwhile! How we eat does make a huge difference to our insulin responses (as does fasting). But, we expect our regular 10almonds readers either know these things now, or can read one of several very good books we’ve already reviewed about such.
This one’s different: it focuses, as the title promises, on fighting insulin resistance with strength training. And why?
It’s because of the difference that our body composition makes to our metabolism. Now, our body fat percentage is often talked about (or, less usefully but more prevalently, even if woefully misleadingly, our BMI), but Dr. Shang makes the case for it being our musculature that has the biggest impact; because of how it hastens our metabolism, and because of how it is much healthier for the body to store glycogen in muscle tissue, than just cramming whatever it can into the liver and visceral fat. It becomes relevant, then, that there’s a limit to how much glycogen can be stored in muscle tissue, and that limit is how much muscle you have.
This is not, however, 243 pages to say “lift some weights, lazybones”. Rather, he explains the relevant pathophysiology (we will be more likely to adhere to things we understand, than things we do not), and gives practical advice on exercising the different kinds of muscle fibers, arguing that the whole is greater than the sum of its parts, as well as outlining an exercise program for the gym, plus a chapter on no-gym exercises too.
The style is quite dense, which may be offputting for some, but it suffices to take one’s time and read thoughtfully; the end result is worth it.
Bottom line: if you’d like to keep insulin resistance at bay, this book is an excellent extra tool for that.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

CBD Oil’s Many Benefits
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
CBD Oil: What Does The Science Say?
First, a quick legal (and practical) note:
CBD and THC are both derived from the hemp or cannabis plant, but only the latter has euphoriant psychoactive effects, i.e., will get you high. We’re writing here about CBD derived from hemp and not containing THC (thus, will not get you high).
Laws and regulations differ far too much from place to place for us to try to advise here, so please check your own local laws and regulations. And also, while you’re at it, with your doctor and/or pharmacist.
As ever, this newsletter is for purposes of education and enjoyment, and does not constitute any kind of legal (or medical) advice.
With that in mind, onwards to today’s research review…
CBD for Pain Relief
CBD has been popularly touted as a pain relief panacea, and there are a lot of pop-science articles out there “debunking” this, but…
The science seems to back it up. We couldn’t find studies refuting the claim (of CBD as a viable pain relief option). We did, however, find research showing it was good against:
Note that that latter (itself a research review, not a single study, hence covering a lot of bases) describes it matter-of-factly, with no caveats or weasel-words, as:
“CBD, a non-euphoriant, anti-inflammatory analgesic with CB1 receptor antagonist and endocannabinoid modulating effects”
As a quick note: all of the above is about the topical use of CBD oil, not any kind of ingestion
CBD for Anxiety/Depression
There’s a well-cited study with what honestly we think was a bit of a small sample size, but compelling results within that:
A study published in the Brazilian Journal of Psychiatry tested the anxiety levels of 57 men in a simulated public speaking test.
Compared to placebo…
- Those who received 300mg of CBD experienced significantly reduced anxiety during the test.
- Those who received either 150mg or 600mg of CBD experienced more anxiety during the test than the 300mg group
- This means there’s a sweet spot to the dosage
There was also a clinical study that found CBD to have anti-depressant effects.
The methodology was a lot more robust, but the subjects were mice. We can’t have everything in one study, apparently! There is probably a paucity of human volunteers to have their brain slices looked at after tests, though.
Anyway, what makes this study interesting is that it measured quite an assortment of biological markers in the brain, and found that the CBD had a similar physiological effect to the antidepressant imipramine.
CBD for Treating Opioid Addiction
There are a lot of studies for this, both animal and human, but we’d like to put the spotlight on a human study (with the participation of heroin users) that found:
❝Within one week, CBD significantly reduced cravings, anxiety, resting heart rate, and salivary cortisol levels. No serious adverse effects were found.❞
This is groundbreaking because the very thing about heroin is that it’s so addictive and the body rapidly needs more and more of it. You might think “duh”, but most people don’t realize this part:
Heroin is attractive because it offers (and delivers) an immediate guaranteed “downer”, instant relaxation… with none of the bad side effects of, for example, alcohol. No nausea, no hangover, nothing.
The problem is that the body gets tolerant to heroin very quickly, meaning your doses need to get bigger and more frequent to have the same effect.
Before you know it, what seemed like an affordable “self-medication for a stressful life” is very much out of control! Many doctors have personally found this out the hard way.
So, it’s ruinous:
- first to your financial health, as the costs rapidly spiral
- then to your physical health, as you either suffer from withdrawal or eventually overdose
Consequently, heroin is an incredibly easy drug to get hooked onto, and incredibly difficult to get back off.
So CBD offering relief is really a game-changer.
And more…
CBD has been well-studied and found to be effective for a lot of things, more than we could hope to cover in a single edition here.
Some further reading that may interest you includes:
- CBD against Diabetes in mice / in vitro / in humans
- CBD against neurological diseases (in general, in humans)
- CBD against arthritis in mice / in humans
- CBD specifically against the pain of rheumatoid arthritis / of osteoarthritis
Let us know if there’s any of these (or other) conditions you’d like us to look more into the CBD-related research for, because there’s a lot! You can always hit reply to any of our emails, or use the feedback widget at the bottom
Read (and shop, if you want and it’s permitted where you are):
10 Best CBD Oils of 2023, According to the Forbes Health Advisory Board
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

A short history of sunscreen, from basting like a chook to preventing skin cancer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Australians have used commercial creams, lotions or gels to manage our skin’s sun exposure for nearly a century.
But why we do it, the preparations themselves, and whether they work, has changed over time.
In this short history of sunscreen in Australia, we look at how we’ve slathered, slopped and spritzed our skin for sometimes surprising reasons.
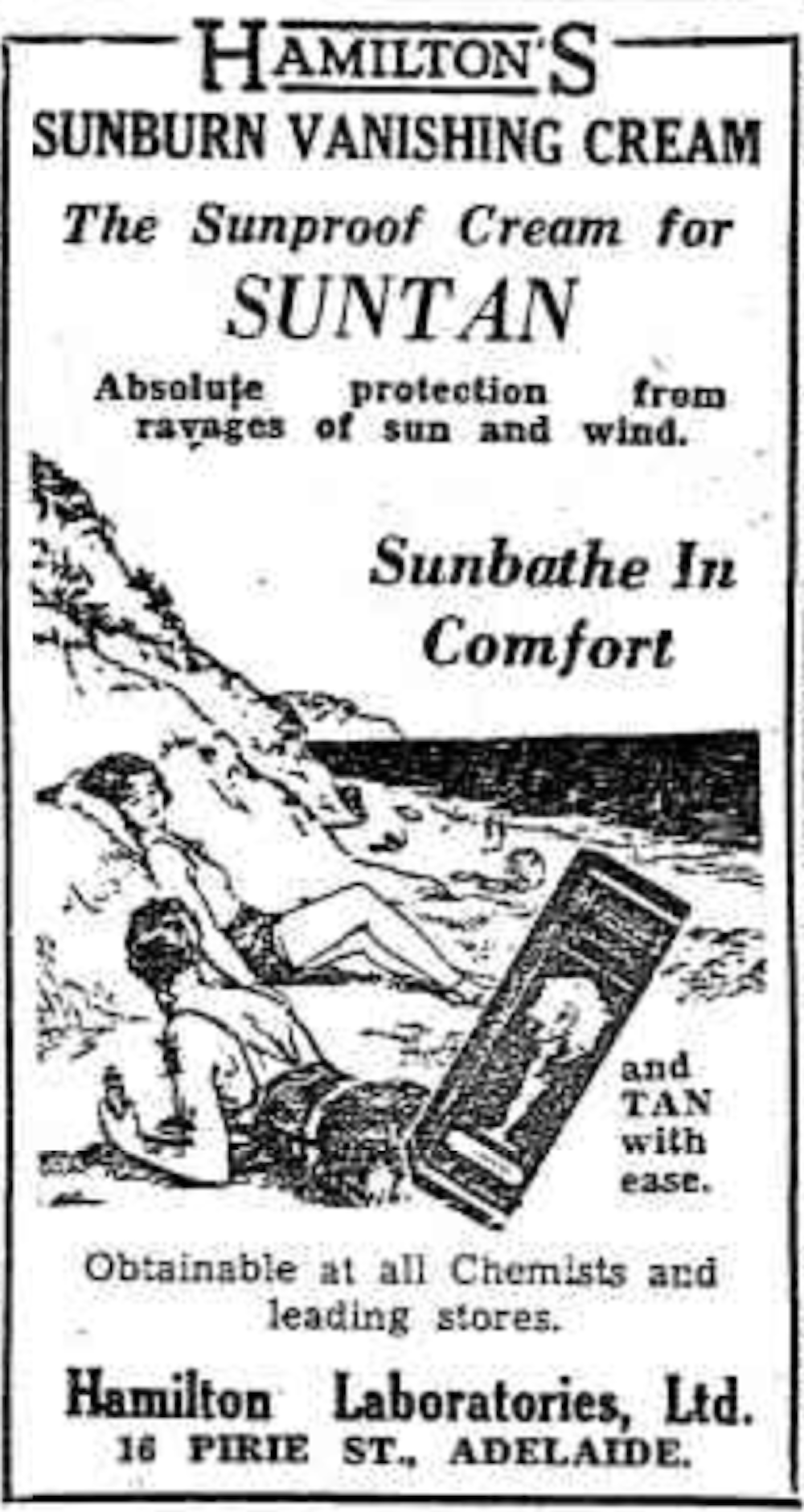
At first, suncreams helped you ‘tan with ease’

This early sunscreen claimed you could ‘tan with ease’.
Trove/NLASunscreens have been available in Australia since the 30s. Chemist Milton Blake made one of the first.
He used a kerosene heater to cook batches of “sunburn vanishing cream”, scented with French perfume.
His backyard business became H.A. Milton (Hamilton) Laboratories, which still makes sunscreens today.
Hamilton’s first cream claimed you could “
Sunbathe in Comfort and TAN with ease”. According to modern standards, it would have had an SPF (or sun protection factor) of 2.The mirage of ‘safe tanning’
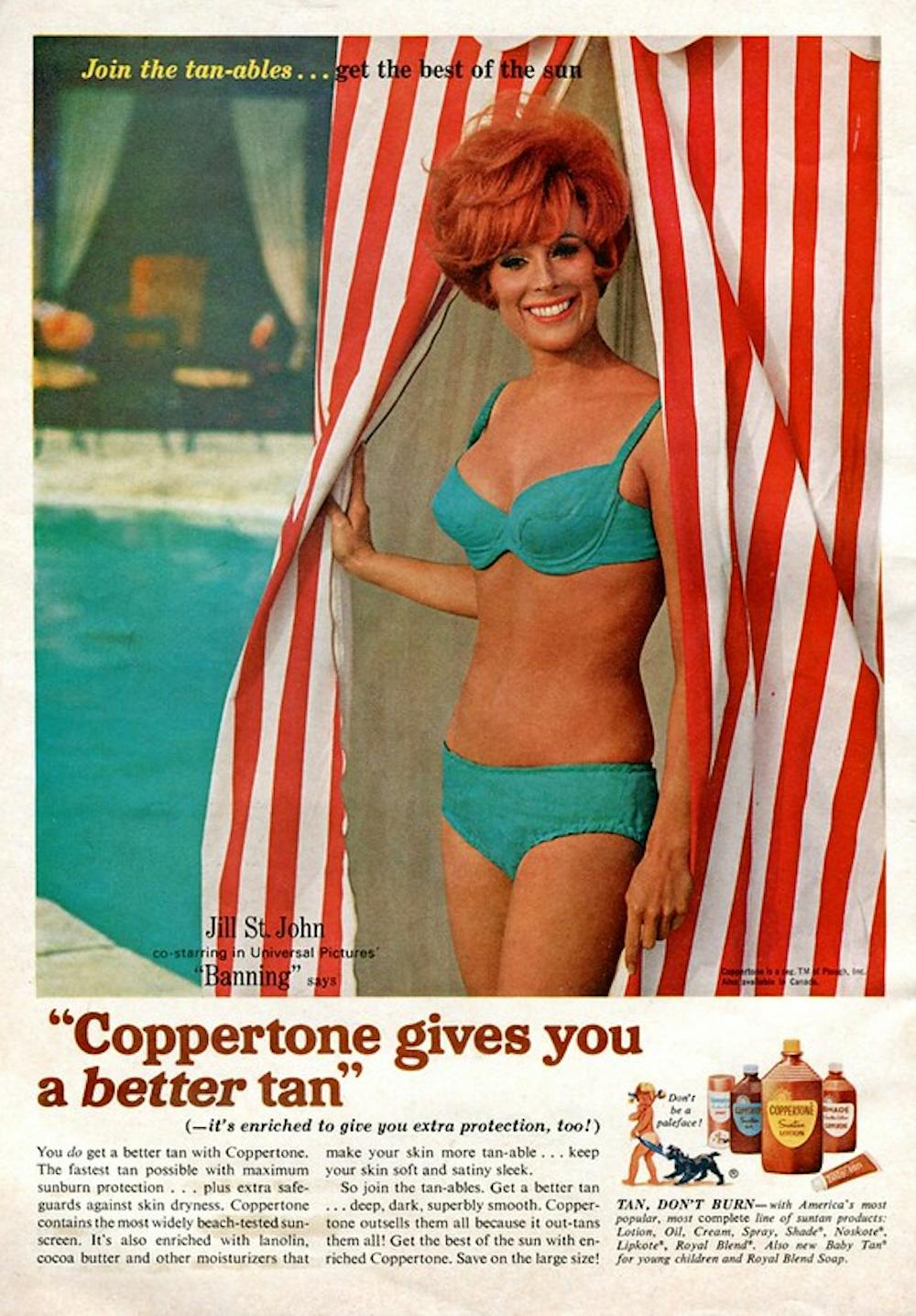
A tan was considered a “modern complexion” and for most of the 20th century, you might put something on your skin to help gain one. That’s when “safe tanning” (without burning) was thought possible.

This 1967 Coppertone advertisement urged you to ‘tan, not burn’.
SenseiAlan/Flickr, CC BY-SASunburn was known to be caused by the UVB component of ultraviolet (UV) light. UVA, however, was thought not to be involved in burning; it was just thought to darken the skin pigment melanin. So, medical authorities advised that by using a sunscreen that filtered out UVB, you could “safely tan” without burning.
But that was wrong.
From the 70s, medical research suggested UVA penetrated damagingly deep into the skin, causing ageing effects such as sunspots and wrinkles. And both UVA and UVB could cause skin cancer.
Sunscreens from the 80s sought to be “broad spectrum” – they filtered both UVB and UVA.
Researchers consequently recommended sunscreens for all skin tones, including for preventing sun damage in people with dark skin.
Delaying burning … or encouraging it?
Up to the 80s, sun preparations ranged from something that claimed to delay burning, to preparations that actively encouraged it to get that desirable tan – think, baby oil or coconut oil. Sun-worshippers even raided the kitchen cabinet, slicking olive oil on their skin.
One manufacturer’s “sun lotion” might effectively filter UVB; another’s merely basted you like a roast chicken.
Since labelling laws before the 80s didn’t require manufacturers to list the ingredients, it was often hard for consumers to tell which was which.
At last, SPF arrives to guide consumers
In the 70s, two Queensland researchers, Gordon Groves and Don Robertson, developed tests for sunscreens – sometimes experimenting on students or colleagues. They printed their ranking in the newspaper, which the public could use to choose a product.
An Australian sunscreen manufacturer then asked the federal health department to regulate the industry. The company wanted standard definitions to market their products, backed up by consistent lab testing methods.
In 1986, after years of consultation with manufacturers, researchers and consumers, Australian Standard AS2604 gave a specified a testing method, based on the Queensland researchers’ work. We also had a way of expressing how well sunscreens worked – the sun protection factor or SPF.
This is the ratio of how long it takes a fair-skinned person to burn using the product compared with how long it takes to burn without it. So a cream that protects the skin sufficiently so it takes 40 minutes to burn instead of 20 minutes has an SPF of 2.
Manufacturers liked SPF because businesses that invested in clever chemistry could distinguish themselves in marketing. Consumers liked SPF because it was easy to understand – the higher the number, the better the protection.
Australians, encouraged from 1981 by the Slip! Slop! Slap! nationwide skin cancer campaign, could now “slop” on a sunscreen knowing the degree of protection it offered.
How about skin cancer?
It wasn’t until 1999 that research proved that using sunscreen prevents skin cancer. Again, we have Queensland to thank, specifically the residents of Nambour. They took part in a trial for nearly five years, carried out by a research team led by Adele Green of the Queensland Institute of Medical Research. Using sunscreen daily over that time reduced rates of squamous cell carcinoma (a common form of skin cancer) by about 60%.
Follow-up studies in 2011 and 2013 showed regular sunscreen use almost halved the rate of melanoma and slowed skin ageing. But there was no impact on rates of basal cell carcinoma, another common skin cancer.
By then, researchers had shown sunscreen stopped sunburn, and stopping sunburn would prevent at least some types of skin cancer.
What’s in sunscreen today?
An effective sunscreen uses one or more active ingredients in a cream, lotion or gel. The active ingredient either works:
-
“chemically” by absorbing UV and converting it to heat. Examples include PABA (para-aminobenzoic acid) and benzyl salicylate, or
-
“physically” by blocking the UV, such as zinc oxide or titanium dioxide.
Physical blockers at first had limited cosmetic appeal because they were opaque pastes. (Think cricketers with zinc smeared on their noses.)
With microfine particle technology from the 90s, sunscreen manufacturers could then use a combination of chemical absorbers and physical blockers to achieve high degrees of sun protection in a cosmetically acceptable formulation.
Where now?
Australians have embraced sunscreen, but they still don’t apply enough or reapply often enough.
Although some people are concerned sunscreen will block the skin’s ability to make vitamin D this is unlikely. That’s because even SPF50 sunscreen doesn’t filter out all UVB.
There’s also concern about the active ingredients in sunscreen getting into the environment and whether their absorption by our bodies is a problem.
Sunscreens have evolved from something that at best offered mild protection to effective, easy-to-use products that stave off the harmful effects of UV. They’ve evolved from something only people with fair skin used to a product for anyone.
Remember, slopping on sunscreen is just one part of sun protection. Don’t forget to also slip (protective clothing), slap (hat), seek (shade) and slide (sunglasses).

Laura Dawes, Research Fellow in Medico-Legal History, Australian National University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-