Overcoming Poor Posture – by Steven Low & Jarlo Ilano
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve previously reviewed the first-named author’s excellent “Overcoming Gravity”, and this time the gymnast-physiotherapist is back with another physio, to deliver us a guide to overcoming poor posture.
They start (after the introductory material you’d expect of any such work) with an examination of the connection between posture and pain, because let’s face it, for most people this is what’s most important.
The authors also do not expect that we live in a world whereby we can devote a lot of time to dedicated postural practice, so they also cover posture in real life, and practical steps to improve posture in the 23.5 (or more) hours per day that you’re mostly not thinking about it.
Which prompts the question: how do we make the change to our regular posture, when indeed we are mostly not thinking about it, and are not likely to start devoting most of our waking thoughts to it? So, again being mindful residents of the real world, the authors also bring us chapters on changing our habits, and redoing our programming, to overcome poor posture in an actually sustainable and thus meaningful fashion.
There are of course specific exercises to do too, but even there, advice is given on how to select those that are most relevant to you, your life, and your body.
Bottom line: if you’d like to be free from the pain caused by the consequences of poor posture, this book can help a lot!
Click here to check out Overcoming Poor Posture, and overcome poor posture, for good!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

New cases of meningococcal disease have been detected. What are the symptoms? And who can get vaccinated?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Two Tasmanian women have been hospitalised with invasive meningococcal disease, bringing the number of cases nationally so far this year to 48. Health authorities are urging people to watch for symptoms and to check if they’re eligible for vaccination.
Invasive meningococcal disease is a rare but life-threatening illness caused by the bacteria Neisseria meningitidis. Invasive means the infection spreads rapidly through the blood and into your organs.
Early emergency medical care is important for survival and to reduce the chance of long-term complications. Even in those who survive, up to 30% suffer permanent cognitive, physical or psychological disabilities.
Thankfully, vaccines are available to protect against it.
How do you catch it?
Around one in ten people carry the meningococcal bacteria in their nose or throats.
The bacteria does not easily pass from person to person by breathing the same air or sharing drinks or food – and the bacteria do not survive well outside the human body.
It is spread through close and prolonged contact of oral and respiratory secretions, such as saliva, from others who live in your household or through deep, intimate kissing.
There is no way to know if you carry the bacteria, as carriers don’t have symptoms.
Who is most at risk?
Meningococcal disease can affect anyone.
But infants under one, adolescents and young adults aged 15–25 years, and people without a spleen or who are immunosuppressed are at a higher risk of developing invasive disease.
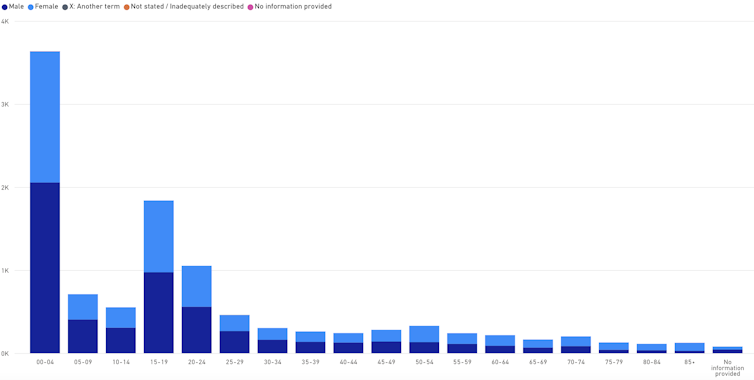
Meningococcal disease notifications by age and sex

Babies and teens are more likely to contract the disease than other age groups. National Notifiable Disease Surveillance System Although sensitive to common antibiotics such as penicillin, the meningococcal bacteria can cause severe infection and death in a matter of hours. The difficulty in picking up meningococcal disease early is that, early on, it can mimic common viral illnesses that people would recover from without any treatment.
Most people experience a sudden onset of fever, difficulty looking at light and/or a rash. The rash is non-blanching, meaning it doesn’t fade when you apply pressure to it. But early in the illness, it can start out as a blanching rash that fades with pressure.
Young infants may also become irritable, have difficulty waking up, or refuse to feed.
The bacteria usually causes a meningitis – inflammation of the lining around the brain and spinal cord – or a bloodstream infection, called septicemia or sepsis. But sometimes it can cause an infection of the bone, lungs (pneumonia) or eyes (conjunctivitis).
Protection against different strains
There are 13 types of meningococcal bacteria that cause invasive disease, but types A, B, C, W and Y cause the most illness.
The rapid disease progression occurs because the bacteria has a sugar capsule which allows it to evade the immune system.
But each of the 13 types has its own unique capsule. So immunity to one strain does not offer immunity to other strains.
Currently, two types of vaccines are available: a vaccine that protects against meningococcal A, C, W and Y (MenACWY); and another vaccine that protects against meningococcal B.
The vaccines are manufactured differently and therefore have different mechanisms of protection.
The MenACWY vaccine uses parts of the sugar capsule within each of the bacteria and joins them to a protein. This is called a “conjugate vaccine” and allows for a better immune response, especially in young infants.
The MenB vaccine does not contain the sugar capsule but includes four other proteins from the surface of the meningococcal B bacteria.
Both vaccines are registered for all people aged six months and older, and are safe for immunocompromised people.
MenACWY vaccine
The MenACWY vaccine is funded under the National Immunisation Program, and given for free, to all infants aged 12 months. There is also a free catch-up program for teens in Year 10.
The MenACWY vaccine protects against disease and also decreases the bacteria load in the throat, reducing the likelihood of transmission to others.
MenB vaccine
The MenB vaccine recommended for all infants aged six weeks or more. But it’s only available for free to infants in South Australia and Queensland, through state-based programs, and to Aboriginal and Torres Strait Islander infants nationally, via the National Immunisation Program.
Parents of non-Indigenous infants in other states will pay around A$220–270 for two doses of the MenB vaccine.
The MenB vaccine is highly protective against invasive disease for the person who receives the vaccine. But it does not eradicate the bacteria from the throat, nor does it decrease spread of the bacteria to others.
Reducing meningococcal disease
Other people who are at high risk of meningococcal exposure are also recommended for vaccination: people without a functional spleen, those with certain immunocompromising conditions, certain travellers and some lab workers.
Since the rollout of the conjugate MenC vaccine in 2001 and the MenACWY in 2018, rates of invasive meningococcal disease have dropped dramatically, from 684 cases in 2002, to 136 cases in 2024. The most common strain to cause disease is now meningococcal B.
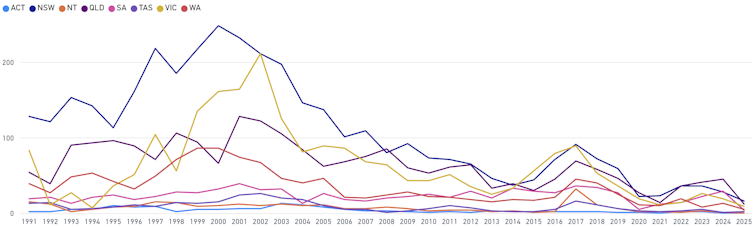
Meningococcal notifications by jurisdiction
Vaccination has reduced case numbers. National Notifiable Disease Surveillance System Another reason for adults to get vaccinated
The MenB vaccine has also been shown to lower rates of another bacterial infection, gonorrhoea, by 33–47%. This is because the gonococcal bacteria is closely related and shares similar surface protein structures to meningococcal bacteria.
In Australia, rates of gonorrhea have doubled over the past ten years , with higher rates among young Aboriginal and Torres Islander people.
The Northern Territory began offering the vaccine to people aged 14 to 19 last year as part of a research trial.
Further research is underway in Australia to better understand the meningococcal bacteria, its capability to evade the immune system and the cross protection against gonorrhoea.
Archana Koirala, Paediatrician and Infectious Diseases Specialist; Clinical Researcher, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Omega-3 Mushroom Spaghetti
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The omega-3 is not the only healthy fat in here; we’re also going to have medium-chain triglycerides, as well as monounsaturates. Add in the ergothioneine from the mushrooms and a stack of polyphenols from, well, most of the ingredients, not to mention the fiber, and this comes together as a very healthy dish. There’s also about 64g protein in the entire recipe, so you do the math for how much that is per serving, depending on how big you want the servings to be.
You will need
- 1lb wholewheat spaghetti (or gluten-free equivalent, such as a legume-based pasta, if avoiding gluten/wheat)
- 12oz mushrooms, sliced (any non-poisonous edible variety)
- ½ cup coconut milk
- ½ onion, finely chopped
- ¼ cup chia seeds
- ¼ bulb garlic, minced (or more, if you like)
- 2 tbsp extra virgin olive oil
- 1 tbsp black pepper, coarse ground
- 1 tbsp lime juice
Method
(we suggest you read everything at least once before doing anything)
1) Cook the spaghetti according to packet instructions, or your own good sense, aiming for al dente. When it’s done, drain it, and lastly rinse it (with cold water), and set it aside.
2) Heat the olive oil in a skillet and add the onion, cooking for 5 minutes
3) Add the garlic, mushrooms, and black pepper, cooking for another 8 minutes.
4) Add the coconut milk, lime juice, and chia seeds, stirring well and cooking for a further two minutes
5) Reheat the spaghetti by passing boiling water through it in a colander (the time it spent cold was good for it; it lowered the glycemic index)
6) Serve, adding the mushroom sauce to the spaghetti:
Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- The Magic of Mushrooms: “The Longevity Vitamin” (That’s Not A Vitamin)
- The Many Health Benefits of Garlic
- Black Pepper’s Impressive Anti-Cancer Arsenal (And More)
- If You’re Not Taking Chia, You’re Missing Out
Take care!
Share This Post
-

Just One Heart – by Dr. Jonathan Fisher
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, what this is not: a book to say eat fiber, go easy on the salt, get some exercise, and so forth.
What this rather is: a book about the connection between the heart and mind; often written poetically, the simple biological reality is that our emotional state does have a genuine impact on our heart health, and as such, any effort to look after our heart (healthwise) would be incomplete without an effort to look after our heart (emotionally).
Dr. Fisher talks about the impact of stress and uncertainty, as well as peace and security, on heart health—and then, having sorted emotional states into “heart breakers” and “heart wakers”, he goes about laying out a plan for what is, emotionally and thus also physiologically, good for our heart.
Chapter by chapter, he walks us through the 7 principles to live by:
- Steadiness: how to steady your heart amid chaos
- Wisdom: how to develop a wise heart in uncertain times
- Openness: how to safely open your heart in a threatening world
- Wholeness: how to show up with your whole heart without going to pieces
- Courage: how to lead with a courageous heart when fear surrounds you
- Lightness: how to live with a light heart in a heavy world
- Warmth: how to love with a warm heart when life feels cold
The style is anything but clinical; it’s well-written, certainly, and definitely informed in part by his medical understanding of the heart, but it’s entirely the raw human element that shines throughout, and that makes the ideas a lot more tangible.
Bottom line: if you’d like your heart to be healthy (cardiac health) and your heart to be healthy (emotional health), this book is a very worthwhile read.
Click here to check out Just One Heart, and take care of yours!
Share This Post


Related Posts
-
Can You Be Fat AND Fit?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The short answer is “yes“.
And as for what that means for your heart and/or all-cause mortality risk: it’s just as good as being fit at a smaller size, and furthermore, it’s better than being less fit at a smaller size.
Here’s the longer answer:
The science
A research team did a systematic review looking at multiple large cohort studies examining the associations between:
- Cardiorespiratory fitness and cardiovascular disease risk
- Cardiorespiratory fitness and all-cause mortality
- BMI and cardiovascular disease risk
- BMI and all-cause mortality
However, they also took this further, and tabulated the data such that they could also establish the cardiovascular disease mortality risk and all-cause mortality risk of:
- Unfit people with “normal” BMI
- Unfit people with “overweight” BMI
- Unfit people with “obese” BMI
- Fit people with “normal” BMI
- Fit people with “overweight” BMI
- Fit people with “obese” BMI
Before we move on, let’s note for the record that BMI is a woeful system in any case, for enough reasons to fill a whole article:
Now, with that in mind, let’s get to the results:
What they found
For cardiovascular disease mortality risk of unfit people specifically, compared to fit people of “normal” BMI:
- Unfit people with “normal” BMI: 2.04x higher risk.
- Unfit people with “overweight” BMI: 2.58x higher risk.
- Unfit people with “obese” BMI: 3.35x higher risk
So here we can see that if you are unfit, then being heavier will indeed increase your CVD mortality risk.
For all-cause mortality risk of unfit people specifically, compared to fit people of “normal” BMI:
- Unfit people with “normal” BMI: 1.92x higher risk.
- Unfit people with “overweight” BMI: 1.82x higher risk.
- Unfit people with “obese” BMI: 2.04x higher risk
This time we see that if you are unfit, then being heavier or lighter than “overweight” will increase your all-cause mortality risk.
So, what about if you are fit? Then being heavier or lighter made no significant difference to either CVD mortality risk or all-cause mortality risk.
Fit individuals, regardless of weight category (normal, overweight, or obese), had significantly lower mortality risks compared to unfit individuals in any weight category.
Note: not just “compared to unfit individuals in their weight category”, but compared to unfit individuals in any weight category.
In other words, if you are obese and have good cardiorespiratory fitness, you will (on average) live longer than an unfit person with “normal” BMI.
You can find the paper itself here, if you want to examine the data and/or method:
Cardiorespiratory fitness, body mass index and mortality: a systematic review and meta-analysis
Ok, so how do I improve the kind of fitness that they measured?
They based their cardiorespiratory fitness on VO2 Max, which scientific consensus holds to be a good measure of how efficiently your body can use oxygen—thus depending on your heart and lungs being healthy.
If you use a fitness tracker that tracks your exercise and your heart rate, it will estimate your VO2 Max for you—to truly measure the VO2 Max itself directly, you’ll need a lot more equipment; basically, access to a lab that tests this. But the estimates are fairly accurate, and so good enough for most personal purposes that aren’t hard-science research.
Next, you’ll want to do this:
53 Studies Later: The Best Way to Improve VO2 Max
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Understanding Cellulitis: Skin And Soft Tissue Infections
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference between a minor passing skin complaint, and a skin condition that’s indicative of something more serious? Dr. Thomas Watchman explains:
More than skin-deep
Cellulitis sounds benign enough, like having a little cellulite perhaps, but in fact it means an infection of the skin and—critically—the underlying soft tissues.
Normally, the skin acts as a barrier against infections, but this barrier can be breached by physical trauma (i.e. an injury that broke the skin), eczema, fungal nail infections, skin ulcers, and other similar things that disrupt the skin’s ability to protect us.
Things to watch out for: Dr. Watchman advises we keep an eye out for warm, reddened skin, swelling, and blisters. Specifically, a golden-yellow crust to these likely indicates a Staphylococcus aureus infection (hence the name).
There’s a scale of degrees of severity:
- Class 1: No systemic toxicity or comorbidities
- Class 2: Systemic toxicity or comorbidities present
- Class 3: Significant systemic toxicity or comorbidities with risk of significant deterioration
- Class 4: Sepsis or life-threatening infection
…with antibiotics being recommended in the latter two cases there, or in other cases for frail, young, old, or immunocompromised patients. Given the rather “scorched earth” results of antibiotics (they cause a lot of collateral iatrogenic damage), this can be taken as a sign of how seriously such infections should be taken.
For more about all this, including visual guides, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Of Brains & Breakouts: The Brain-Skin Doctor
- Beyond Supplements: The Real Immune-Boosters!
- Antibiotics? You Might Want To Think Thrice
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Are GMOs Good Or Bad For Us?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Unzipping Our Food’s Genes
In yesterday’s newsletter, we asked you for your (health-related) views on GMOs.
But what does the science say?
First, a note on terms
Technically, we (humans) have been (g)enetically (m)odifying (o)rganisms for thousands of years.
If you eat a banana, you are enjoying the product of many generations of artificial selection, to change its genes to produce a fruit that is soft, sweet, high in nutrients, and digestible without cooking. The original banana plant would be barely recognizable to many people now (and also, barely edible). We’ve done similarly with countless other food products.
So in this article, we’re going to be talking exclusively about modern genetic modification of organisms, using exciting new (ish, new as in “in the last century”) techniques to modify the genes directly, in a copy-paste fashion.
For more details on the different kinds of genetic modification of organisms, and how they’re each done (including the modern kinds), check out this great article from Sciencing, who explain it in more words than we have room for here:
Sciencing | How Are GMOs Made?
(the above also offers tl;dr section summaries, which are great too)
GMOS are outright dangerous (cancer risks, unknown risks, etc): True or False?
False, so far as we know, in any direct* fashion. Obviously “unknown risks” is quite a factor, since those are, well, unknown. But GMOs on the market undergo a lot of safety testing, and have invariably passed happily.
*However! Glyphosate (the herbicide), on the other hand, has a terrible safety profile and is internationally banned in very many countries for this reason.
Why is this important? Because…
- in the US (and two out of ten Canadian provinces), glyphosate is not banned
- In the US (and we may hypothesize, those two Canadian provinces) one of the major uses of genetic modification of foodstuffs is to make it resistant to glyphosate
- Consequently, GMO foodstuffs grown in those places have generally been liberally doused in glyphosate
So… It’s not that the genetic modification itself makes the food dangerous and potentially carcinogenic (it doesn’t), but it is that the genetic modification makes it possible to use a lot more glyphosate without losing crops to glyphosate’s highly destructive properties.
Which results in the end-consumer eating glyphosate. Which is not good. For example:
❝Following the landmark case against Monsanto, which saw them being found liable for a former groundskeeper, 46 year old Dewayne Johnson’s cancer, 32 countries have to date banned the use of Glyphosate, the key ingredient in Monsanto’s Roundup weed killer. The court awarded Johnson R4.2 billion in damages finding Monsanto “acted with malice or oppression”.❞
Source: see below!
You can read more about where glyphosate is and isn’t banned, here:
33 countries ban the use of Glyphosate—the key ingredient in Roundup
For the science of this (and especially the GMO → glyphosate use → cancer pipeline), see:
Use of Genetically Modified Organism (GMO)-Containing Food Products in Children
GMOs are extra healthy because of the modifications (they were designed for that, right?): True or False?
True or False depending on who made them and why! As we’ve seen above, not all companies seem to have the best interests of consumer health in mind.
However, they can be! Here are a couple of great examples:
❝Recently, two genome-edited crops targeted for nutritional improvement, high GABA tomatoes and high oleic acid soybeans, have been released to the market.
Nutritional improvement in cultivated crops has been a major target of conventional genetic modification technologies as well as classical breeding methods❞
Source: Drs. Nagamine & Ezura
Read in full: Genome Editing for Improving Crop Nutrition
(note, they draw a distinction of meaning between genome editing and genetic modification, according to which of two techniques is used, but for the purposes of our article today, this is under the same umbrella)
Want to know more?
If you’d like to read more about this than we have room for here, here’s a great review in the Journal of Food Science & Nutrition:
Should we still worry about the safety of GMO foods? Why and why not? A review
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: