A Therapeutic Journey – by Alain de Botton
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve often featured The School of Life’s videos here on 10almonds, and most of those are written by (and often voiced by) Alain de Botton.
This book lays out the case for mental health being also just health, that no person is perfectly healthy all the time, and sometimes we all need a little help. While he does suggest seeking help from reliable outside sources, he also tells a lot about how we can improve things for ourselves along the way, whether by what we can control in our environment, or just what’s between our ears.
In the category of limitations, the book is written with the assumption that you are in a position to have access to a therapist of your choice, and in a sufficiently safe and stable life situation that there is a limit to how bad things can get.
The style is… Alain de Botton’s usual style. Well-written, clear, decisive, instructive, compassionate, insightful, thought-provoking.
Bottom line: this isn’t a book for absolutely everyone, but if your problems are moderate and your resources are comfortable, then this book has a lot of insights that can make your life more easy-going and joyful, without dropping the seriousness when appropriate.
Click here to check out A Therapeutic Journey, and perhaps begin one of your own!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What is frozen shoulder? And will I need surgery?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Frozen shoulder can make simple tasks – such as lifting your arm, sleeping on your side, getting out of bed, putting on a bra, driving or playing with your kids – painful and challenging.
This condition usually starts with pain suddenly developing in the shoulder and stiffness. Over time, the pain and stiffness get worse. It can drag on for months or even years.
So, what causes frozen shoulder? And can it be treated?

Mikolette/Getty What is frozen shoulder?
This shoulder condition, also known as “adhesive capsulitis”, affects around 8% of men and 10% of women aged 25–64. But it’s more common over 40, especially for people in their 60s.
We don’t fully understand what causes frozen shoulder.
The tissues around the joint become tight, swollen and stiff. But we don’t know exactly why these changes occur and lead to pain and limited movement.
There are usually three stages:
- freezing – pain gradually gets worse and the shoulder becomes stiff, limiting the range of movement
- frozen – stiffness and pain usually peak, but may begin to ease
- thawing – pain and stiffness slowly improve, and movement begins to return.
While health professionals commonly accept it, this staged description suggests frozen shoulder will follow a predictable pattern and always get better on its own. But research suggests this is not always the case.
For example, the “freezing” stage is usually expected to last at least ten weeks. But some people will start to notice improved movement sooner.
Recovery stages will vary from person to person and can take months to years. Some people may not fully recover, even with treatment.
One 2020 study followed up with 215 patients with frozen shoulder. While over 70% of participants said they were happy with improvements in their symptoms, around 40% still had some movement restriction two years after their symptoms began.
Another study from 2008 found over a third of people they surveyed (41%) had ongoing symptoms two to seven years later, including pain and difficulty sleeping.
Who is most at risk?
Certain groups are more likely to develop frozen shoulder:
- women, especially during menopause
- people with diabetes
- older adults
- those with high cholesterol or thyroid problems.
There is some evidence genetics also plays a role, as a family history increases your risk.
But we need more high-quality research to understand what’s behind these risk factors.
For example, people with diabetes are around five times more likely to develop frozen shoulder than those without diabetes – and also have worse pain. This may be linked to diabetes-related changes in the body, such as reduced blood flow to tissues and chemical changes from high blood sugar. But the exact mechanisms are unclear, and research is yet to determine whether controlling blood sugar better could help prevent or slow frozen shoulder.
Similarly, women are 40% more likely to develop frozen shoulder than men, with one theory suggesting hormone fluctuations during menopause are responsible. But there is no clear evidence yet to support this.
How is frozen shoulder treated?
There is mixed evidence about which treatments are effective, including whether over-the-counter pain medication such as Voltaren helps.
Oral steroids
A review of the evidence suggests oral steroids, such as prednisolone, can provide some short-term pain relief and improve shoulder movement, compared to doing nothing or a placebo. But these benefits don’t seem to last beyond six weeks, and the evidence comes from a few small studies. These require a prescription.
Injections
High-quality evidence shows corticosteroid injections can provide short-term relief, compared to doing nothing.
There is also some limited evidence that corticosteroid injections and platelet rich plasma injections can provide better short-term pain relief, compared with over-the-counter pain relief and physiotherapy. However, the studies are small or poorly designed and the effects are small, so the evidence needs to be interpreted with caution.
Physiotherapy
Moderate-quality evidence suggests physiotherapy can help improve shoulder movement. Benefits of physio are greater when combined with a steroid injection, and followed up by doing the exercises at home. More research is needed to understand how well these treatments work in the long term.
What about surgery?
There are two main procedures for frozen shoulder, both done while the patient is unconscious under anaesthetic.
1. Manipulation under anaesthetic
This is a less invasive procedure where the surgeon stretches the shoulder, without cutting into the joint, to help loosen tight tissue that may be causing stiffness.
2. Arthroscopic capsular release
In this type of keyhole surgery, the surgeon cuts tight tissues inside the shoulder joint to try to free up shoulder movement.
Improvements from these procedures are typically small, and evidence suggests the results are not better than non-surgical treatments. For example, one study showed that after one year, patients who’d had surgery had similar improvements to those who’d had physiotherapy and a steroid injection, but no surgery.
These procedures also have several downsides. It’s more expensive than other treatments, carries additional risks, and typically requires weeks (and up to three months) of rehabilitation.
The bottom line
Being physically active and doing exercises can help if you’re experiencing pain and limited movement. But you don’t have to work this out alone. It’s a good idea to get advice on managing pain and how to stay active.
If you suspect you have frozen shoulder, it’s important to see a doctor or physiotherapist so they can rule out other conditions, such as fracture and arthritis.
A health professional can also discuss management – the potential benefits, harms, costs, and how easy it is to access each treatment option.
Fernando Sousa, Research Fellow in Physiotherapy, Monash University; Joshua Zadro, NHMRC Emerging Leader Research Fellow, Sydney Musculoskeletal Health, University of Sydney, and Peter Malliaras, Professor in Physiotherapy, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Why You’re Probably Not Getting Enough Potassium
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Everybody knows we need potassium; not everybody knows why. In fact, there are a lot of things it does for us; we’ll let Harvard Health sum it up in few words:
❝Potassium is necessary for the normal functioning of all cells. It regulates the heartbeat, ensures proper function of the muscles and nerves, and is vital for synthesizing protein and metabolizing carbohydrates.❞
Read in full: Harvard Health | The Importance Of Potassium
However, we’re going to focus on one aspect of that:
When 0 K Is Not OK
Potassium (chemical symbol: K) helps regulate blood pressure by doing the opposite of what sodium does: high sodium intake increases blood volume and pressure by retaining fluid, while potassium promotes sodium excretion through urine, reducing fluid retention and lowering blood pressure.
Research has shown that increasing potassium intake can reduce systolic blood pressure by an average of 3.49 units, with even greater reductions (up to 7 units) at higher potassium intakes of 3,500–4,700 mg/day:
❝Increased potassium intake reduced systolic blood pressure by 3.49 (95% confidence interval 1.82 to 5.15) mm Hg and diastolic blood pressure by 1.96 (0.86 to 3.06) mm Hg in adults, an effect seen in people with hypertension but not in those without hypertension.
Systolic blood pressure was reduced by 7.16 (1.91 to 12.41) mm Hg when the higher potassium intake was 90-120 mmol/day, without any dose response.
Increased potassium intake had no significant adverse effect on renal function, blood lipids, or catecholamine concentrations in adults.
An inverse statistically significant association was seen between potassium intake and risk of incident stroke (risk ratio 0.76, 0.66 to 0.89).❞
Read in full: Effect of increased potassium intake on cardiovascular risk factors and disease: systematic review and meta-analyses
Note that the blood-pressure-lowering effect not being seen in people without hypertension is a good thing too; if your blood pressure is already healthy, you don’t want it to be lower!
For most people, though, the BP numbers could stand to be lower.
So, should I eat more bananas?
Potassium-rich foods include most fruit*, leafy greens, broccoli, lentils, and beans.
*because of some popular mentions in TV shows, people get hung up on bananas being a good source of potassium. Which they are, but they’re not even in the top 10 of fruits for potassium. Here’s a non-exhaustive list of fruits that have more potassium than bananas, portion for portion:
- Honeydew melon
- Papaya
- Mango
- Prunes
- Figs
- Dates
- Nectarine
- Cantaloupe melon
- Kiwi
- Orange
However, fruit is mostly water weight, and if we take the top-scorer from that list, the honeydew, we see that you’d need to eat 2kg of honeydew melon per day to get your ideal potassium needs met.
So, supplementation?
That’s probably a good idea for most people.
This is especially an issue because a lot of people take a daily “multivitamins and minerals” tablet, and figure it’ll cover whatever their diet misses.
That’s reasonable logic, but those kinds of supplements don’t usually have potassium, for the simple reason that to get even the low-end recommended daily amount (3.4g), then no matter how you slice it, you cannot fit 3.4g of potassium into a multivitamin tablet that weighs about 1g in total and has a lot of other things in there too. So, they usually just skip it entirely, or include a very tiny amount.
So, if you want to supplement, soluble powder is probably better than tablets; here’s an example product on Amazon—by all means feel free to shop around.
Additionally, you might want to consider, if you use salt in your cooking, switching sodium chloride (table salt, sea salt, rock salt, etc) for potassium chloride, which is also “salty” to the taste but has the double-effect of reducing your sodium intake while increasing your potassium intake.
“Low sodium salt” as sold in supermarkets is very often a mixture of sodium chloride and potassium chloride—check the labels, and try to choose one with a good potassium ratio.
See also: Why the WHO has recommended switching to a healthier salt alternative
Want to learn more?
Check out:
10 Ways To Lower Blood Pressure Naturally ← getting more potassium is #3 on the list!
Take care!
Share This Post
-
What Your Hormones Mean For Weight Gain/Loss
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Kait Ann-Michelle describes herself as an “exercise scientist”, so what does that mean?
It means: she has an MS in exercise science, and an MA in clinical psychology.
With this mind, here’s what she has to say about hormones, weight gain/loss, and more:
What she wants us to know
Things to bear in mind over a certain age include:
- That “certain age” is about 35. If that seems a lifetime ago to you, in a way it could well be, if your hormones were very different then. In popular culture, menopause is often played as a joke, and the bar for having passed it is usually set quite high. But since the hormonal changes themselves begin nearer 35, that’s where to start examining things.
- A lot of online advice is woefully inappropriate for women over that age. Which is quite an injustice, as the 25–35 age range is such a tiny slice of life, yet it seems 80–90% of everything is aimed at it and tailored for it.
- Estrogen gets talked about a lot, but there are many hormones involved in perimenopausal symptoms, as one thing affects another, and before you know it, estrogen, progesterone, and even non-sex hormones like cortisol, insulin, thyroid hormones, and melatonin can be entirely out from where they should be. And the longer this goes on, the more pronounced and deep-rooted the effects.
- That goes for weight too, especially given the cortisol, insulin, and thyroid imbalances.
- It’s not just a case of “one hormone affects another”, either. Yes, it’s that too, but for example if you have a mood swing due to low estrogen, which creates a stressful situation that ups your cortisol, then you don’t sleep so well, then the next day you are more tired so you skip the exercise you planned, and then and then and then… In short, lifestyle factors matter a lot too; they affect, and are affected by, our hormones.
- All of this does tend to lead to weight gain if mismanaged.
- She advises advises taking up HRT once it becomes appropriate (which for most women means around menopause—though other conditions can make HRT indicated earlier or in some cases not at all), and/but also focusing a lot on “lifestyle medicine”, that is to say, diet and exercise, good sleep, stress management, and so forth.
- All of this does tend to lead to weight loss/maintenance if managed correctly.
- She doesn’t recommend guesswork when it comes to hormones, though, and rather recommends getting regularly tested for: thyroid panel, estradiol, progesterone, DHEAS, testosterone, CBC, lipid panel, CMP, and hemoglobin A1c, as well as, ideally, “nice-to-have lab values” of cortisol, IGF1, vitamin D3, homocysteine, B12, SHBG, FSH, LH, iron, ferritin, and CRP.
- That’s a lot of tests, so note, they’re in relative order of importance.
She notes that your doctor probably won’t want to do all those and will probably try to talk you out of them, so be prepared to advocate for yourself, as comprehensive lab work gives a full picture that the bare minimum does not.
For more details on all of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- What Does “Balance Your Hormones” Even Mean?
- What You Should Have Been Told About The Menopause Beforehand
- HRT: A Tale Of Two Approaches (Bioidentical vs Animal)
- HRT & Your Heart
- Hormones & Health, Beyond The Obvious
Take care!
Share This Post
- That “certain age” is about 35. If that seems a lifetime ago to you, in a way it could well be, if your hormones were very different then. In popular culture, menopause is often played as a joke, and the bar for having passed it is usually set quite high. But since the hormonal changes themselves begin nearer 35, that’s where to start examining things.


-
Kidney Beans vs Red Lentils – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing kidney beans to red lentils, we picked the lentils.
Why?
Both are excellent! But…
In terms of macros, kidney beans have more carbs, while the lentils have more fiber and protein; an easy first-round win for lentils.
In the category of vitamins, kidney beans have more vitamin K (appropriately enough), while lentils have more of vitamins B1, B2, B3, B5, B6, B7, B9, C, and E, winning this round too.
Looking at minerals, kidney beans have more calcium and magnesium, while lentils have more copper, iron, manganese, phosphorus, selenium, and zinc, winning their third round in a row.
Adding up the sections makes for a clear overall win for red lentils, but by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like:
What Do The Different Kinds Of Fiber Do? 30 Foods That Rank Highest
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Why do some people need less sleep than others? A gene variation could have something to do with it
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Have you ever noticed how some people bounce out of bed after just a few hours of sleep, while others can barely function without a solid eight hours?
Take Margaret Thatcher, for example. The former British prime minister was known for sleeping just four hours a night. She worked late, rose early, and seemed to thrive on little sleep.
But for most of us, that kind of sleep schedule would be disastrous. We’d be groggy, unfocused, and reaching for sugary snacks and caffeinated drinks by mid-morning.
So why do some people seem to need less sleep than others? It’s a question that’s fascinated scientists for years. Here’s what we know so far.
Maria Korneeva/Getty Images Natural short sleepers
There is a small group of people who don’t need much sleep. We call them natural short sleepers. They can function perfectly well on just four to six hours of sleep each night, often for their entire lives.
Generally they don’t feel tired, they don’t nap, and they don’t suffer the usual negative consequences of sleep deprivation. Scientists call this the natural short sleep phenotype – a biological trait that allows people to get all the benefits of sleep in less time.
In 2010 researchers discovered genetic mutations that help explain this phenomenon. Natural short sleepers carry rare variants in certain genes, which seem to make their sleep more efficient.
More recently, a 2025 study assessed a woman in her 70s with one of these rare mutations. Despite sleeping just six hours a night for most of her life, she remained physically healthy, mentally sharp, and led a full, active life. Her body, it seems, was simply wired to need less sleep.
We’re still learning about how common these genetic mutations are and why they occur.
Not everyone who sleeps less is a natural short sleeper
But here’s the catch: most people who think they’re natural short sleepers aren’t. They’re just chronically sleep-deprived. Often, their short sleep is due to long work hours, social commitments, or a belief sleeping less is a sign of strength or productivity.
In today’s hustle culture, it’s common to hear people boast about getting by on only a few hours of sleep. But for the average person, that’s not sustainable.
The effects of short sleep build up over time, creating what’s known as a “sleep debt”. This can lead to poor concentration, mood swings, micro-sleeps (brief lapses into sleep), reduced performance and even long-term health risks. For example, short sleep has been linked to an increased risk of obesity, diabetes, high blood pressure and cardiovascular disease (heart disease and stroke).
The weekend catch-up dilemma
To make up for lost sleep during the week, many people try to “catch up” on weekends.
This can help repay some of the sleep debt that has accumulated in the short term. Research suggests getting one to two extra hours of sleep on the weekend or taking naps when possible may help reduce the negative effects of short sleep.
However, it’s not a perfect fix. Weekend catch-up sleep and naps may not fully resolve sleep debt. The topic remains one of ongoing scientific debate.
A recent large study suggested weekend catch-up sleep may not offset the cardiovascular risks associated with chronic short sleep.
Catching up on sleep on the weekends may not fully resolve your ‘sleep debt’. Ground Picture/Shutterstock What’s more, large swings in sleep timing can disrupt your body’s internal clock, and sleeping in too much on weekends may make it harder to fall asleep on Sunday night, which can mean starting the working week less rested.
Increasing evidence indicates repeated cycles of irregular sleep may have an important influence on general health and the risk of early death, potentially even more so than how long we sleep for.
Ultimately, while moderate catch-up sleep might offer some benefits, it’s no substitute for consistent, high-quality sleep throughout the week. That said, maintaining such regularity can be particularly challenging for people with non-traditional schedules, such as shift workers.
So, was Thatcher a true natural short sleeper?
It’s hard to say. Some reports suggest she napped during the day in the back of a car between meetings. That could mean she was simply sleep-deprived and compensating for an accumulated sleep debt when she could.
Separate to whether someone is a natural short sleeper, there are a range of other reasons people may need more or less sleep than others. Factors such as age and underlying health conditions can significantly influence sleep requirements.
For example, older adults often experience changes in their circadian rhythms and are more likely to suffer from fragmented sleep due to conditions such as arthritis or cardiovascular disease.
Sleep needs vary from person to person, and while a lucky few can thrive on less, most of us need seven to nine hours a night to feel and function our best. If you’re regularly skimping on sleep and relying on weekends to catch up, it might be time to rethink your routine. After all, sleep isn’t a luxury – it’s a biological necessity.
Kelly Sansom, Research Associate, College of Medicine and Public Health, Flinders University; Research Associate, Centre for Healthy Ageing, Murdoch University and Peter Eastwood, Deputy Vice Chancellor, Research and Innovation, Murdoch University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What’s the difference between a heart attack and cardiac arrest? One’s about plumbing, the other wiring
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In July 2023, rising US basketball star Bronny James collapsed on the court during practice and was sent to hospital. The 18-year-old athlete, son of famous LA Lakers’ veteran LeBron James, had experienced a cardiac arrest.
Many media outlets incorrectly referred to the event as a “heart attack” or used the terms interchangeably.
A cardiac arrest and a heart attack are distinct yet overlapping concepts associated with the heart.
With some background in how the heart works, we can see how they differ and how they’re related.
Explode/Shutterstock Understanding the heart
The heart is a muscle that contracts to work as a pump. When it contracts it pushes blood – containing oxygen and nutrients – to all the tissues of our body.
For the heart muscle to work effectively as a pump, it needs to be fed its own blood supply, delivered by the coronary arteries. If these arteries are blocked, the heart muscle doesn’t get the blood it needs.
This can cause the heart muscle to become injured or die, and results in the heart not pumping properly.
Heart attack or cardiac arrest?
Simply put, a heart attack, technically known as a myocardial infarction, describes injury to, or death of, the heart muscle.
A cardiac arrest, sometimes called a sudden cardiac arrest, is when the heart stops beating, or put another way, stops working as an effective pump.
In other words, both relate to the heart not working as it should, but for different reasons. As we’ll see later, one can lead to the other.
Why do they happen? Who’s at risk?
Heart attacks typically result from blockages in the coronary arteries. Sometimes this is called coronary artery disease, but in Australia, we tend to refer to it as ischaemic heart disease.
The underlying cause in about 75% of people is a process called atherosclerosis. This is where fatty and fibrous tissue build up in the walls of the coronary arteries, forming a plaque. The plaque can block the blood vessel or, in some instances, lead to the formation of a blood clot.
Atherosclerosis is a long-term, stealthy process, with a number of risk factors that can sneak up on anyone. High blood pressure, high cholesterol, diet, diabetes, stress, and your genes have all been implicated in this plaque-building process.
Other causes of heart attacks include spasms of the coronary arteries (causing them to constrict), chest trauma, or anything else that reduces blood flow to the heart muscle.
Regardless of the cause, blocking or reducing the flow of blood through these pipes can result in the heart muscle not receiving enough oxygen and nutrients. So cells in the heart muscle can be injured or die.
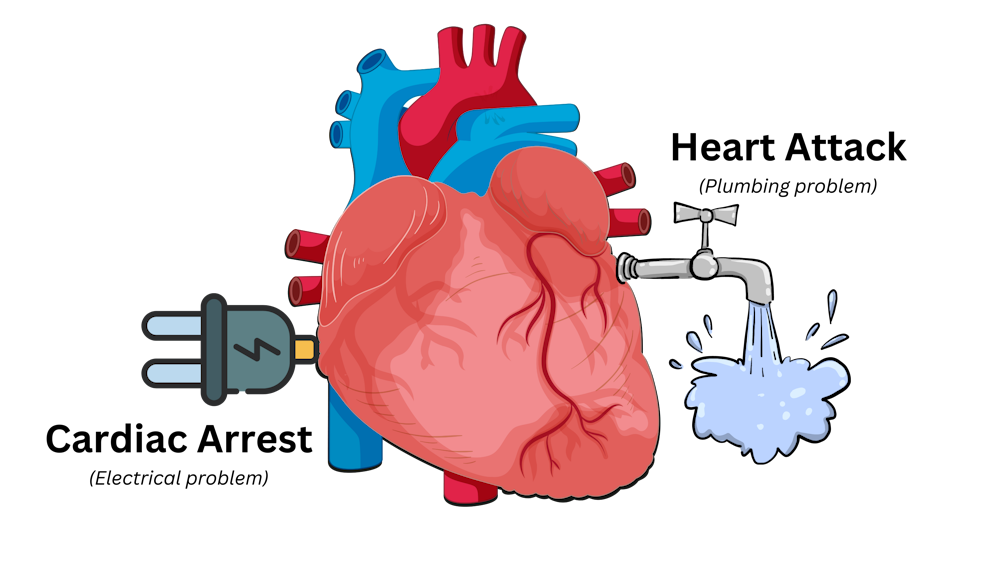
Here’s a simple way to remember the difference. Author provided But a cardiac arrest is the result of heartbeat irregularities, making it harder for the heart to pump blood effectively around the body. These heartbeat irregularities are generally due to electrical malfunctions in the heart. There are four distinct types:
- ventricular tachycardia: a rapid and abnormal heart rhythm in which the heartbeat is more than 100 beats per minute (normal adult, resting heart rate is generally 60-90 beats per minute). This fast heart rate prevents the heart from filling with blood and thus pumping adequately
- ventricular fibrillation: instead of regular beats, the heart quivers or “fibrillates”, resembling a bag of worms, resulting in an irregular heartbeat greater than 300 beats per minute
- pulseless electrical activity: arises when the heart muscle fails to generate sufficient pumping force after electrical stimulation, resulting in no pulse
- asystole: the classic flat-line heart rhythm you see in movies, indicating no electrical activity in the heart.
Remember this flat-line rhythm from the movies? It’s asystole, when there’s no electrical activity in the heart. Kateryna Kon/Shutterstock Cardiac arrest can arise from numerous underlying conditions, both heart-related and not, such as drowning, trauma, asphyxia, electrical shock and drug overdose. James’ cardiac arrest was attributed to a congenital heart defect, a heart condition he was born with.
But among the many causes of a cardiac arrest, ischaemic heart disease, such as a heart attack, stands out as the most common cause, accounting for 70% of all cases.
So how can a heart attack cause a cardiac arrest? You’ll remember that during a heart attack, heart muscle can be damaged or parts of it may die. This damaged or dead tissue can disrupt the heart’s ability to conduct electrical signals, increasing the risk of developing arrhythmias, possibly causing a cardiac arrest.
So while a heart attack is a common cause of cardiac arrest, a cardiac arrest generally does not cause a heart attack.
What do they look like?
Because a cardiac arrest results in the sudden loss of effective heart pumping, the most common signs and symptoms are a sudden loss of consciousness, absence of pulse or heartbeat, stopping of breathing, and pale or blue-tinged skin.
But the common signs and symptoms of a heart attack include chest pain or discomfort, which can show up in other regions of the body such as the arms, back, neck, jaw, or stomach. Also frequent are shortness of breath, nausea, light-headedness, looking pale, and sweating.
What’s the take-home message?
While both heart attack and cardiac arrest are disorders related to the heart, they differ in their mechanisms and outcomes.
A heart attack is like a blockage in the plumbing supplying water to a house. But a cardiac arrest is like an electrical malfunction in the house’s wiring.
Despite their different nature both conditions can have severe consequences and require immediate medical attention.
Michael Todorovic, Associate Professor of Medicine, Bond University and Matthew Barton, Senior lecturer, School of Nursing and Midwifery, Griffith University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: