Loving Someone Who Has Dementia – by Dr. Pauline Boss
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We previously reviewed Dr. Boss’s excellent book “Loss, Trauma, and Resilience: Therapeutic Work With Ambiguous Loss”, which partially overlaps in ideas with this one. In that case, it was about grief when a loved one is “gone, but are they really?”, which can include missing persons, people killed in ways that weren’t 100% confirmed (e.g. no body to bury), and in contrast, people who are present in body but not entirely present mentally: perhaps in a coma, for example. It also includes people are for other reasons not entirely present in the way they used to be, which includes dementia. And that latter case is what this book focuses on.
In the case of dementia, we cannot, of course, simply focus on ourselves. Well, not if we care about the person with dementia, anyway. Much like with the other kinds of ambiguous loss, we cannot fully come to terms with things while on the cusp of presence and absence, and we cannot, as such, “give up” on our loved one.
What then, of hope? The author makes the case for—in absence of any kind of closure—making our peace with the situation as it is, making our peace with the uncertainty of things. And that means not only “at any moment could come a more clearly complete loss”, but also on the flipside at least a faint candle of hope, that we should not grasp with both hands (that is not how to treat a candle, literally or metaphorically), but rather, hold gently, and enjoy its gentle light.
Dr. Boss also covers more practical considerations; family rituals, celebrations, gatherings, and the idea of “the good-enough relationship”. Particularly helpfully, she gives her “seven guidelines for the journey”, which even if one decides against adopting them all, are definitely all good things to at least have considered.
The style is much more tailored to the lay reader than the other book of hers that we reviewed, which was intended more for clinicians, but useful also for those of us who have been hit by such kinds of grief. In this case, however, her intention is first and foremost for the family of a person who has dementia—there are still footnotes throughout though, for those who still want to read scientific papers that support the various ideas discussed in the book.
Bottom line: if a loved one has dementia or that seems a likely possibility for you, this book can help a lot!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Makkō-Hō – by Haruka Nagai

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve all heard the claims, “Fluent in 3 Months!”, “Russian in Two Weeks!”, “Overnight Mandarin Chinese”, “15-Minute Arabic!”, “Instant Italian!”.
We see the same in the world of health and fitness too. So how does this one’s claim of “five minutes’ physical fitness” hold up?
Well, it is 5 minutes per day. And indeed, the author writes:
❝The total time [to do these exercises], then, is only one minute and thirty seconds. This series I call one round. When it has been completed, execute another complete round. You should find the exercises easier to do the second time. Executed this way, the exercsies will prove very effective, though they take only three minutes in all. After you have leaned back into the final position, you must remain in that posture for one minute. That brings the total time to four minutes. Even when [some small additions] are added, it takes only five minutes at most.❞
The exercises themselves are from makkō-hō, which is a kind of Japanese dynamic yoga. They involve repetitions of (mostly) moving stretches with good form, and are excellent for mobility and general health, keeping us supple and robust as we get older.
The text descriptions are clear, as are the diagrams and photos. The language is a little dated, as this book was written in the 1970s, but the techniques themselves are timeless.
Bottom line: consider it a 5-minute anti-aging regimen. And, as Nagai says, “the person who cannot find 5 minutes out of 24 hours, was never truly interested in their health”.
Click here to check out Makkō-Hō and schedule your five minutes!
Share This Post
-

I have a stuffy nose, how can I tell if it’s hay fever, COVID or something else?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hay fever (also called allergic rhinitis) affects 24% of Australians. Symptoms include sneezing, a runny nose (which may feel blocked or stuffy) and itchy eyes. People can also experience an itchy nose, throat or ears.
But COVID is still spreading, and other viruses can cause cold-like symptoms. So how do you know which one you’ve got?

Lysenko Andrii/Shutterstock Remind me, how does hay fever cause symptoms?
Hay fever happens when a person has become “sensitised” to an allergen trigger. This means a person’s body is always primed to react to this trigger.
Triggers can include allergens in the air (such as pollen from trees, grasses and flowers), mould spores, animals or house dust mites which mostly live in people’s mattresses and bedding, and feed on shed skin.
When the body is exposed to the trigger, it produces IgE (immunoglobulin E) antibodies. These cause the release of many of the body’s own chemicals, including histamine, which result in hay fever symptoms.
People who have asthma may find their asthma symptoms (cough, wheeze, tight chest or trouble breathing) worsen when exposed to airborne allergens. Spring and sometimes into summer can be the worst time for people with grass, tree or flower allergies.
However, animal and house dust mite symptoms usually happen year-round.
Ryegrass pollen is a common culprit. bangku ceria/Shutterstock What else might be causing my symptoms?
Hay fever does not cause a fever, sore throat, muscle aches and pains, weakness, loss of taste or smell, nor does it cause you to cough up mucus.
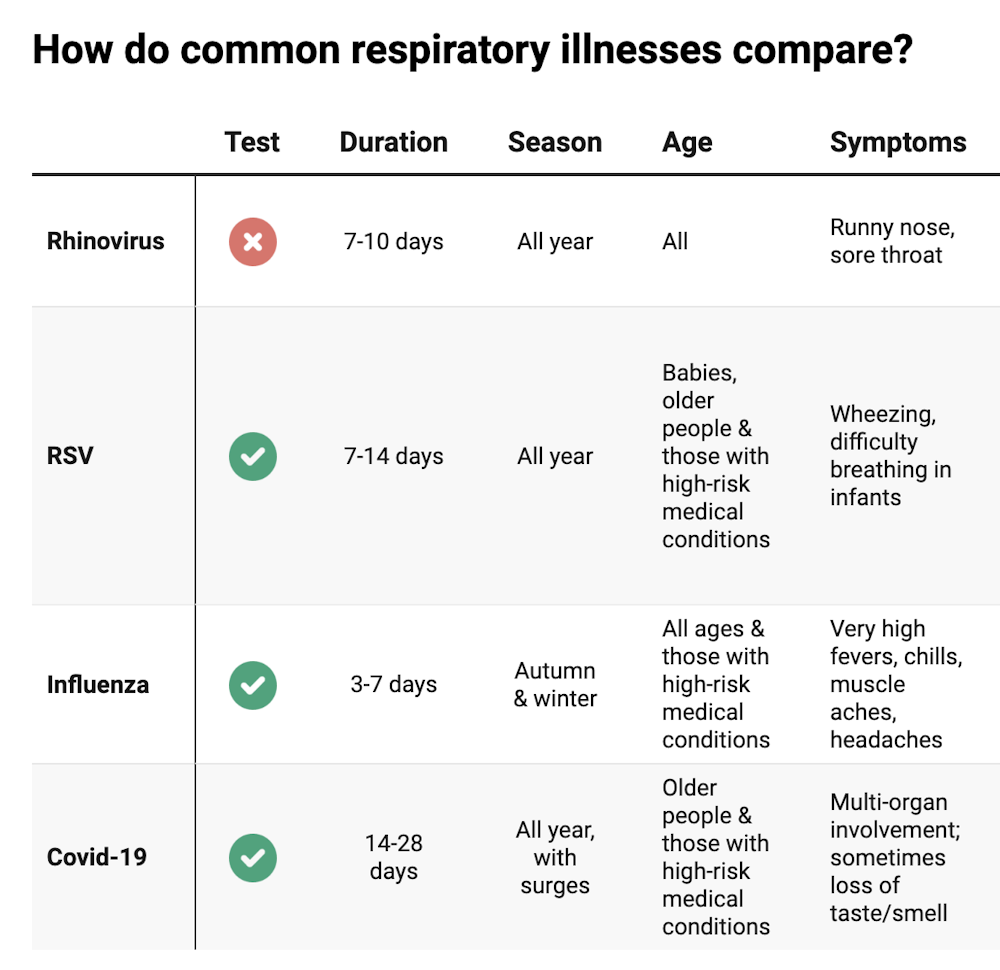
These symptoms are likely to be caused by a virus, such as COVID, influenza, respiratory syncytial virus (RSV) or a “cold” (often caused by rhinoviruses). These conditions can occur all year round, with some overlap of symptoms:
Natasha Yates/The Conversation COVID still surrounds us. RSV and influenza rates appear higher than before the COVID pandemic, but it may be due to more testing.
So if you have a fever, sore throat, muscle aches/pains, weakness, fatigue, or are coughing up mucus, stay home and avoid mixing with others to limit transmission.
People with COVID symptoms can take a rapid antigen test (RAT), ideally when symptoms start, then isolate until symptoms disappear. One negative RAT alone can’t rule out COVID if symptoms are still present, so test again 24–48 hours after your initial test if symptoms persist.
You can now test yourself for COVID, RSV and influenza in a combined RAT. But again, a negative test doesn’t rule out the virus. If your symptoms continue, test again 24–48 hours after the previous test.
If it’s hay fever, how do I treat it?
Treatment involves blocking the body’s histamine release, by taking antihistamine medication which helps reduce the symptoms.
Doctors, nurse practitioners and pharmacists can develop a hay fever care plan. This may include using a nasal spray containing a topical corticosteroid to help reduce the swelling inside the nose, which causes stuffiness or blockage.
Nasal sprays need to delivered using correct technique and used over several weeks to work properly. Often these sprays can also help lessen the itchy eyes of hay fever.
Drying bed linen and pyjamas inside during spring can lessen symptoms, as can putting a smear of Vaseline in the nostrils when going outside. Pollen sticks to the Vaseline, and gently blowing your nose later removes it.
People with asthma should also have an asthma plan, created by their doctor or nurse practitioner, explaining how to adjust their asthma reliever and preventer medications in hay fever seasons or on allergen exposure.
People with asthma also need to be alert for thunderstorms, where pollens can burst into tinier particles, be inhaled deeper in the lungs and cause a severe asthma attack, and even death.
What if it’s COVID, RSV or the flu?
Australians aged 70 and over and others with underlying health conditions who test positive for COVID are eligible for antivirals to reduce their chance of severe illness.
Most other people with COVID, RSV and influenza will recover at home with rest, fluids and paracetamol to relieve symptoms. However some groups are at greater risk of serious illness and may require additional treatment or hospitalisation.
For RSV, this includes premature infants, babies 12 months and younger, children under two who have other medical conditions, adults over 75, people with heart and lung conditions, or health conditions that lessens the immune system response.
For influenza, people at higher risk of severe illness are pregnant women, Aboriginal people, people under five or over 65 years, or people with long-term medical conditions, such as kidney, heart, lung or liver disease, diabetes and decreased immunity.
If you’re concerned about severe symptoms of COVID, RSV or influenza, consult your doctor or call 000 in an emergency.
If your symptoms are mild but persist, and you’re not sure what’s causing them, book an appointment with your doctor or nurse practitioner. Although hay fever season is here, we need to avoid spreading other serious infectious.
For more information, you can call the healthdirect helpline on 1800 022 222 (known as NURSE-ON-CALL in Victoria); use the online Symptom Checker; or visit healthdirect.gov.au or the Australian Society of Clinical Immunology and Allergy.
Deryn Thompson, Eczema and Allergy Nurse; Lecturer, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

A Therapeutic Journey – by Alain de Botton
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve often featured The School of Life’s videos here on 10almonds, and most of those are written by (and often voiced by) Alain de Botton.
This book lays out the case for mental health being also just health, that no person is perfectly healthy all the time, and sometimes we all need a little help. While he does suggest seeking help from reliable outside sources, he also tells a lot about how we can improve things for ourselves along the way, whether by what we can control in our environment, or just what’s between our ears.
In the category of limitations, the book is written with the assumption that you are in a position to have access to a therapist of your choice, and in a sufficiently safe and stable life situation that there is a limit to how bad things can get.
The style is… Alain de Botton’s usual style. Well-written, clear, decisive, instructive, compassionate, insightful, thought-provoking.
Bottom line: this isn’t a book for absolutely everyone, but if your problems are moderate and your resources are comfortable, then this book has a lot of insights that can make your life more easy-going and joyful, without dropping the seriousness when appropriate.
Click here to check out A Therapeutic Journey, and perhaps begin one of your own!
Share This Post


Related Posts
-

Cold Medicines & Heart Health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cold Medicines & Heart Health
In the wake of many decongestants disappearing from a lot of shelves after a common active ingredient being declared useless*, you may find yourself considering alternative decongestants at this time of year.
*In case you missed it:
It doesn’t seem to be dangerous, by the way, just also not effective:
FDA Panel Says Common OTC Decongestant, Phenylephrine, Is Useless
Good for your nose, bad for your heart?
With products based on phenylephrine out of the running, products based on pseudoephedrine, a competing drug, are enjoying a surge in popularity.
Good news: pseudoephedrine works!
Bad news: pseudoephedrine works because it is a vasoconstrictor, and that vasoconstriction reduces nasal swelling. That same vasoconstriction also raises overall blood pressure, potentially dangerously, depending on an assortment of other conditions you might have.
Further reading: Can decongestants spike your blood pressure? What to know about hypertension and cold medicine
Who’s at risk?
The warning label, unread by many, reads:
❝Do not use this product if you have heart disease, high blood pressure, thyroid disease, diabetes, or difficulty in urination due to enlargement of the prostate gland, unless directed by a doctor❞
Source: Harvard Health | Don’t let decongestants squeeze your heart
What are the other options?
The same source as above recommends antihistamines as an option to be considered, citing:
❝Antihistamines such as […] cetirizine (Zyrtec) and loratadine (Claritin) can help with a stuffy nose and are safe for the heart.❞
But we’d be remiss not to mention drug-free options too, for example:
- Saline rinse with a neti pot or similar
- Use of a humidifier in your house/room
- Steam inhalation, with or without eucalyptus etc
See also: Inhaled Eucalyptus’s Immunomodulatory and Antimicrobial Effects
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Women Rowing North – by Dr. Mary Pipher
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Ageism is rife, as is misogyny. And those can be internalized too, and compounded as they intersect.
Clinical psychologist Dr. Mary Pipher, herself 75, writes for us a guidebook of, as the subtitle goes, “navigating life’s currents and flourishing as we age”.
The book does assume, by the way, that the reader is…
- a woman, and
- getting old (if not already old)
However, the lessons the book imparts are vital for women of any age, and valuable as a matter of insight and perspective for any reader.
Dr. Pipher takes us on a tour of aging as a woman, and what parts of it we can make our own, do things our way, and take what joy we can from it.
Nor is the book given to “toxic positivity” though—it also deals with themes of hardship, frustration, and loss.
When it comes to those elements, the book is… honest, human, and raw. But also, an exhortation to hope, beauty, and a carpe diem attitude.
Bottom line: this book is highly recommendable to anyone of any age; life is precious and can be short. And be we blessed with many long years, this book serves as a guide to making each one of them count.
Click here to check out Women Rowing North—it really is worth it
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Seven-Day Sleep Prescription – by Dr. Aric Prather
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You probably already know about sleep hygiene. So, what does this book have to offer?
Dr. Aric Prather offers seven days’ worth of adjustments, practices to take up, from when you get up in the morning to when you lay your head down at night.
Some you’ll surely be familiar with, like avoiding blue light and social media at night.
Others, you might not be familiar with, like scheduling 15 minutes for worrying in the daytime. The rationale for this one is that when you find yourself inclined to worry at a time that will keep you awake, you’ll know that you can put off such thoughts to your scheduled “worrying time”. That they’ll be addressed then, and that you can thus sleep soundly meanwhile.
Where the book really comes into its own is in such things as discussing how to not just manage sleep debt, but how to actually use it in your favour.
Nor does Dr. Prather shy away from the truths of our world… That the world these days is not built for us to sleep well. That there are so many other priorities; to get our work done, to succeed and achieve, to pay bills, to support our kids and partners. That so many of these things make plenty of sense in the moment, but catch up with us eventually.
Bottom line: what this book aims to give is a genuinely sustainable approach to sleeping—controlling what we can, and working with what we can’t. If you’d like to have a better relationship with sleep, this book is an excellent choice.
Click here to check out the Seven-Day Sleep Prescription, and improve yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: