‘Noisy’ autistic brains seem better at certain tasks. Here’s why neuroaffirmative research matters
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Pratik Raul, University of Canberra; Jeroen van Boxtel, University of Canberra, and Jovana Acevska, University of Canberra
Autism is a neurodevelopmental difference associated with specific experiences and characteristics.
For decades, autism research has focused on behavioural, cognitive, social and communication difficulties. These studies highlighted how autistic people face issues with everyday tasks that allistic (meaning non-autistic) people do not. Some difficulties may include recognising emotions or social cues.
But some research, including our own study, has explored specific advantages in autism. Studies have shown that in some cognitive tasks, autistic people perform better than allistic people. Autistic people may have greater success in identifying a simple shape embedded within a more complex design, arranging blocks of different shapes and colours, or spotting an object within a cluttered visual environment (similar to Where’s Wally?). Such enhanced performance has been recorded in babies as young as nine months who show emerging signs of autism.
How and why do autistic individuals do so well on these tasks? The answer may be surprising: more “neural noise”.
What is neural noise?
Generally, when you think of noise, you probably think of auditory noise, the ups and downs in the amplitude of sound frequencies we hear.
A similar thing happens in the brain with random fluctuations in neural activity. This is called neural noise.
This noise is always present, and comes on top of any brain activity caused by things we see, hear, smell and touch. This means that in the brain, an identical stimulus that is presented multiple times won’t cause exactly the same activity. Sometimes the brain is more active, sometimes less. In fact, even the response to a single stimulus or event will fluctuate continuously.
Neural noise in autism
There are many sources of neural noise in the brain. These include how the neurons become excited and calm again, changes in attention and arousal levels, and biochemical processes at the cellular level, among others. An allistic brain has mechanisms to manage and use this noise. For instance, cells in the hippocampus (the brain’s memory system) can make use of neural noise to enhance memory encoding and recall.
Evidence for high neural noise in autism can be seen in electroencephalography (EEG) recordings, where increased levels of neural fluctuations were observed in autistic children. This means their neural activity is less predictable, showing a wider range of activity (higher ups and downs) in response to the same stimulus.
In simple terms, if we imagine the EEG responses like a sound wave, we would expect to see small ups and downs (amplitude) in allistic brains each time they encounter a stimulus. But autistic brains seem to show bigger ups and downs, demonstrating greater amplitude of neural noise.
Many studies have linked this noisy autistic brain with cognitive, social and behavioural difficulties.
But could noise be a bonus?
The diagnosis of autism has a long clinical history. A shift from the medical to a more social model has also seen advocacy for it to be reframed as a difference, rather than a disorder or deficit. This change has also entered autism research. Neuroaffirming research can examine the uniqueness and strengths of neurodivergence.
Psychology and perception researcher David Simmons and colleagues at the University of Glasgow were the first to suggest that while high neural noise is generally a disadvantage in autism, it can sometimes provide benefits due to a phenomenon called stochastic resonance. This is where optimal amounts of noise can enhance performance. In line with this theory, high neural noise in the autistic brain might enhance performance for some cognitive tasks.
Our 2023 research explores this idea. We recruited participants from the general population and investigated their performance on letter-detection tasks. At the same time, we measured their level of autistic traits.
We performed two letter-detection experiments (one in a lab and one online) where participants had to identify a letter when displayed among background visual static of various intensities.
By using the static, we added additional visual noise to the neural noise already present in our participants’ brains. We hypothesised the visual noise would push participants with low internal brain noise (or low autistic traits) to perform better (as suggested by previous research on stochastic resonance). The more interesting prediction was that noise would not help individuals who already had a lot of brain noise (that is, those with high autistic traits), because their own neural noise already ensured optimal performance.
Indeed, one of our experiments showed people with high neural noise (high autistic traits) did not benefit from additional noise. Moreover, they showed superior performance (greater accuracy) relative to people with low neural noise when the added visual static was low. This suggests their own neural noise already caused a natural stochastic resonance effect, resulting in better performance.
It is important to note we did not include clinically diagnosed autistic participants, but overall, we showed the theory of enhanced performance due to stochastic resonance in autism has merits.
Why this is important?
Autistic people face ignorance, prejudice and discrimination that can harm wellbeing. Poor mental and physical health, reduced social connections and increased “camouflaging” of autistic traits are some of the negative impacts that autistic people face.
So, research underlining and investigating the strengths inherent in autism can help reduce stigma, allow autistic people to be themselves and acknowledge autistic people do not require “fixing”.
The autistic brain is different. It comes with limitations, but it also has its strengths.
Pratik Raul, PhD candidiate, University of Canberra; Jeroen van Boxtel, Associate professor, University of Canberra, and Jovana Acevska, Honours Graduate Student, University of Canberra
This article is republished from The Conversation under a Creative Commons license. Read the original article.

Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How community health screenings get more people of color vaccinated

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
U.S. preventive health screening rates dropped drastically at the height of the COVID-19 pandemic. They have yet to go back to pre-pandemic levels, especially for Black and Latine communities.
Screenings, or routine medical checkups, are important ways to avoid and treat disease. They’re key to finding problems early on and can even help save people’s lives.
Community health workers say screenings are also a key to getting more people vaccinated. Screening fairs provide health workers the chance to build rapport and trust with the communities they serve, while giving their clients the chance to ask questions and get personalized recommendations according to their age, gender, and family history.
But systemic barriers to health care can often keep people from marginalized communities from accessing recommended screenings, exacerbating racial health disparities.
Public Good News spoke with Dr. Marie-Jose Francois, president and chief executive officer, and April Johnson, outreach coordinator, at the Center for Multicultural Wellness and Prevention (CMWP), in Central Florida, to learn how they promote the benefits of screening and leverage screenings for vaccination outreach among their diverse communities.
Here’s what they said.
[Editor’s note: This content has been edited for clarity and length.]
PGN: What is CMWP’s mission? How does vaccine outreach fit into the work you do in the communities you serve?
Dr. Marie-Jose Francois: Since 1995, our mission has been to enhance the health, wellness, and quality of life for diverse populations in Central Florida. At the beginning, our main focus was education, wellness, and screening for HIV/AIDS, and we continue to do case management for HIV screening and testing.
When the issue of COVID-19 came into the picture, we included COVID-19 information and education and stressed the importance of screening and receiving vaccinations during all of our outreach activities.
We try to meet the community where they are. Because there is so much misconception—and taboo—in regard to immunization.
April Johnson: So our job is to disperse accurate information. And how we do that is we go into rural communities. We build partnerships with local apartment complexes, hair salons, nail salons, laundromats, and provide a little community engagement, where people just hang out in different areas.
We build gatekeepers in those communities because you first have to get in there. You have to know that they trust you. Being in this field for about 30 years, I’ve [learned that] flexibility is key. Because sometimes you can’t get them from 9 to 5, or [from] Monday through Friday. So, you have to be very flexible in doing the outreach portion in order to get what you need.
I’ve built collaborations with senior citizen centers, community centers, schools, clinics, churches in Orlando and [in] different areas in Orange, Osceola, Seminole, and Lake counties. And we also partner with other community-based organizations to try to make it like a one-stop shop. So, partnership is a big thing.
PGN: How do you promote the importance of preventive screenings in the communities you serve?
M.F.: We try to make them view their health in a more comprehensive way, for them to understand the importance of screening. [That] self care is key, and for them to not be afraid.
We empower them to know what to ask when they go to the doctor. We ask them, ‘Do you know your status? Do you know your numbers?’
For example, if you go to the doctor, do you know your blood pressure? If you’re diabetic? Do you know your hemoglobin (A1C)? Do you know your cholesterol levels?
And now, [we also ask them]: ‘Have you received your flu shot for the year? Have you received all of your vaccine doses for COVID-19?’ We are even adding the mpox vaccine now, based on risk factors.
[We recommend they] ask their provider. For women, [we ask], ‘When do you need to have your mammogram?’ For the men, ‘You need to ask about your PSA and also about when and when to have your colonoscopy based on your age.’
We also try to explain to the community that the more they know their family history, the more they can engage in their own health. Because sometimes you have mom and dad who have a history of cancer. They have a history of diabetes or blood pressure—and they don’t talk to their children. So, we try to [recommend they] talk to their children. Your own family needs to know what’s going on so they can be proactive in their screenings.
PGN: What strategies or methods have you found most effective in getting people screened?
M.F.: Not everybody wants to be screened, not everybody wants to receive vaccines.
But with patience, just give them the facts. It goes right back to education, people have to be assured.
When you talk to them about COVID, or even HIV, you may hear them say, ‘Oh, I don’t see myself at risk for HIV.’ But we have to repeat to them that the more they get screened to make sure they’re OK, the better it is for them. ‘The more you use condoms, [the] safer it is for you.’
In Haitian culture, they listen to the radio. So we use the radio as a tool to educate and deliver information [to] get vaccinated, wash your hands. ‘If you’re coughing, cover your mouth. If you have a fever, wear your masks. Call your doctor.’
In our target population, we have people who have chronic conditions. We have people with HIV. So, we have to motivate them to receive the flu vaccine, to receive the COVID vaccine, to receive that RSV [vaccine], or to get the mpox vaccine. We have people with diabetes, high blood pressure, high cholesterol, depressed immune systems. We have people with lupus, we have people with sickle cell disease.
So, this is a way to [ensure that] whomever you’re talking to one-on-one understands the value of being safe.
This article first appeared on Public Good News and is republished here under a Creative Commons license.

Share This Post
-

What Are Nootropics, Really?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What are nootropics, really?
A nootropic is anything that functions as a cognitive enhancer—in other words, improves our brainpower.
These can be sensationalized as “smart drugs”, misrepresented excitingly in science fiction, meme-ified in the mundane (“but first, coffee”), and reframed entirely, (“exercise is the best nootropic”).
So, clearly, “nootropics” can mean a lot of different things. Let’s look at some of the main categories…
The neurochemical modulators
These are what often get called “smart drugs”. They are literally drugs (have a chemical effect on the body that isn’t found in our diet), and they affect the levels of certain neurotransmitters in the brain, such as by:
- Adding more of that neurotransmitter (simple enough)
- Decreasing the rate at which we lose that neurotransmitter (re-uptake inhibitors)
- Antagonizing an unhelpful neurotransmitter (doing the opposite thing to it)
- Blocking an unhelpful neurotransmitter (stopping the receptors from receiving it)
“Unhelpful” here is relative and subjective, of course. We need all the neurotransmitters that are in our brain, after all, we just don’t need all of them all the time.
Examples: modafinil, a dopamine re-uptake inhibitor (mostly prescribed for sleep disorders), reduces the rate at which our brains scrub dopamine, resulting in a gradual build-up of dopamine that we naturally produced, so we get to enjoy that dopamine for longer. This will tend to promote wakefulness, and may also help with problem-solving and language faculties—as well as giving a mood boost. In other words, all things that dopamine is used for. Mirtazaрine, an adrenoreceptor agonist (mostly prescribed as an antidepressant), increases noradrenergic neurotransmission, thus giving many other brain functions a boost.
Why it works: our brains need healthy levels of neurotransmitters, in order to function well. Those levels are normally self-regulating, but can become depleted in times of stress or fatigue, for example.
The metabolic brain boosters
These are the kind of things that get included in nootropic stacks (stack = a collection of supplements and/or drugs that complement each other and are taken together—for example, a multivitamin tablet could be described as a vitamin stack) even though they have nothing specifically relating them to brain function. Why are they included?
The brain needs so much fuel. Metabolically speaking, it’s a gas-guzzler. It’s the single most resource-intensive organ of our body, by far. So, metabolic brain boosters tend to:
- Increase blood flow
- Increase blood oxygenation
- Increase blood general health
- Improve blood pressure (this is relative and subjective, since very obviously there’s a sweet spot)
Examples: B-vitamins. Yep, it can be that simple. A less obvious example might be Co-enzyme Q10, which supports energy production on a cellular level, and good cardiovascular health.
Why it works: you can’t have a healthy brain without a healthy heart!
We are such stuff as brains are made of
Our brains are made of mostly fat, water, and protein. But, not just any old fat and protein—we’re at least a little bit special! So, brain-food foods tend to:
- Give the brain the fats and proteins it’s made of
- Give the brain the stuff to make the fats and proteins it’s made of (simpler fats, and amino acids)
- Give the brain hydration! Just having water, and electrolytes as appropriate, does this
Examples: healthy fats from nuts, seeds, and seafood; also, a lot of phytonutrients from greens and certain fruits. Long-time subscribers may remember our article “Brain Food: The Eyes Have It!” on the importance of dietary lutein in reducing Alzheimer’s risk, for example
Why it works: this is matter of structural upkeep and maintenance—our brains don’t work fabulously if deprived of the very stuff they’re made of! Especially hydration is seriously underrated as a nootropic factor, by the way. Most people are dehydrated most of the time, and the brain dehydrates quickly. Fortunately, it rehydrates quickly as well when we take hydrating liquids.
Weird things that sound like ingredients in a witch’s potion
These are too numerous and too varied in how they work to cover here, but they do appear a lot in nootropic stacks and in popular literature on the subject.
Often they work by one of the mechanisms described above; sometimes we’re not entirely sure how they work, and have only measured their effects sufficiently to know that, somehow, they do work.
Examples: panax ginseng is one of the best-studied examples that still remains quite mysterious in many aspects of its mechanism. Lion’s Mane (the mushroom, not the jellyfish or the big cat hairstyle), meanwhile, is known to contain specific compounds that stimulate healthy brain cell growth.
Why it works: as we say, it varies so much from on ingredient to another in this category, so… Watch out for our Research Review Monday features, as we’ll be covering some of these in the coming weeks!
(PS, if there’s any you’d like us to focus on, let us know! We always love to hear from you. You can hit reply to any of our emails, or use the handy feedback widget at the bottom)
Share This Post
-
Is it true foods with a short ingredient list are healthier? A nutrition expert explains
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
At the end of a long day, who has time to check the detailed nutrition information on every single product they toss into their shopping basket?
To eat healthily, some people prefer to stick to a simple rule: choose products with a short ingredient list. The idea is foods with just a few ingredients are less processed, more “natural” and therefore healthy.
But is this always the case? Here’s what the length of an ingredient list can and can’t tell you about nutrition – and what else to look for.
Hryshchyshen Serhii/Shutterstock How ingredient lists work
You can find an ingredient list on most packaged food labels, telling you the number and type of ingredients involved in making that food.
In Australia, packaged food products must follow certain rules set by the Australian and New Zealand Food Standards Code.
Ingredients must be listed in order of ingoing weight. This means items at the beginning of the list are those that make up the bulk of the product. Those at the end make up the least.
Food labels also include a nutrition information panel, which tells you the quantity of key nutrients (energy, protein, total carbohydrates, sugars, total fat, saturated fat and sodium) per serving.
This panel also tells you the content per 100 grams or millilitres, which allows you to work out the percentage.
Whole foods can be packaged, too
Products with just one, two or three items in their ingredient list are generally in a form that closely reflects the food when it was taken from the farm. So even though they come in packaging, they could be considered whole foods.
“Whole foods” are those that have undergone zero to minimal processing, such as fresh fruit and vegetables, lentils, legumes, whole grains such as oats or brown rice, seeds, nuts and unprocessed meat and fish.
To support overall health, the Australian Dietary Guidelines recommend eating whole foods and limiting those that are highly processed.
Many whole foods, such as fresh fruits and vegetables, don’t have an ingredient list because they don’t come in a packet. But some do, including:
- canned or frozen vegetables, such as a tin of black beans or frozen peas
- canned fish, for example, tuna in springwater
- plain Greek yoghurt.
These sorts of food items can contribute every day to a healthy balanced diet.
What is an ultra-processed food?
A shorter ingredient list also means the product is less likely to be an ultra-processed food.
This describes products made using industrial processes that combine multiple ingredients, often including colours, flavours and other additives. They are hyperpalatable, packaged and designed for convenience.
Ultra-processed foods often have long ingredient lists, due to added sugars (such as dextrose), modified oils, protein sources (for example, soya protein isolate) and cosmetic additives – such as colours, flavours and thickeners.
Some examples of ultra-processed foods with long ingredient lists include:
- meal-replacement drinks
- plant-based meat imitations
- some commercial bakery items, including cookies or cakes
- instant noodle snacks
- energy or performance drinks.
If a food is heavily branded and marketed it’s more likely to be an ultra-processed food – a created product, rather than a whole food that hasn’t changed much since the farm.
Nutrition is more than a number
Choosing products with a shorter ingredient list can work as a general rule of thumb. But other factors matter too.
The length of an ingredient list doesn’t tell us anything about the food’s nutritional content, so it’s important to consider the type of ingredients as well.
Remember that items are listed in order of their ingoing weight, so if sugar is second or third on the list, there is probably a fair bit of added sugar.
For instance, a food product may have only a few ingredients, but if the first, second or third is a type of fat, oil or sugar, then it may not be an ideal choice for every day.
You can also check the nutrition information panel. Use the “per serve” column to check the nutrients you’d get from eating one serve of the food. If you want to compare the amount of a nutrient in two different foods, it’s best to look at the per 100g/mL column.
Some examples of foods with relatively short ingredient lists but high amounts of added fats and sugars include:
- potato crisps
- chocolate
- soft drink.
Alcoholic beverages such as beer or wine may also have only a few ingredients, but this does not mean that they should be consumed every day.
Non-food ingredients
You can also keep an eye out for cosmetic ingredients, which don’t have any nutritional value. These include colours, flavours, emulsifiers, thickeners, sweeteners, bulking agents and gelling agents.
It sometimes takes a bit of detective work to spot cosmetic ingredients in the list, as they can come under many different names (for example, stabiliser, malted barley extract, methylcellulose). But they are usually always recognisable as non-food items.
If there are multiple non-food items included in an ingredient list, there is a good chance the food is ultra-processed and not ideal as an everyday choice.
The bottom line? Choosing foods with a shorter ingredient list can help guide you choose less processed foods. But you should also consider what type of ingredients are being used and maintain a varied diet.
Margaret Murray, Senior Lecturer, Nutrition, Swinburne University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post




-

Pasteurization: What It Does And Doesn’t Do
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Pasteurization’s Effect On Risks & Nutrients
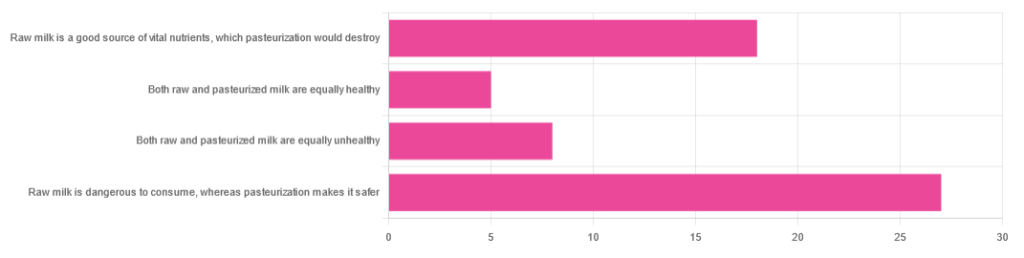
In Wednesday’s newsletter, we asked you for your health-related opinions of raw (cow’s) milk, and got the above-depicted, below-described, set of responses:
- About 47% said “raw milk is dangerous to consume, whereas pasteurization makes it safer”
- About 31% said “raw milk is a good source of vital nutrients which pasteurization would destroy”
- About 14% said “both raw milk and pasteurized milk are equally unhealthy”
- About 9% said “both raw milk and pasteurized milk are equally healthy”
Quite polarizing! So, what does the science say?
“Raw milk is dangerous to consume, whereas pasteurization makes it safer: True or False?”
True! Coincidentally, the 47% who voted for this are mirrored by the 47% of the general US population in a similar poll, deciding between the options of whether raw milk is less safe to drink (47%), just as safe to drink (15%), safer to drink (9%), or not sure (30%):
Public Fails to Appreciate Risk of Consuming Raw Milk, Survey Finds
As for what those risks are, by the way, unpasteurized dairy products are estimated to cause 840x more illness and 45x more hospitalizations than pasteurized products.
This is because unpasteurized milk can (and often does) contain E. coli, Listeria, Salmonella, Cryptosporidium, and other such unpleasantries, which pasteurization kills.
Source for both of the above claims:
(we know the title sounds vague, but all this information is easily visible in the abstract, specifically, the first two paragraphs)
Raw milk is a good source of vital nutrients which pasteurization would destroy: True or False?
False! Whether it’s a “good” source can be debated depending on other factors (e.g., if we considered milk’s inflammatory qualities against its positive nutritional content), but it’s undeniably a rich source. However, pasteurization doesn’t destroy or damage those nutrients.
Incidentally, in the same survey we linked up top, 16% of the general US public believed that pasteurization destroys nutrients, while 41% were not sure (and 43% knew that it doesn’t).
Note: for our confidence here, we are skipping over studies published by, for example, dairy farming lobbies and so forth. Those do agree, by the way, but nevertheless we like sources to be as unbiased as possible. The FDA, which is not completely unbiased, has produced a good list of references for this, about half of which we would consider biased, and half unbiased; the clue is generally in the journal names. For example, Food Chemistry and the Journal of Food Science and Journal of Nutrition are probably less biased than the International Dairy Association and the Journal of Dairy Science:
FDA | Raw Milk Misconceptions and the Danger of Raw Milk Consumption
this page covers a lot of other myths too, more than we have room to “bust” here, but it’s very interesting reading and we recommend to check it out!
Notably, we also weren’t able to find any refutation by counterexample on PubMed, with the very slight exception that some studies sometimes found that in the case of milks that were of low quality, pasteurization can reduce the vitamin E content while increasing the vitamin A content. For most milks however, no significant change was found, and in all cases we looked at, B-vitamins were comparable and vitamin D, popularly touted as a benefit of cow’s milk, is actually added later in any case. And, importantly, because this is a common argument, no change in lipid profiles appears to be findable either.
In science, when something has been well-studied and there aren’t clear refutations by counterexample, and the weight of evidence is clearly very much tipped into one camp, that usually means that camp has it right.
Milk generally is good/bad for the health: True or False?
True or False, depending on what we want to look at. It’s definitely not good for inflammation, but the whole it seems to be cancer-neutral and only increases heart disease risk very slightly:
- Keep Inflammation At Bay ← short version is milk is bad, fermented milk products are fine in moderation
- Is Dairy Scary? ← short version is that milk is neither good nor terrible; fermented dairy products however are health-positive in numerous ways when consumed in moderation
You may be wondering…
…how this goes for the safety of dairy products when it comes to the bird flu currently affecting dairy cows, so:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
3 drugs that went from legal, to illegal, then back again
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cannabis, cocaine and heroin have interesting life stories and long rap sheets. We might know them today as illicit drugs, but each was once legal.
Then things changed. Racism and politics played a part in how we viewed them. We also learned more about their impact on health. Over time, they were declared illegal.
But decades later, these drugs and their derivatives are being used legally, for medical purposes.
Here’s how we ended up outlawing cannabis, cocaine and heroin, and what happened next.
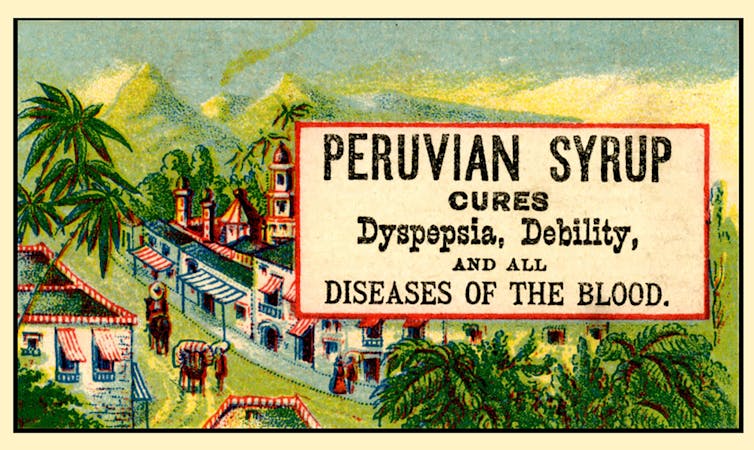
Peruvian Syrup, containing cocaine, was used to ‘cure’ a range of diseases. Smithsonian Museum of American History/Flickr Cannabis, religion and racism
Cannabis plants originated in central Asia, spread to North Africa, and then to the Americas. People grew cannabis for its hemp fibre, used to make ropes and sacks. But it also had other properties. Like many other ancient medical discoveries, it all started with religion.
Cannabis is mentioned in the Hindu texts known as the Vedas (1700-1100 BCE) as a sacred, feel-good plant. Cannabis or bhang is still used ritually in India today during festivals such as Shivratri and Holi.
From the late 1700s, the British in India started taxing cannabis products. They also noticed a high rate of “Indian hemp insanity” – including what we’d now recognise as psychosis – in the colony. By the late 1800s, a British government investigation found only heavy cannabis use seemed to affect people’s mental health.
This drug bottle from the United States contains cannabis tincture. Wikimedia In the 1880s, cannabis was used therapeutically in the United States to treat tetanus, migraine and “insane delirium”. But not everyone agreed on (or even knew) the best dose. Local producers simply mixed up what they had into a tincture – soaking cannabis leaves and buds in alcohol to extract essential oils – and hoped for the best.
So how did cannabis go from a slightly useless legal drug to a social menace?
Some of it was from genuine health concerns about what was added to people’s food, drink and medicine.
In 1908 in Australia, New South Wales listed cannabis as an ingredient that could “adulterate” food and drink (along with opium, cocaine and chloroform). To sell the product legally, you had to tell the customers it contained cannabis.
Some of it was international politics. Moves to control cannabis use began in 1912 with the world’s first treaty against drug trafficking. The US and Italy both wanted cannabis included, but this didn’t happen until until 1925.
Some of it was racism. The word marihuana is Spanish for cannabis (later Anglicised to marijuana) and the drug became associated with poor migrants. In 1915, El Paso, Texas, on the Mexican border, was the first US municipality to ban the non-medical cannabis trade.
By the late 1930s, cannabis was firmly entrenched as a public menace and drug laws had been introduced across much of the US, Europe and (less quickly) Australia to prohibit its use. Cannabis was now a “poison” regulated alongside cocaine and opiates.
The 1936 movie Reefer Madness fuelled cannabis paranoia. Motion Picture Ventures/Wikimedia Commons The 1936 movie Reefer Madness was a high point of cannabis paranoia. Cannabis smoking was also part of other “suspect” new subcultures such as Black jazz, the 1950s Beatnik movement and US service personnel returning from Vietnam.
Today recreational cannabis use is associated with physical and mental harm. In the short term, it impairs your functioning, including your ability to learn, drive and pay attention. In the long term, harms include increasing the risk of psychosis.
But what about cannabis as a medicine? Since the 1980s there has been a change in mood towards experimenting with cannabis as a therapeutic drug. Medicinal cannabis products are those that contain cannabidiol (CBD) or tetrahydrocannabinol (THC). Today in Australia and some other countries, these can be prescribed by certain doctors to treat conditions when other medicines do not work.
Medicinal cannabis has been touted as a treatment for some chronic conditions such as cancer pain and multiple sclerosis. But it’s not clear yet whether it’s effective for the range of chronic diseases it’s prescribed for. However, it does seem to improve the quality of life for people with some serious or terminal illnesses who are using other prescription drugs.
Cocaine, tonics and addiction
Several different species of the coca plant grow across Bolivia, Peru and Colombia. For centuries, local people chewed coca leaves or made them into a mildly stimulant tea. Coca and ayahuasca (a plant-based psychedelic) were also possibly used to sedate people before Inca human sacrifice.
In 1860, German scientist Albert Niemann (1834-1861) isolated the alkaloid we now call “cocaine” from coca leaves. Niemann noticed that applying it to the tongue made it feel numb.
But because effective anaesthetics such as ether and nitrous oxide had already been discovered, cocaine was mostly used instead in tonics and patent medicines.
Hall’s Coca Wine was made from the leaves of the coca plant. Stephen Smith & Co/Wellcome Collection, CC BY Perhaps the most famous example was Coca-Cola, which contained cocaine when it was launched in 1886. But cocaine was used earlier, in 1860s Italy, in a drink called Vin Mariani – Pope Leo XIII was a fan.
With cocaine-based products easily available, it quickly became a drug of addiction.
Cocaine remained popular in the entertainment industry. Fictional detective Sherlock Holmes injected it, American actor Tallulah Bankhead swore by it, and novelist Agatha Christie used cocaine to kill off some of her characters.
In 1914, cocaine possession was made illegal in the US. After the hippy era of the 1960s and 1970s, cocaine became the “it” drug of the yuppie 1980s. “Crack” cocaine also destroyed mostly Black American urban communities.
Cocaine use is now associated with physical and mental harms. In the short and long term, it can cause problems with your heart and blood pressure and cause organ damage. At its worst, it can kill you. Right now, illegal cocaine production and use is also surging across the globe.
But cocaine was always legal for medical and surgical use, most commonly in the form of cocaine hydrochloride. As well as acting as a painkiller, it’s a vasoconstrictor – it tightens blood vessels and reduces bleeding. So it’s still used in some types of surgery.
Heroin, coughing and overdoses
Opium has been used for pain relief ever since people worked out how to harvest the sap of the opium poppy. By the 19th century, addictive and potentially lethal opium-based products such as laudanum were widely available across the United Kingdom, Europe and the US. Opium addiction was also a real problem.
Because of this, scientists were looking for safe and effective alternatives for pain relief and to help people cure their addictions.
In 1874, English chemist Charles Romley Alder Wright (1844-1894) created diacetylmorphine (also known as diamorphine). Drug firm Bayer thought it might be useful in cough medicines, gave it the brand name Heroin and put it on the market in 1898. It made chest infections worse.
Allenburys Throat Pastilles contained heroin and cocaine. Seth Anderson/Flickr, CC BY-NC Although diamorphine was created with good intentions, this opiate was highly addictive. Shortly after it came on the market, it became clear that it was every bit as addictive as other opiates. This coincided with international moves to shut down the trade in non-medical opiates due to their devastating effect on China and other Asian countries.
Like cannabis, heroin quickly developed radical chic. The mafia trafficked into the US and it became popular in the Harlem jazz scene, beatniks embraced it and US servicemen came back from Vietnam addicted to it. Heroin also helped kill US singers Janis Joplin and Jim Morrison.
Today, we know heroin use and addiction contributes to a range of physical and mental health problems, as well as death from overdose.
However, heroin-related harm is now being outpaced by powerful synthetic opioids such as oxycodone, fentanyl, and the nitazene group of drugs. In Australia, there were more deaths and hospital admissions from prescription opiate overdoses than from heroin overdoses.
In a nutshell
Not all medicines have a squeaky-clean history. And not all illicit drugs have always been illegal.
Drugs’ legal status and how they’re used are shaped by factors such as politics, racism and social norms of the day, as well as their impact on health.
Philippa Martyr, Lecturer, Pharmacology, Women’s Health, School of Biomedical Sciences, The University of Western Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The World’s Shortest Weight Loss Course
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The third part of this is what most people are missing:
As easy as 1-2-3?
A lot of things that work very quickly are either not sustainable, or are optical illusions (e.g. loss of water weight) or both.
That doesn’t mean you can or should wait forever for something to magically work, though. Instead, you want something that will offer you consistent measurable progress. Here’s a step-by-step guide to one such approach:
First, the foundation:
• Eat in a small deficit: consume about 15% fewer calories than maintenance, with 18% from protein—any eating style that achieves this works.
• Move more: increase daily steps by 1,000 per month until reaching 6,000–10,000 a day; everyday movement burns more than workouts alone.
• Improve psychology: consistency matters more than fluctuations on the scale. Common blockers include emotional eating, unresolved beliefs about thinness, and lack of deeper motivation beyond appearance.Next, the optimization:
• Improve food quality: aim for 80% whole foods and 20% “anything goes”, reducing junk food gradually.
• Enjoy movement: pick fun, low-impact, medium-intensity activities (like hiking or dancing) to protect joints and build long-term habits.
• Prioritize sleep: add even just 15 minutes at a time, levelling up to another 15 minutes each month, until you reach 8–9 hours per night—vital for metabolic health, brain health, and health on the whole*.Finally, the continuation:
• Be prepared: expect progress to stall every few months; this is biological, not failure. These plateaus are inevitable (but not insurmountable, as you’ll see).
• Overcome plateaus: by adjusting one factor at a time—calories, carbs, protein, sensitivities, exercise type, or temporary maintenance eating.*Yes, even at your age, whatever age that may be. The idea that “older people need less sleep” is a myth, based on the observation of “older people get less sleep”.
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
How To Lose Weight (Healthily!) ← our own main feature on this, which is very compatible with the above method, while having more tips and some very useful resources
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: