Mango vs Pear – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing mango to pear, we picked the mango.
Why?
In terms of macros, pear starts out strong with 2x the fiber for similar carbs and near-equally minimal protein, winning in this category.
In the category of vitamins, however, mango has a lot more of vitamins A, B1, B2, B3, B5, B6, B7, B9, C, and E, while pears are not higher in any vitamin (although they are equal in vitamin K), meaning a 10:0 win for mango here.
Looking at minerals, mango has more calcium, copper, magnesium, manganese, phosphorus, potassium, and selenium, while pears have more iron and zinc, yielding a 7:2 win for mango this time.
Adding up the sections makes for an overall win for mango, but by all means enjoy either or both, as diversity is good!
Want to learn more?
You might like:
What’s Your Plant Diversity Score?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

A ketamine nasal spray will be subsidised for treatment-resistant depression. Here’s what you need to know about Spravato

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
An antidepressant containing a form of the drug ketamine has been added to the Pharmaceutical Benefits Scheme (PBS), making it much cheaper for the estimated 30,000 Australians with treatment-resistant depression. This is when a patient has tried multiple forms of treatment for major depression – usually at least two antidepressant medications – without any improvement.
From May 1, a dose of Spravato (also known as esketamine hydrochloride) will cost $A31.60 and $7.70 for concession card holders.
However, unlike oral antidepressants, Spravato can’t be taken at home. Here’s how it works, and who it’s expected to help.

WPixz/Shutterstock What is Spravato?
The chemical ketamine is used as an anaesthetic. In this formulation it combines both the right-handed (designated “R”) and left-handed (called “S”) forms of the molecule.
This means they are mirror images of each other, similar to how your left hand is a mirror image of your right hand. The left- and right-hand forms can have different effects in the body.
Spravato contains only the left-handed version, giving the drug its generic name esketamine.
Spravato works by increasing the levels of glutamate in the brain. Glutamate is a key chemical messenger molecule that excites brain nerve cells, lifting and improving mood. It also plays a role in learning and forming memories.
How is it taken?
Spravato cannot be taken at home.
A patient can self-administer, but it must be done at a registered treatment facility, such as a hospital, under the supervision of medical staff so they can look out for blood pressure changes and monitor potential side effects.
The drug is provided as a single-use nasal spray. This application means it’s absorbed directly through the nasal lining into the brain, so it starts to work within minutes.
Spravato must also be taken alongside an oral antidepressant. This will be a new one the patient hasn’t tried before. In clinical trials, it was usually an SNRI or SSRI medication.
When a patient first starts on Spravato, they are given the spray twice a week in the first month. It is then administered once a week for the second month, and then weekly or fortnightly after that.
Once there are signs the medicine is working, treatment is continued for at least six months.
You can use the spray yourself but it must be under medical supervision in a registered facility. Scarc/Shutterstock How effective is it?
Spravato was approved for sale in Australia based on clinical trial data from more than 1,600 patients who were administered the drug for a period of four weeks. Each was given either Spravato, or a nasal placebo, and an oral antidepressant.
Patients were given a starting dose of either 28 or 56mg, which could be then increased up to 84mg by their doctor.
By the end of the four weeks, a greater percentage of patients who were given Spravato were found to have had a meaningful response to the treatment when compared with patients who received the placebo. Patients who were taking Spravato were also found to relapse at a lower rate. For those who did relapse, it took the Spravato patients longer to relapse when compared with patients who took the placebo.
It is expected Spravato will benefit a wide range of patients. The clinical trials demonstrated effectiveness for men and women, people aged 18 to 64, and those from a range of different ethnic backgrounds.
Potential side effects
As with any medicine, Spravato may cause side effects, some of which can be serious. The most common include:
- dissociation (feeling disconnected from yourself or what is around you)
- dizziness
- nausea and vomiting
- drowsiness
- headache
- change in taste
- vertigo.
Because Spravato can potentially increase blood pressure, medical staff will monitor a patient before and after it is administered.
Usually, blood pressure spikes around 40 minutes after taking the drug, so a reading is taken around this time. After taking Spravato, if their blood pressure has stayed low, or it’s dropping, the patient is given the all-clear to go home.
Due to the potential for this and other serious side effects, Spravato carries a black triangle warning. This means medical staff are encouraged to report any problem or side effect to the Therapeutic Goods Administration. A black triangle warning is generally used for new medicines or medicines that are being used in a new way.
Who will be eligible?
To be eligible for a prescription, a patient will need to have been diagnosed with treatment-resistant depression. In practice, this means they will have unsuccessfully tried at least two other antidepressant drugs first.
Australia’s Therapeutic Goods Administration approved Spravato for use in Australia in 2021, meaning it was available but not subsidised. Since then, the sponsoring company, Janssen-Cilag (an Australian subsidiary of the multinational Johnson & Johnson), applied to have it added to the PBS four times.
In December 2024, the Pharmaceutical Benefits Advisory Committee recommended a PBS listing.
The new PBS listing, capping the price of a single treatment at $31.60, is a significant price drop. In 2023, single doses of branded Spravato were reported to cost anywhere between $500 and $900.
However, patients may still have to pay hundreds of dollars for appointments at private clinics where Spravato can be administered. Public places are available but limited.
Spravato may be suitable for you if you’ve tried different antidepressants without success. If it is suitable for you, then your doctor can discuss the next steps.
If this article has raised issues for you, or if you’re concerned about someone you know, call Lifeline on 13 11 14.
Nial Wheate, Professor, School of Natural Sciences, Macquarie University and Shoohb Alassadi, Associate Lecturer and Registered Pharmacist, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Beet The Odds – by Dr. Nathan Bryan & Carolyn Pierini
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
By the same first-listed author as the book we recently reviewed about nitric oxide, this time he’s teamed up with a clinician specialized in the biochemistry of human nutrigenomics, this time to extol the virtues of beets—and we do say “beets”, since while the root (thus, beetroot) is the most-discussed part of the plant, the leaves and stalks have benefits too.
We learn a lot about its effects on the heart and blood, and its antioxidant properties, as well as the unique properties associated with betalain and especially betanin. Lastly, unsurprisingly from this author, we also hear about beets’ benefits in the category of improving nitric oxide levels (as the plant is a good source of nitrates, which the body can use to make that).
The style is is quite bold and colorful; there’s little hard science here, and we are not treated to sources for claims as we go along. It’s also worth noting that this book is a scant 56 pages, so, a lot more than we can fit in an article here (such as our own Beetroot For More Than Just Your Blood Pressure), but still a little lighter than we’re used to.
There is an ad for Dr. Bryan’s beetroot powder supplements at the end.
Bottom line: beets are great (unless you are avoiding oxalates, in which case, maybe skip them as they’re quite high in those, but for most people without kidney problems this is a non-issue), and this short, light, enthusiastic book does a fair job of explaining how they’re great.
Share This Post
-

Who will look after us in our final years? A pay rise alone won’t solve aged-care workforce shortages
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Aged-care workers will receive a significant pay increase after the Fair Work Commission ruled they deserved substantial wage rises of up to 28%. The federal government has committed to the increases, but is yet to announce when they will start.
But while wage rises for aged-care workers are welcome, this measure alone will not fix all workforce problems in the sector. The number of people over 80 is expected to triple over the next 40 years, driving an increase in the number of aged care workers needed.
How did we get here?
The Royal Commission into Aged Care Quality and Safety, which delivered its final report in March 2021, identified a litany of tragic failures in the regulation and delivery of aged care.
The former Liberal government was dragged reluctantly to accept that a total revamp of the aged-care system was needed. But its weak response left the heavy lifting to the incoming Labor government.
The current government’s response started well, with a significant injection of funding and a promising regulatory response. But it too has failed to pursue a visionary response to the problems identified by the Royal Commission.
Action was needed on four fronts:
- ensuring enough staff to provide care
- building a functioning regulatory system to encourage good care and weed out bad providers
- designing and introducing a fair payment system to distribute funds to providers and
- implementing a financing system to pay for it all and achieve intergenerational equity.
A government taskforce which proposed a timid response to the fourth challenge – an equitable financing system – was released at the start of last week.
Consultation closed on a very poorly designed new regulatory regime the week before.
But the big news came at end of the week when the Fair Work Commission handed down a further determination on what aged-care workers should be paid, confirming and going beyond a previous interim determination.
What did the Fair Work Commission find?
Essentially, the commission determined that work in industries with a high proportion of women workers has been traditionally undervalued in wage-setting. This had consequences for both care workers in the aged-care industry (nurses and Certificate III-qualified personal-care workers) and indirect care workers (cleaners, food services assistants).
Aged-care staff will now get significant pay increases – 18–28% increase for personal care workers employed under the Aged Care Award, inclusive of the increase awarded in the interim decision.
The commission determined aged care work was undervalued.
Shutterstock/Toa55Indirect care workers were awarded a general increase of 3%. Laundry hands, cleaners and food services assistants will receive a further 3.96% on the grounds they “interact with residents significantly more regularly than other indirect care employees”.
The final increases for registered and enrolled nurses will be determined in the next few months.
How has the sector responded?
There has been no push-back from employer groups or conservative politicians. This suggests the uplift is accepted as fair by all concerned.
The interim increases of up to 15% probably facilitated this acceptance, with the recognition of the community that care workers should be paid more than fast food workers.
There was no criticism from aged-care providers either. This is probably because they are facing difficulty in recruiting staff at current wage rates. And because government payments to providers reflect the actual cost of aged care, increased payments will automatically flow to providers.
When the increases will flow has yet to be determined. The government is due to give its recommendations for staging implementation by mid-April.
Is the workforce problem fixed?
An increase in wages is necessary, but alone is not sufficient to solve workforce shortages.
The health- and social-care workforce is predicted to grow faster than any other sector over the next decade. The “care economy” will grow from around 8% to around 15% of GDP over the next 40 years.
This means a greater proportion of school-leavers will need to be attracted to the aged-care sector. Aged care will also need to attract and retrain workers displaced from industries in decline and attract suitably skilled migrants and refugees with appropriate language skills.
Aged care will need to attract workers from other sectors.
nastya_ph/ShutterstockThe caps on university and college enrolments imposed by the previous government, coupled with weak student demand for places in key professions (such as nursing), has meant workforce shortages will continue for a few more years, despite the allure of increased wages.
A significant increase in intakes into university and vocational education college courses preparing students for health and social care is still required. Better pay will help to increase student demand, but funding to expand place numbers will ensure there are enough qualified staff for the aged-care system of the future.

Stephen Duckett, Honorary Enterprise Professor, School of Population and Global Health, and Department of General Practice and Primary Care, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post






Related Posts
-
Beetroot vs Zucchini – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing beetroot to zucchini, we picked the beetroot.
Why?
Both have their strong virtues! But…
In terms of macros, beetroot has more fiber, carbs, and protein, winning in this round.
In the category of vitamins, beetroot has more vitamin B9, while zucchini has more of vitamins A, B1, B2, B3, B5, B6, C, E, K, and choline, winning easily.
Looking at minerals; this imbalance gets flipped: beetroot has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while zucchini is not higher in any minerals; a total win here for beetroot.
In other considerations, beetroot has more polyphenols, especially quercetin, and beetroot’s other phytochemical benefits are so numerous we’ll not list them here, and just recommend checking out the link below!
Adding up the sections makes for a clear overall win for beetroot, but zucchini were much stronger in the vitamin category, so by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
Beetroot For More Than Just Your Blood Pressure ← more beetroot benefits
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Canned Tuna vs Canned Sardines – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing canned tuna to canned sardines, we picked the sardines.
Why?
This comparison is unfair, but practical—because both are sold next to each other in the supermarket and often used for similar things.
It’s unfair because in a can of tuna, there is tuna meat, whereas in a can of sardines, there is sardine meat, skin, and bones.
Consequently, sardines outperform tuna in almost everything, because a lot of nutrients are in the skin and bones.
To be completely unambiguous:
Sardines have more vitamins and minerals by far (special shout-out to calcium, of which sardines contain 6000% more), and more choline (which is sometimes reckoned as a vitamin, sometimes not).
Tuna does have marginally more protein, and less fat. If you are trying to limit your cholesterol intake, then that could be an argument for choosing tuna over sardines.
All in all: the sardines are more nutrient dense by far, are good sources of vitamins and minerals that tuna contains less of (and in many cases only trace amounts of), and for most people this will more than offset the difference in cholesterol, especially if having not more than one can per day.
About that skin and bones…
That’s where the real benefit for your joints lies, by the way!
See: We Are Such Stuff As Fish Are Made Of
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Cannabis Myths vs Reality
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cannabis Myths vs Reality

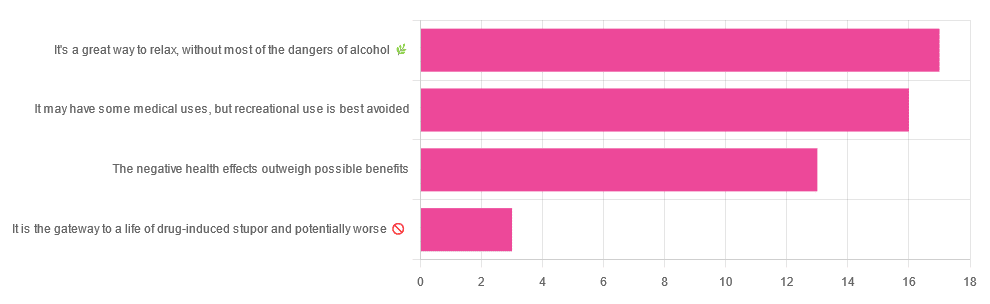
We asked you for your (health-related) opinion on cannabis use—specifically, the kind with psychoactive THC, not just CBD. We got the above-pictured, below-described, spread of responses:
- A little over a third of you voted for “It’s a great way to relax, without most of the dangers of alcohol”.
- A little under a third of you voted for “It may have some medical uses, but recreational use is best avoided”.
- About a quarter of you voted for “The negative health effects outweigh the possible benefits”
- Three of you voted for “It is the gateway to a life of drug-induced stupor and potentially worse”
So, what does the science say?
A quick legal note first: we’re a health science publication, and are writing from that perspective. We do not know your location, much less your local laws and regulations, and so cannot comment on such. Please check your own local laws and regulations in that regard.
Cannabis use can cause serious health problems: True or False?
True. Whether the risks outweigh the benefits is a personal and subjective matter (for example, a person using it to mitigate the pain of late stage cancer is probably unconcerned with many other potential risks), but what’s objectively true is that it can cause serious health problems.
One subscriber who voted for “The negative health effects outweigh the possible benefits” wrote:
❝At a bare minimum, you are ingesting SMOKE into your lungs!! Everyone SEEMS TO BE against smoking cigarettes, but cannabis smoking is OK?? Lung cancer comes in many forms.❞
Of course, that is assuming smoking cannabis, and not consuming it as an edible. But, what does the science say on smoking it, and lung cancer?
There’s a lot less research about this when it comes to cannabis, compared to tobacco. But, there is some:
❝Results from our pooled analyses provide little evidence for an increased risk of lung cancer among habitual or long-term cannabis smokers, although the possibility of potential adverse effect for heavy consumption cannot be excluded.❞
Read: Cannabis smoking and lung cancer risk: Pooled analysis in the International Lung Cancer Consortium
Another study agreed there appears to be no association with lung cancer, but that there are other lung diseases to consider, such as bronchitis and COPD:
❝Smoking cannabis is associated with symptoms of chronic bronchitis, and there may be a modest association with the development of chronic obstructive pulmonary disease. Current evidence does not suggest an association with lung cancer.❞
Read: Cannabis Use, Lung Cancer, and Related Issues
Cannabis edibles are much safer than smoking cannabis: True or False?
Broadly True, with an important caveat.
One subscriber who selected “It may have some medical uses, but recreational use is best avoided”, wrote:
❝I’ve been taking cannabis gummies for fibromyalgia. I don’t know if they’re helping but they’re not doing any harm. You cannot overdose you don’t become addicted.❞
Firstly, of course consuming edibles (rather than inhaling cannabis) eliminates the smoke-related risk factors we discussed above. However, other risks remain, including the much greater ease of accidentally overdosing.
❝Visits attributable to inhaled cannabis are more frequent than those attributable to edible cannabis, although the latter is associated with more acute psychiatric visits and more ED visits than expected.❞
Note: that “more frequent” for inhaled cannabis, is because more people inhale it than eat it. If we adjust the numbers to control for how much less often people eat it, suddenly we see that the numbers of hospital admissions are disproportionately high for edibles, compared to inhaled cannabis.
Or, as the study author put it:
❝There are more adverse drug events associated on a milligram per milligram basis of THC when it comes in form of edibles versus an inhaled cannabis. If 1,000 people smoked pot and 1,000 people at the same dose in an edible, then more people would have more adverse drug events from edible cannabis.❞
See the numbers: Acute Illness Associated With Cannabis Use, by Route of Exposure
Why does this happen?
- It’s often because edibles take longer to take effect, so someone thinks “this isn’t very strong” and has more.
- It’s also sometimes because someone errantly eats someone else’s edibles, not realising what they are.
- It’s sometimes a combination of the above problems: a person who is now high, may simply forget and/or make a bad decision when it comes to eating more.
On the other hand, that doesn’t mean inhaling it is necessarily safer. As well as the pulmonary issues we discussed previously, inhaling cannabis has a higher risk of cannabinoid hyperemesis syndrome (and the resultant cyclic vomiting that’s difficult to treat).
You can read about this fascinating condition that’s sometimes informally called “scromiting”, a portmanteau of screaming and vomiting:
Cannabinoid Hyperemesis Syndrome
You can’t get addicted to cannabis: True or False?
False. However, it is fair to say that the likelihood of developing a substance abuse disorder is lower than for alcohol, and much lower than for nicotine.
See: Prevalence of Marijuana Use Disorders in the United States Between 2001–2002 and 2012–2013
If you prefer just the stats without the science, here’s the CDC’s rendering of that:
Addiction (Marijuana or Cannabis Use Disorder)
However, there is an interesting complicating factor, which is age. One is 4–7 times more likely to develop a substance abuse disorder, if one starts use as an adolescent, rather than later as an adult:
Cannabis is the gateway to use of more dangerous drugs: True or False?
False, generally speaking. Of course, for any population there will be some outliers, but there appears to be no meaningful causal relation between cannabis use and other substance use:
Interestingly, the strongest association (where any existed at all) was between cannabis use and opioid use. However, rather than this being a matter of cannabis use being a gateway to opioid use, it seems more likely that this is a matter of people looking to both for the same purpose: pain relief.
As a result, growing accessibility of cannabis may actually reduce opioid problems:
- Cannabis as a Gateway Drug for Opioid Use Disorder
- Association between medical cannabis laws and opioid overdose mortality has reversed over time
Some final words…
Cannabis is a complex drug with complex mechanisms and complex health considerations, and research is mostly quite young, due to its historic illegality seriously cramping science by reducing sample sizes to negligible. Simply put, there’s a lot we still don’t know.
Also, we covered some important topics today, but there were others we didn’t have time to cover, such as the other potential psychological benefits—and risks. Likely we’ll revisit those another day.
Lastly, while we’ve covered a bunch of risks today, those of you who said it has fewer and lesser risks than alcohol are quite right—the only reason we couldn’t focus on that more, is because to talk about all the risks of alcohol would make this feature many times longer!
Meanwhile, whether you partake or not, stay safe and stay well.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: