International Women’s Day (and what it can mean for you, really)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How to not just #EmbraceEquity, but actually grow it, this International Women’s Day!
It’s International Women’s Day, and there’s a lot going on beyond the hashtagging! So, what’s happening, and how could you get involved in more than a “token” way in your workplace, business, or general life?
Well, that depends on your own environment and circumstances, but for example…
A feminist policy for productivity in the food sector?
We tend to think that in this modern world, we all have equal standing when it comes to productivity, food, and health. And yet…
❝If women do 70 per cent of the work in agriculture worldwide, but the land is mainly owned by men, then we don’t have equity yet. If in Germany, only one-tenth of female farmers manage the farm on which they work on, while they also manage the household, then there is no equity yet❞
~ Lea Leimann, Germany
What to do about it, though? It turns out there’s a worldwide organization dedicated to fixing this! It’s called Slow Food.
Their mission is to make food…
- GOOD: quality, flavorsome and healthy food
- CLEAN: production that does not harm the environment
- FAIR: accessible prices for consumers and fair conditions and pay for producers
…and yes, that explicitly includes feminism-attentive food policy:
Read all about it: Slow Food women forge change in the food system
Do you work in the food system?
If so, you can have an impact. Your knee-jerk reaction might be “I don’t”, but there are a LOT of steps from farm-to-table, so, are you sure?
Story time: me, I’m a writer (you’d never have guessed, right?) and wouldn’t immediately think of myself as working “in the food system”.
But! Not long back I (a woman) was contracted by a marketing agent (a woman) to write marketing materials for a small business (owned by a woman) selling pickles and chutneys across the Australian market, based on the recipes she learned from her mother, in India. The result?
I made an impact in the food chain the other side of the planet from me, without leaving my desk.
Furthermore, the way I went about my work empowered—at the very least—myself and the end client (the lady making and selling the pickles and chutneys).
Sometimes we can’t change the world by ourselves… but we don’t have to.
If we all just nudge things in the right direction, we’ll end up with a healthier, better-fed, more productive system for all!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Basil vs Oregano – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing basil to oregano, we picked the basil.
Why?
You may be thinking: these are just herbs; we don’t eat enough of these for the nutritional values to be relevant!
And to this we say: there’s nothing stopping you :p Herbs are full of flavor and goodness and there is really no reason to deny yourself. On this note, check out the sabzi khordan (traditional Levantine herb platter), linked below. You’ll start thinking about herbs in new ways, and you can thank us later!
Now, in terms of macros, nominally basil has more protein and oregano has more carbs and fiber, but the numbers are so close in each case that we’re going to call this category a tie.
When it comes to vitamins, things get more interesting: basil has more of vitamins B2, B3, B6, B9, K, and choline, while oregano has more of vitamins A, B1, B5, C, and E. This means a 6:5 win for basil, but note how the two herbs together give an impressive vitamin coverage. In other words, they complement each other nutritionally, not just culinarily!
In the category of minerals, basil has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium and zinc, while oregano has more selenium. Now, this is obviously a clear win for basil, but we’d like to highlight that both of these herbs are incredibly rich in minerals (i.e. oregano is a very good source of all those minerals we listed for basil, too!); it’s just that basil has even more of most of them.
When looking at any nutrient-dense food (which most herbs are), it’s worth looking at polyphenols. In this case, both are very abundant in polyphenols, and/but their respective numbers are close enough to be within each other’s margin of variation (i.e. exact numbers will depend on the individual plant’s life history), so this category is a tie.
Adding up the sections makes for an overall clear win for basil, but absolutely please do enjoy both unless you have a good reason not to—they complement each other so well, in nutrients as well as in flavor!
Want to learn more?
You might like to read:
- Cilantro vs Parsley – Which is Healthier?
- Holy Basil: What Does (And Doesn’t) It Do?
- Invigorating Sabzi Khordan (A Traditional Levantine Platter Of Herbs & Accompaniments)
Enjoy!
Share This Post
-
Over-50s Physio: What My 5 Oldest Patients (Average Age 92) Do Right
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Oftentimes, people of particularly advanced years will be asked their secret to longevity, and sometimes the answers aren’t that helpful because they don’t actually know, and ascribe it to some random thing. Will Harlow, the over-50s specialist physio, talks about the top 5 science-based things that his 5 oldest patients do, that enhances the healthy longevity that they are enjoying:
The Top 5’s Top 5
Here’s what they’re doing right:
Daily physical activity: all five patients maintain a consistent habit of daily exercise, which includes activities like exercise classes, home workouts, playing golf, or taking daily walks. They prioritize movement even when it’s difficult, rarely skipping a day unless something serious happened. A major motivator was the fear of losing mobility, as they had seen spouses, friends, or family members stop exercising and never start again.
Stay curious: a shared trait among the patients was their curiosity and eagerness to learn. They enjoy meeting new people, exploring new experiences, and taking on new challenges. Two of them attended the University of the Third Age to learn new skills, while another started playing bridge as a new hobby. The remaining two have recently made new friends. They all maintain a playful attitude, a good sense of humor, and aren’t afraid to fail or laugh at themselves.
Prioritize sleep (but not too much): the patients each average seven hours of sleep per night, aligning with research suggesting that 7–9 hours of sleep is ideal for health. They maintain consistent sleep and wake-up times, which contributes to their well-being. While they allow themselves short naps when needed, they avoid long afternoon naps to avoid disrupting their sleep patterns.
Spend time in nature: spending time outdoors is a priority for all five individuals. Whether through walking, gardening, or simply sitting on a park bench, they make it a habit to connect with nature. This aligns with studies showing that time spent in natural environments, especially near water, significantly reduces stress. When water isn’t accessible, green spaces still provide a beneficial boost to mental health.
Stick to a routine: the patients all value simple daily routines, such as enjoying an evening cup of tea, taking a daily walk, or committing to small gardening tasks. These routines offer mental and physical grounding, providing stability even when life becomes difficult sometimes. They emphasized the importance of keeping routines simple and manageable to ensure they could stick to them regardless of life’s challenges.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Top 8 Habits Of The Top 1% Healthiest Over-50s ← another approach to the same question, this time with a larger sample size, and/but many younger (than 90s) respondents.
Take care!
Share This Post
-

The Case of the Armadillo: Is It Spreading Leprosy in Florida?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
GAINESVILLE, Fla. — In an open-air barn at the edge of the University of Florida, veterinarian Juan Campos Krauer examines a dead armadillo’s footpads and ears for signs of infection.
Its claws are curled tight and covered in blood. Campos Krauer thinks it was struck in the head while crossing a nearby road.
He then runs a scalpel down its underside. He removes all the important organs: heart, liver, kidneys. Once the specimens are bottled up, they’re destined for an ultra-cold freezer in his lab at the college.
Campos Krauer plans to test the armadillo for leprosy, an ancient illness also known as Hansen’s disease that can lead to nerve damage and disfigurement in humans. He and other scientists are trying to solve a medical mystery: why Central Florida has become a hot spot for the age-old bacteria that cause it.
Leprosy remains rare in the United States. But Florida, which often reports the most cases of any state, has seen an uptick in patients. The epicenter is east of Orlando. Brevard County reported a staggering 13% of the nation’s 159 leprosy cases in 2020, according to a Tampa Bay Times analysis of state and federal data.
Many questions about the phenomenon remain unanswered. But leprosy experts believe armadillos play a role in spreading the illness to people. To better understand who’s at risk and to prevent infections, about 10 scientists teamed up last year to investigate. The group includes researchers from the University of Florida, Colorado State University, and Emory University in Atlanta.
“How this transmission is happening, we really don’t know,” said Ramanuj Lahiri, chief of the laboratory research branch for the National Hansen’s Disease Program, which studies the bacteria involved and cares for leprosy patients across the country.
‘Nothing Was Adding Up’
Leprosy is believed to be the oldest human infection in history. It probably has been sickening people for at least 100,000 years. The disease is highly stigmatized — in the Bible, it was described as a punishment for sin. In more modern times, patients were isolated in “colonies” around the world, including in Hawaii and Louisiana.
In mild cases, the slow-growing bacteria cause a few lesions. If left untreated, they can paralyze the hands and feet.
But it’s actually difficult to fall ill with leprosy, as the infection isn’t very contagious. Antibiotics can cure the ailment in a year or two. They’re available for free through the federal government and the World Health Organization, which launched a campaign in the 1990s to eliminate leprosy as a public health problem.
In 2000, reported U.S. cases dropped to their lowest point in decades with 77 infections. But they later increased, averaging about 180 per year from 2011 to 2020, according to data from the National Hansen’s Disease Program.
During that time, a curious trend emerged in Florida.
In the first decade of the 21st century, the state logged 67 cases. Miami-Dade County noted 20 infections — the most of any Florida county. The vast majority of its cases were acquired outside the U.S., according to a Times analysis of Florida Department of Health data.
But over the next 10 years, recorded cases in the state more than doubled to 176 as Brevard County took center stage.
The county, whose population is about a fifth the size of Miami-Dade’s, logged 85 infections during that time — by far the most of any county in the state and nearly half of all Florida cases. In the previous decade, Brevard noted just five cases.
Remarkably, at least a quarter of Brevard’s infections were acquired within the state, not while the individuals were abroad. India, Brazil, and Indonesia diagnose more leprosy cases than anywhere, reporting over 135,000 infections combined in 2022 alone. People were getting sick even though they hadn’t traveled to such areas or been in close contact with existing leprosy patients, said Barry Inman, a former epidemiologist at the Brevard health department who investigated the cases and retired in 2021.
“Nothing was adding up,” Inman said.
A few patients recalled touching armadillos, which are known to carry the bacteria. But most didn’t, he said. Many spent a lot of time outdoors, including lawn workers and avid gardeners. The cases were usually mild.
It was difficult to nail down where people got the illness, he added. Because the bacteria grow so slowly, it can take anywhere from nine months to 20 years for symptoms to begin.
Amoeba or Insect Culprits?
Heightened awareness of leprosy could play a role in Brevard’s groundswell of cases.
Doctors must report leprosy to the health department. Yet Inman said many in the county didn’t know that, so he tried to educate them after noticing cases in the late 2000s.
But that’s not the sole factor at play, Inman said.
“I don’t think there’s any doubt in my mind that something new is going on,” he said.
Other parts of Central Florida have also recorded more infections. From 2011 to 2020, Polk County logged 12 cases, tripling its numbers compared with the previous 10 years. Volusia County noted 10 cases. It reported none the prior decade.
Scientists are honing in on armadillos. They suspect the burrowing critters may indirectly cause infections through soil contamination.
Armadillos, which are protected by hard shells, serve as good hosts for the bacteria, which don’t like heat and can thrive in the animals whose body temperatures range from a cool 86-95 degrees.
Colonists probably brought the disease to the New World hundreds of years ago, and somehow armadillos became infected, said Lahiri, the National Hansen’s Disease Program scientist. The nocturnal mammals can develop lesions from the illness just as humans can. More than 1 million armadillos occupy Florida, estimated Campos Krauer, an assistant professor in the University of Florida’s Department of Large Animal Clinical Sciences.
How many carry leprosy is unclear. A study published in 2015 of more than 600 armadillos in Alabama, Florida, Georgia, and Mississippi found that about 16% showed evidence of infection. Public health experts believe leprosy was previously confined to armadillos west of the Mississippi River, then spread east.
Handling the critters is a known hazard. Lab research shows that single-cell amoebas, which live in soil, can also carry the bacteria.
Armadillos love to dig up and eat earthworms, frustrating homeowners whose yards they damage. The animals may shed the bacteria while hunting for food, passing it to amoebas, which could later infect people.
Leprosy experts also wonder if insects help spread the disease. Blood-sucking ticks might be a culprit, lab research shows.
“Some people who are infected have little to no exposure to the armadillo,” said Norman Beatty, an assistant professor of medicine at the University of Florida. “There is likely another source of transmission in the environment.”
Campos Krauer, who’s been searching Gainesville streets for armadillo roadkill, wants to gather infected animals and let them decompose in a fenced-off area, allowing the remains to soak into a tray of soil while flies lay eggs. He hopes to test the dirt and larvae to see if they pick up the bacteria.
Adding to the intrigue is a leprosy strain found only in Florida, according to scientists.
In the 2015 study, researchers discovered that seven armadillos from the Merritt Island National Wildlife Refuge, which is mostly in Brevard but crosses into Volusia, carried a previously unseen version of the pathogen.
Ten patients in the region were stricken with it, too. At the genetic level, the strain is similar to another type found in U.S. armadillos, said Charlotte Avanzi, a Colorado State University researcher who specializes in leprosy.
It’s unknown if the strain causes more severe disease, Lahiri said.
Reducing Risk
The public should not panic about leprosy, nor should people race to euthanize armadillos, researchers warn.
Scientists estimate that over 95% of the global human population has a natural ability to ward off the disease. They believe months of exposure to respiratory droplets is needed for person-to-person transmission to occur.
But when infections do happen, they can be devastating.
“If we better understand it,” Campos Krauer said, “the better we can learn to live with it and reduce the risk.”
The new research may also provide insight for other Southern states. Armadillos, which don’t hibernate, have been moving north, Campos Krauer said, reaching areas like Indiana and Virginia. They could go farther due to climate change.
People concerned about leprosy can take simple precautions, medical experts say. Those working in dirt should wear gloves and wash their hands afterward. Raising garden beds or surrounding them with a fence may limit the chances of soil contamination. If digging up an armadillo burrow, consider wearing a face mask, Campos Krauer said.
Don’t play with or eat the animals, added John Spencer, a scientist at Colorado State University who studies leprosy transmission in Brazil. They’re legal to hunt year-round in Florida without a license.
Campos Krauer’s team has so far examined 16 dead armadillos found on Gainesville area roads, more than 100 miles from the state’s leprosy epicenter, trying to get a preliminary idea of how many carry the bacteria.
None has tested positive yet.
This article was produced through a partnership between KFF Health News and the Tampa Bay Times.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-

Healthy Kids, Happy Kids – by Dr. Elisa Song
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you have young children or perhaps grandchildren, you probably care deeply about those children and their wellbeing, but there can often be a lot more guesswork than would be ideal, when it comes to ensuring they be and remain healthy.
Nevertheless, a lot of common treatments for children are based (whether parents know it or not—and often they dont) on what is most convenient for the parent, not necessarily what is best for the child. Dr. Song looks to correct that.
Rather than dosing kids with acetaminophen or even antibiotics, assuming eczema can be best fixed with a topical cream (treating the symptom rather than the cause, much?), and that some things like asthma “just are”, and “that’s unfortunate”, Dr. Song takes us on a tour of pediatric health, centered around the gut.
Why the gut? Well, it’s pretty central to us as adults, and it’s the same for kids, except one difference: their gut microbiome is changing even more quickly than ours (along with the rest of their body), and as such, is even more susceptible to little nudges for better or for worse, having a big impact in either direction. So, might as well make it a good one!
After an explanatory overview, most of the book is given over to recognizing and correcting what things can go wrong, including the top 25 acute childhood conditions, and the most critical chronic ones, and how to keep things on-track as a team (the child is part of the team! An important part!).
The style of the book is very direct and instructional; easy to understand throughout. It’s a lot like being in a room with a very competent pediatrician who knows her stuff and explains it well, thus neither patronizing nor mystifying.
Bottom line: if there are kids in your life, be they yours or your grandkids or someone else, this is a fine book for giving them the best foundational health.
Click here to check out Healthy Kids, Happy Kids, and take care of yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What’s the difference between Alzheimer’s and dementia?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
Changes in thinking and memory as we age can occur for a variety of reasons. These changes are not always cause for concern. But when they begin to disrupt daily life, it could indicate the first signs of dementia.
Another term that can crop up when we’re talking about dementia is Alzheimer’s disease, or Alzheimer’s for short.
So what’s the difference?

Lightspring/Shutterstock What is dementia?
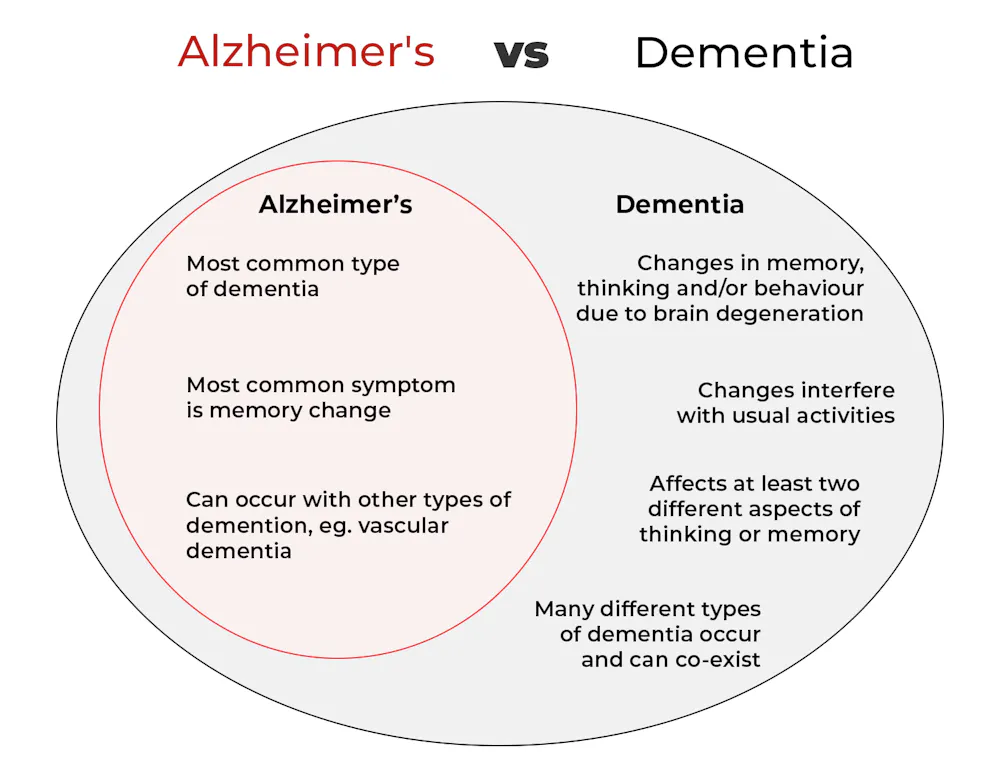
Dementia is an umbrella term used to describe a range of syndromes that result in changes in memory, thinking and/or behaviour due to degeneration in the brain.
To meet the criteria for dementia these changes must be sufficiently pronounced to interfere with usual activities and are present in at least two different aspects of thinking or memory.
For example, someone might have trouble remembering to pay bills and become lost in previously familiar areas.
It’s less-well known that dementia can also occur in children. This is due to progressive brain damage associated with more than 100 rare genetic disorders. This can result in similar cognitive changes as we see in adults.
So what’s Alzheimer’s then?
Alzheimer’s is the most common type of dementia, accounting for about 60-80% of cases.
So it’s not surprising many people use the terms dementia and Alzheimer’s interchangeably.
Changes in memory are the most common sign of Alzheimer’s and it’s what the public most often associates with it. For instance, someone with Alzheimer’s may have trouble recalling recent events or keeping track of what day or month it is.
People with dementia may have trouble keeping track of dates. Daisy Daisy/Shutterstock We still don’t know exactly what causes Alzheimer’s. However, we do know it is associated with a build-up in the brain of two types of protein called amyloid-β and tau.
While we all have some amyloid-β, when too much builds up in the brain it clumps together, forming plaques in the spaces between cells. These plaques cause damage (inflammation) to surrounding brain cells and leads to disruption in tau. Tau forms part of the structure of brain cells but in Alzheimer’s tau proteins become “tangled”. This is toxic to the cells, causing them to die. A feedback loop is then thought to occur, triggering production of more amyloid-β and more abnormal tau, perpetuating damage to brain cells.
Alzheimer’s can also occur with other forms of dementia, such as vascular dementia. This combination is the most common example of a mixed dementia.
Vascular dementia
The second most common type of dementia is vascular dementia. This results from disrupted blood flow to the brain.
Because the changes in blood flow can occur throughout the brain, signs of vascular dementia can be more varied than the memory changes typically seen in Alzheimer’s.
For example, vascular dementia may present as general confusion, slowed thinking, or difficulty organising thoughts and actions.
Your risk of vascular dementia is greater if you have heart disease or high blood pressure.
Frontotemporal dementia
Some people may not realise that dementia can also affect behaviour and/or language. We see this in different forms of frontotemporal dementia.
The behavioural variant of frontotemporal dementia is the second most common form (after Alzheimer’s disease) of younger onset dementia (dementia in people under 65).
People living with this may have difficulties in interpreting and appropriately responding to social situations. For example, they may make uncharacteristically rude or offensive comments or invade people’s personal space.
Semantic dementia is also a type of frontotemporal dementia and results in difficulty with understanding the meaning of words and naming everyday objects.
Dementia with Lewy bodies
Dementia with Lewy bodies results from dysregulation of a different type of protein known as α-synuclein. We often see this in people with Parkinson’s disease.
So people with this type of dementia may have altered movement, such as a stooped posture, shuffling walk, and changes in handwriting. Other symptoms include changes in alertness, visual hallucinations and significant disruption to sleep.
Do I have dementia and if so, which type?
If you or someone close to you is concerned, the first thing to do is to speak to your GP. They will likely ask you some questions about your medical history and what changes you have noticed.
Sometimes it might not be clear if you have dementia when you first speak to your doctor. They may suggest you watch for changes or they may refer you to a specialist for further tests.
There is no single test to clearly show if you have dementia, or the type of dementia. A diagnosis comes after multiple tests, including brain scans, tests of memory and thinking, and consideration of how these changes impact your daily life.
Not knowing what is happening can be a challenging time so it is important to speak to someone about how you are feeling or to reach out to support services.
Dementia is diverse
As well as the different forms of dementia, everyone experiences dementia in different ways. For example, the speed dementia progresses varies a lot from person to person. Some people will continue to live well with dementia for some time while others may decline more quickly.
There is still significant stigma surrounding dementia. So by learning more about the various types of dementia and understanding differences in how dementia progresses we can all do our part to create a more dementia-friendly community.
The National Dementia Helpline (1800 100 500) provides information and support for people living with dementia and their carers. To learn more about dementia, you can take this free online course.
Nikki-Anne Wilson, Postdoctoral Research Fellow, Neuroscience Research Australia (NeuRA), UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Reduce Caffeine’s Impact on Kidneys
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝Avid coffee drinker so very interested in the results Also question Is there something that you could take or eat that would prevent the caffeine from stimulating the kidneys? I tried to drink decaf from morning to night not a good result! Thanks❞
That is a good question! The simple answer is “no” (but keep reading, because all is not lost)
There’s no way (that we yet know of) to proof the kidneys against the stimulating effect of caffeine. This is especially relevant because part of caffeine’s stimulating effect is noradrenergic, and that “ren” in the middle there? It’s about the kidneys. This is just because the adrenal gland is situated next to them (actually, it’s pretty much sitting on top of them), hence the name, but it does mean that the kidneys are about the hardest thing in the body to have not effected by caffeine.
However! The effects of caffeine in general can be softened a little with l-theanine (found in tea, or it can be taken as a supplement). It doesn’t stop it from working, but it makes the curve of the effect a little gentler, and so it can reduce some unwanted side effects.
You can read more about l-theanine here:
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: