Intermittent fasting doesn’t have an edge for weight loss, but might still work for some
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Intermittent fasting has become a buzzword in nutrition circles, with many people looking to it as a way to lose weight or improve their health.
But new research from the Cochrane Collaboration shows intermittent fasting is no more effective for weight loss than receiving traditional dietary advice or even doing nothing at all.
In this international review, researchers assessed 22 studies involving 1,995 adults who were classified as overweight (with a body mass index of 25–29.9 kg/m²) or obese (with a BMI of 30 kg/m² or above) to assess the effectiveness of intermittent fasting for up to 12 months.
The authors found, when compared to energy restricted dieting, intermittent fasting doesn’t seem to work for people who are overweight or obese and are trying to lose weight. However they note intermittent fasting may still be a reasonable option for some people.

Remind me, what’s intermittent fasting?
Intermittent fasting is a tool for weight management, which includes three main strategies:
- alternate day fasting, where every second day is reduced to low or no energy intake
- periodic fasting or the 5:2 diet, where one or two days of the week are spent with low or no energy intake
- time-restricted eating or the 16:8 diet, where daily energy intake is reduced to a shorter window, usually between eight and ten waking hours.
What did previous research show?
Previous reviews have found differences between types of intermittent fasting.
Alternate day fasting, for example, resulted in more weight loss when compared to time-restricted eating.
This is because participants who fasted every second day consumed about 20% less energy than those following time-restricted eating.
What did the Cochrane review find?
Cochrane review use gold-standard techniques to give an objective overview of the evidence. This review looked at 22 individual randomised controlled trials published between 2016 and 2024 from North America, Europe, China, Australia and South America.
The trials compared the outcomes of almost 2,000 adults who were classified as being overweight or obese. These participants either:
- received standard dietary advice, such as restricting calories or eating different types of foods
- practised intermittent fasting
- received either regular dietary advice, no intervention or were on a wait list.
The authors found:
1. Intermittent fasting was no better than getting dietary advice
The researchers found intermittent fasting and receiving dietary advice to restrict energy intake led to similar levels of weight loss.
This finding was based on 21 studies involving 1,713 people, with the researchers measuring the change from the participants’ starting weight.
Dietary advice (from registered dietitians or trained researchers) could include an eating plan focused on fruit, vegetables, whole grains and seafood, restricting calories, or any specific dietary advice for weight loss.
The amount of weight the participants lost ranged from a 10% loss to a 1% gain, with either intermittent fasting or dietary advice.
These findings are similar to several recent meta-analyses which found intermittent fasting is no better than dieting.
Previous research has found most of the alternate day fasting and periodic diet studies leads to about 6% to 7% weight loss. This is compared to very low energy “shake” diets (about 10%), GLP-1 medications (15% to 20%) and surgery (above 20%).
The review also found intermittent fasting likely makes little difference to a person’s quality of life, based on only three studies.
2. Intermittent fasting was no better than doing nothing
The researchers found intermittent fasting and no intervention led to similar levels of weight loss. This finding was based on six studies involving 448 people.
In the intermittent fasting studies, participants experienced about 5% weight loss. The “no intervention” or control group lost about 2% of their original weight.
In research, a 3% difference in weight loss is not considered clinically meaningful. That’s why the authors of this review concluded intermittent fasting is no more effective for weight loss than doing nothing at all.
However, the result for the “no intervention” condition could be due to the Hawthorne effect: the tendency for people to behave differently because they know they are being watched, such as in a clinical trial.
What are the review’s limitations?
There were few large, high-quality randomised controlled trials to draw on.
Only six studies were included in the part of the review which compared intermittent fasting and doing nothing. Two of these focused on time-restricted eating, which is arguably the least effective weight-loss strategy. One looked at the effects of fasting for one day per week. The other three were intermittent fasting studies, each with varying control groups, where some received guidance and others did not.
Also, the review only looked at studies where the interventions lasted between six and 12 months. It’s possible intermittent fasting strategies could be a long-term tool for weight maintenance. So we need to do more research, and ideally studies of longer duration.
What about the other health benefits of fasting?
Studies have found intermittent fasting can lower blood pressure, improve fertility, and reduce the incidence of metabolic syndrome which refers to a group of conditions that increase the risk of cardiovascular disease.
In one 2024 study, researchers found intermittent fasting may lead to changes in metabolism and the gut that restrict how cancer develops. Another study from 2025 found intermittent fasting could improve the metabolic health of shift workers.
So if you’re practising or considering intermittent fasting, the current evidence suggests it can be a safe and effective way to manage your weight.
But for any weight loss strategy to work, it needs to align with your personal preferences. And it’s best to consult a health-care professional before starting any new diet, especially if you have any underlying health conditions.
Evelyn Parr, Research Fellow in Exercise Metabolism and Nutrition, Mary MacKillop Institute for Health Research, Australian Catholic University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Bell Pepper vs Celery – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing bell peppers to celery, we picked the celery.
Why?
First, you might remember that different color bell peppers have different nutritional profiles. So, you might be wondering why we didn’t specify the color.
The reason is: the things that differ from one color to another are important differences between the respective bell peppers, but they make no difference to this comparison, as for any given nutrient that changes from one color to another, it doesn’t change the outcome, because the numbers are still on the same side relative to celery.
With that in mind…
It was close!
In terms of macros, there’s really nothing between them, so the first round’s a tie.
In the category of vitamins, bell peppers have more of vitamins B1, B3, B6, C, and E, while celery has more of vitamins A, B2, B5, B7, B9, and K, yielding a marginal victory to celery here.
Looking at minerals, bell peppers have more coper, iron, and manganese, while celery has more calcium, magnesium, phosphorus, potassium, and selenium, winning another round.
In other considerations, bell peppers have more carotenoids such as lutein, while celery is rather higher in polyphenols, so we’ll call this round a tie.
Adding up the sections makes for a modest-yet-clear overall win for celery, but by all means enjoy either or both, as diversity is best!
Want to learn more?
You might like:
- Which Bell Peppers To Pick? A Spectrum Of Specialties ← for the differences between the different colors
- 21 Most Beneficial Polyphenols & What Foods Have Them
Enjoy!
Share This Post
-
How Fish Oil Can Harm Your Brain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Omega-3 fatty acids have many benefits for the health, including for the brain!
We wrote about some of them, here: What Omega-3 Fatty Acids Really Do For Us
There are even some less well-known benefits, such as: Why Healthy Teeth May Depend On Omega-3 & Exercise
Now, the press has not been all positive, for example: Fish Oil Can Backfire Without This Enzyme
But what’s this about omega-3s harming the brain?
Brain recovery impediment
Researchers (Dr. Eda Karakaya et al.) examined how omega-3 fatty acids from fish oil affect brain recovery, and the results were not happy ones.
In few words: the fish-derived omega-3 fatty acid EPA (eicosapentaenoic acid) accumulated in the brain and was linked to reduced recovery capacity after injury.
Further, EPA altered cortical gene programs by suppressing pathways involved in vascular repair* and extracellular matrix organization while increasing lipid metabolism activity.
*And this is critical. Regular 10almonds readers will remember that we often say “what’s good for your heart is good for your brain”, and it’s because the former feeds the latter, with nutrients, oxygen, etc, and also ultimately takes away detritus (yes, it’s the glymphatic system that does it directly, but without good blood flow, there’s nowhere for it to usefully drain to). So all this means that if cerebrovascular repair is impaired, then ultimately, brain maintenance will be impaired too.
More than just that, in human brain microvascular endothelial cells, EPA reduced the ability to form repair networks under conditions promoting fatty acid use.
And while no ethics board would let the researchers take brain slices from living human volunteers to look at under the microscope, postmortem brain samples from humans with chronic traumatic encephalopathy showed disrupted fatty acid balance and vascular-related gene changes consistent with EPA-linked effects.
In other words: a further smoking gun that strongly suggests (albeit does not outright prove, in this case) “EPA did this”.
There is one thing that’s not completely bad news for fish oil here, which is that DHA (docosahexaenoic acid), another omega-3 fatty acid, did not show the same negative effects and remains associated with normal brain structure.
But since fish oil contains both EPA and DHA in generous amounts, there’s a limit to how helpful this is:
❝Fish oil supplements are everywhere, and people take them for a range of reasons, often without a clear understanding of their long-term effects
But in terms of neuroscience, we still don’t know whether the brain has resilience or resistance to this supplement. That’s why ours is the first such study in the field.❞
~ Dr. Onder Albaryam, a colleague of Dr. Karakaya, and part of the “et al.” in this study
You can read the paper in full, here: Eicosapentaenoic acid reprograms cerebrovascular metabolism and impairs repair after brain injury, with relevance to chronic traumatic encephalopathy
Want to do better for your brain?
You do have other options!
For example, as well as the difference between EPA and DHA that we talked about above, there are also plant-based omega-3s that just have ALA (and not EPA or DHA) which the body can convert to whatever omega-3 form it needs (just like the fish did, for we too are animals that can do that, and for this reason our liver fats would, if healthy, also be a good source of EPA/DHA if something were to predate on us).
For more on that, check out: Omega-3s: Different Sources, Different Benefits?
Enjoy!
Share This Post
-
Can An AI Program Deliver Useful Psychotherapy?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There are increasing numbers of AI-based chat programs that boast the convenience of a therapist in your pocket, always ready to listen.
So far, things have not gone entirely without incident, as (for example) the tendency of such chatbots to be agreeable in the things they say, can worsen some people’s mental health, if the chatbot uncritically believes everything they say. This has been a big problem for people using OpenAI’s ChatGPT as a therapist (something its makers, to their credit, do not claim it is qualified to do), when ChatGPT has encouraged and exacerbated paranoia and delusions, due to its tendency to give agreeable “yes, and…” responses.
But, it’s been worse than that, too. Some chatbots have inadvertently encouraged users to kill themselves, in a (technically successful) attempt to be encouraging, in inappropriate response to users expressing uncertainty on the topic.
This is a problem with applying a large language model (LLM) approach without sufficient failsafes in place, because a LLM AI will hear, after a discussion of previous suicidal ideation, “Maybe I’ll really do it this time, I don’t know” and will check its database for a huge number of instances of those words, and determine that an appropriate response is “I believe in you, you will succeed if you put your mind to it”, for example.
A sensible middle ground?
Researchers have tried to boundary those potential pitfalls, to provide an AI that can help a user to manage some of the most common mental health concerns (e.g. depression, anxiety, etc), while raising the alarm (rather than overextending its reach) when it comes to serious risks such as those associated with suicidal ideation:
❝While these results are very promising, no generative AI agent is ready to operate fully autonomously in mental health where there is a very wide range of high-risk scenarios it might encounter.
Therabot is not limited to an office and can go anywhere a patient goes. It was available around the clock for challenges that arose in daily life and could walk users through strategies to handle them in real time. But the feature that allows AI to be so effective is also what confers its risk—patients can say anything to it, and it can say anything back.
This trial brought into focus that the study team has to be equipped to intervene—possibly right away—if a patient expresses an acute safety concern such as suicidal ideation, or if the software responds in a way that is not in line with best practices. Thankfully, we did not see this often with Therabot, but that is always a risk with generative AI, and our study team was ready.
We still need to better understand and quantify the risks associated with generative AI used in mental health contexts.❞
Dr. Heinz, quoted above, was a lead researcher on a study testing “Therabot”, and his colleague and fellow lead researcher Dr. Nicholas Jacobson boasts,
❝Our results are comparable to what we would see for people with access to gold-standard cognitive therapy with outpatient providers. We’re talking about potentially giving people the equivalent of the best treatment you can get in the care system over shorter periods of time.❞
You can read their paper here: Randomized Trial of a Generative AI Chatbot for Mental Health Treatment
Lower-tech smartphone options
When it comes to more basic things, such as Cognitive Behavioral Therapy (CBT), advanced AI may not be necessary, as CBT by its very nature lends itself well to being presented in a way that’s scarcely more complicated than a flowchart, with relatively little that can go wrong even when done by an app. For example:
Perhaps the lowest-tech way (that still involves tech) is journaling, using an app that provides journaling prompts. We discuss several of the options for that, here:
The Easiest Way To Take Up Journaling
Take care!
Share This Post



-
Don’t Train Harder (Yet); Fix Your Form First
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cori Lefkowitz, of Strong at Every Age, shows us how to make it count:
You might want to sit up and pay attention to this
Prioritizing “training harder” can cause more problems than you might expect, because progressing too quickly causes your hips and lower back to compensate. Instead, it’s best to work up very gradually. For example, build up from a pelvic tilt hold to a march, a double knee tuck, a single leg lower, and finally a double leg lower to properly train a posterior pelvic tilt, and protect your lower back.
Some other mistakes to avoid:
- Avoiding or misusing spinal flexion: include crunches and sit-ups since your abs are meant to flex your spine, and control the curl one vertebra at a time—round forwards as you reach towards your toes and lower with control—so you don’t rely on momentum or your hip flexors.
- Not focusing on true muscle engagement: prioritize curling your pelvis towards your ribs in reverse crunches and leg raises, monitor what you feel working, and regress or adjust if your hip flexors dominate instead of your abs.
- Prioritizing fatigue and quantity over quality and intensity: spread your ab work across three to four sessions per week, maintain controlled reps, and create full-body tension in movements like a plank by bracing your core, slightly tucking your pelvis, engaging your glutes and quads, and driving back through your heels so shorter, high-effort sets replace longer, relaxed holds.
In fewer words, the advice here is to avoid forcing advanced variations before mastering fundamentals, and instead focus on the controlled, intentional reps that actually build strong abs.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Is A Visible Six-Pack Obtainable Regardless Of Genetic Predisposition?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Why do some autistic people walk differently?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Autism is a neurodevelopmental condition that affects how people’s brains develop and function, impacting behaviour, communication and socialising. It can also involve differences in the way you move and walk – known as your “gait”.
Having an “odd gait” is now listed in the Diagnostic and Statistical Manual of Mental Disorders as a supporting diagnostic feature of autism.
What does this look like?
The most noticeable gait differences among autistic people are:
- toe-walking, walking on the balls of the feet
- in-toeing, walking with one or both feet turned inwards
- out-toeing, walking with one or both feet turned out.
Research has also identified more subtle differences. A study summarising 30 years of research among autistic people reports that gait is characterised by:
- walking more slowly
- taking wider steps
- spending longer in the “stance” phase, when the foot leaves the ground
- taking more time to complete each step.
Autistic people show much more personal variability in the length and speed of their strides, as well as their walking speed.
Gait differences also tend to occur alongside other motor differences, such as issues with balance, coordination, postural stability and handwriting. Autistic people may need support for these other motor skills.
What causes gait differences?
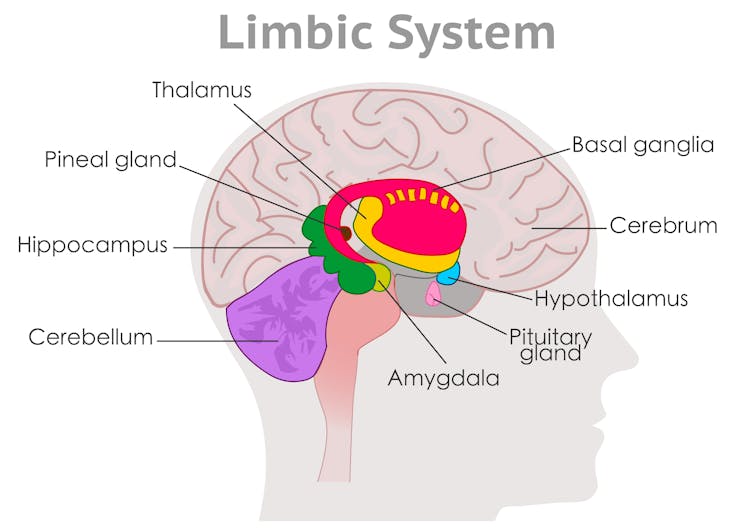
These are largely due to differences in brain development, specifically in areas known as the basal ganglia and cerebellum.
The basal ganglia are broadly responsible for sequencing movement including through shifting posture. It ensures your gait appears effortless, smooth and automatic.
The cerebellum then uses visual and proprioceptive information (to sense the body’s position and movement) to adjust and time movements to maintain postural stability. It ensures movement is controlled and coordinated.

Differences occur in the cerebellum and basal ganglia. grayjay/Shutterstock Developmental differences in these brain regions relate to the way the areas look (their structure), how they work (their function and activation) and how they “speak” to other areas of the brain (their connections).
While some researchers have suggested that autistic gait occurs due to delayed development, we now know gait differences persist across the lifespan. Some differences actually become clearer with age.
In addition to brain-based differences, the autistic gait is also associated with factors such as the person’s broader motor, language and cognitive capabilities.
People with more complex support needs might have more pronounced gait or motor differences, together with language and cognitive difficulties.
Motor dysregulation might indicate sensory or cognitive overload and be a useful marker that the person might benefit from extra support or a break.
How is it managed?
Not all differences need to be treated. Instead, clinicians take an individualised and goals-based approach.
Some autistic people might have subtle gait differences that are observable during testing. But if these differences don’t impact a person’s ability to participate in everyday life, they don’t require support.
An autistic person is likely to benefit from support for gait differences if they have a functional impact on their daily life. This might include:
- increased risk of, or frequent, falls
- difficulty participating in the physical activities they enjoy
- physical consequences such as tightness of the Achilles and calf muscles, or associated pain in other areas, such as the feet or back.
Some children may also benefit from support for motor skill development. However this doesn’t have to occur in a clinic.
Given children spend a large portion of their time at school, programs that integrate opportunities for movement throughout the school day allow autistic children to develop motor skills outside of the clinic and alongside peers. We developed the Joy of Moving Program in Australia, for example, which gets students moving in the classroom.
Our community-based intervention studies show autistic children’s movement abilities can improve after engaging in community-based interventions, such as sports or dance.
Community-based support models empower autistic children to have agency in how they move, rather than seeing different ways of moving as a problem to be fixed.
Where to from here?
While we have learnt a lot about autistic gait at a broad level, researchers and clinicians are still seeking a better understanding of why and when individual variability occurs.
We’re also still determining how to best support individual movement styles, including among children as they develop.
However there is growing evidence that physical activity enhances social skills and behavioural regulation in preschool children with autism.
So it’s encouraging that states and territories are moving towards more community-based foundational supports for autistic children and their peers, as governments develop supports outside the National Disability Insurance Scheme (NDIS).
The authors thank the late Emeritus Professor John Bradshaw for his early input into this piece.
Nicole Rinehart, Nicole Rinehart, Professor, Clinical Psychology, Director of the Neurodevelopment Program, School of Psychological Sciences, Faculty of Medicine, Nursing and Health Sciences, Monash University; Chloe Emonson, Research Fellow, School of Psychological Sciences, Monash University, and Ebony Renee Lindor, Senior Research Fellow and Senior Clinical Neuropsychologist, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Hit A Weight Loss Plateau? Here’s What To Do
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s very common for people to hit a plateau in our progress towards various goals.
When it comes to weight loss specifically, a large (n=24,035) study of mostly women (19.972/24,035 = 83.09%) aged 31–70 (with more than half being in the 51–70 range) has good news about this:
Most people who sustainably lose weight weight over the course of a year, have a plateau at some point, usually at least one three-month plateau.
The top three weight loss patterns were:
- 15% lost weight for 6 months, then maintained their weight for a further 6 months, resulting in an average 11kg weight loss after a year (12% of their starting body weight)
- 11% lost weight in the first 3 months, then maintained for 9 months, losing 5kg after a year (nearly 6% of their starting body weight)
- 9% lost weight for 9 months, followed by 3 months of maintenance, resulting in an average 16kg loss (17% of their starting body weight)
You can read the full paper here: Weight Loss Patterns and Outcomes Over 12 Months on a Commercial Weight Management Program (CSIRO Total Wellbeing Diet Online): Large-Community Cohort Evaluation Study
Did you notice the reframe there? What may be seen (and not welcomed) by the individual is a plateau, but what it also is objectively, is weight loss maintenance. In other words, not regaining weight, as we all know can be all too easy for many.
You may be thinking: “but I want to continue losing weight!”
And that’s fine. The trick is to use the maintenance phase (or plateau, if you want to call it that) as an opportunity to assess what’s working for you and what’s not, and where you want to go from here.
The chances are good that your metabolism has simply adapted to whatever diet/exercises changes you made to your lifestyle… And that’s good!
Three months ago, you wanted your body to have this new “set point”, and now you have it. Congratulations on the improved metabolism!
Now, imagine yourself starting again, but this time you’re starting with a better metabolism than last time you started. What will you do next to up the ante?
Whatever you do, we recommend making sure to do it healthily, for example: How To Lose Weight (Healthily!)
You might even want to coast for a little in a maintenance phase, and use the opportunity to improve related areas of your health, before diving back into your next weight loss phase.
For example, you might want to: Stop Trying To Lose Weight (And Do This Instead) ← this is about metabolic health in a more general fashion, and is very important
Alternatively, you might want to take the opportunity to build a little muscle (which in turn will improve your metabolic health, because muscle “costs” calories to maintain, while fat cues your body to dial down the metabolism to survive the famine for which it thinks you were preparing).
If you want to do that, then check out: Can You Gain Muscle & Lose Fat At The Same Time?
And if at any point your weight loss journey (or perhaps a plateau somewhere along such) is getting you down, then… You know the saying “have fun and be yourself”? The trick here is to have fun and be your best self. Seriously! Mindset is actually really important, not just for your mental health, but also for your physical health, and yes, also for weight loss specifically, if that’s your goal.
See: 8 Pillars of Weight Loss Explained ← Surprise, diet is #6 and exercise is #7, while emotional freedom and resilience is #1 😎
Want to know more?
Check out this trio of articles that’ll keep you on the right path:
- How To Plan For The Unplannable & Always Follow Through
- How To Avoid Slipping Into (Bad) Old Habits
- How To Keep On Keeping On… Long Term!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: