How Much Can Hypnotherapy Really Do?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sit Back, Relax, And…
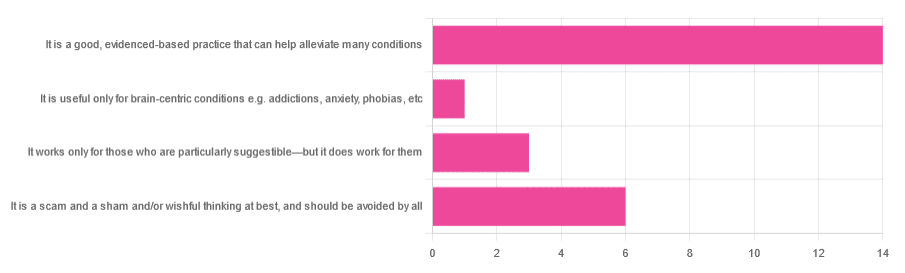
In Tuesday’s newsletter, we asked you for your opinions of hypnotherapy, and got the above-depicted, below-described, set of responses:
- About 58% said “It is a good, evidenced-based practice that can help alleviate many conditions”
- Exactly 25% said “It is a scam and sham and/or wishful thinking at best, and should be avoided by all”
- About 13% said “It works only for those who are particularly suggestible—but it does work for them”
- One (1) person said “It is useful only for brain-centric conditions e.g. addictions, anxiety, phobias, etc”
So what does the science say?
Hypnotherapy is all in the patient’s head: True or False?
True! But guess which part of your body controls much of the rest of it.
So while hypnotherapy may be “all in the head”, its effects are not.
Since placebo effect, nocebo effect, and psychosomatic effect in general are well-documented, it’s quite safe to say at the very least that hypnotherapy thus “may be useful”.
Which prompts the question…
Hypnotherapy is just placebo: True or False?
False, probably. At the very least, if it’s placebo, it’s an unusually effective placebo.
And yes, even though testing against placebo is considered a good method of doing randomized controlled trials, some placebos are definitely better than others. If a placebo starts giving results much better than other placebos, is it still a placebo? Possibly a philosophical question whose answer may be rooted in semantics, but happily we do have a more useful answer…
Here’s an interesting paper which: a) begins its abstract with the strong, unequivocal statement “Hypnosis has proven clinical utility”, and b) goes on to examine the changes in neural activity during hypnosis:
Brain Activity and Functional Connectivity Associated with Hypnosis
It works only for the very suggestible: True or False?
False, broadly. As with any medical and/or therapeutic procedure, a patient’s expectations can affect the treatment outcome.
And, especially worthy of note, a patient’s level of engagement will vastly affect it treatment that has patient involvement. So for example, if a doctor prescribes a patient pills, which the patient does not think will work, so the patient takes them intermittently, because they’re slow to get the prescription refilled, etc, then surprise, the pills won’t get as good results (since they’re often not being taken).
How this plays out in hypnotherapy: because hypnotherapy is a guided process, part of its efficacy relies on the patient following instructions. If the hypnotherapist guides the patient’s mind, and internally the patient is just going “nope nope nope, what a lot of rubbish” then of course it will not work, just like if you ask for directions in the street and then ignore them, you won’t get to where you want to be.
For those who didn’t click on the above link by the way, you might want to go back and have a look at it, because it included groups of individuals with “high/low hypnotizability” per several ways of scoring such.
It works only for brain-centric things, e.g. addictions, anxieties, phobias, etc: True or False?
False—but it is better at those. Here for example is the UK’s Royal College of Psychiatrists’ information page, and if you go to “What conditions can hypnotherapy help to treat”, you’ll see two broad categories; the first is almost entirely brain-stuff; the second is more varied, and includes pain relief of various kinds, burn care, cancer treatment side effects, and even menopause symptoms. Finally, warts and other various skin conditions get their own (positive) mention, per “this is possible through the positive effects hypnosis has on the immune system”:
RCPsych | Hypnosis And Hypnotherapy
Wondering how much psychosomatic effect can do?
You might like this previous article; it’s not about hypnotherapy, but it is about the difference the mind can make on physical markers of aging:
Aging, Counterclockwise: When Age Is A Flexible Number
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What Your Doctor Wants You to Know to Crush Medical Debt – by Dr. Virgie Ellington

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First things first: this one’s really only of relevance to people living in the US. That’s most of our readership, but if it’s not you, then apologies, this one won’t be of interest.
For the US Americans, though, Dr. Ellington starts strong with “you got a bill—now get the right bill”, and then gives a step-by-step process for finding the mistakes in your medical bills, fixing them, dealing with insurers who do not want to live up to their part of the bargain, and how to minimize what you need to pay, when you actually arrive at your final bill.
The biggest strength of this book is the wealth of insider knowledge (the author has worked as a primary care physician as well as as a health insurance executive), and while this information won’t stay current forever, its relatively recent publication date (2022) means that little has changed since then, and once you’re up to speed with how things are now, it’ll be easy to roll with whatever changes may come in the future.
Bottom line: if you’re living in the US and would like to not be ripped off as badly as possible when it comes to healthcare costs, this book is a very small, very powerful, investment.
Share This Post
-

Statins and Brain Fog?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝I was wondering if you had done any info about statins. I’ve tried 3, and keep quitting them because they give me brain fog. Am I imagining this as the research suggests?❞
If you are female, the chances of adverse side-effects are a lot higher:
As an extra kicker, not only are the adverse side-effects more likely for women, but also, the benefits are often less beneficial, too (see the above main feature for some details).
That’s not to say that statins can’t have their place for women; sometimes it will still be the right choice. Just, not as readily so as for men.
Enjoy!
Share This Post
-

Dyslexia Test
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
(and it’s mostly not about reading/writing!)
More than just shuffled letters
This video provides a self-test based on the Bangor Dyslexia Test (BDT). The BDT is 94% accurate in identifying dyslexia, and it includes 9 parts, with a mix of questions and tasks. Answering “yes” or struggling with tasks indicates possible dyslexia. Collecting 4+ indicators suggests dyslexia, but of course is not a replacement for official diagnosis.
It’s best to watch the video if you can, but here’s what to expect:
- Left-Right confusion: point your left hand to your right/left shoulder.
- Family history: any family members with dyslexia or struggles with reading/writing?
- Repeating numbers (order): repeat a given sequence of numbers in order.
- Letter confusion (e.g. b/d): do you confuse letters like “b” and “d” beyond age 8?
- Times tables: recite the 6, 7, and 8 times tables.
- Word manipulation: replace the letters in a word to create a new word, e.g. change “slide” (s ⇾ g) to “glide.”
- Repeating numbers (reversed): repeat a given sequence of numbers in reverse order.
- Months in reverse: recite the months of the year in reverse order.
- Subtraction: do you struggle with subtraction, e.g. 44-9 or 55-12?
Writer’s anecdote: I am not dyslexic, and/but I have an impressive level of dyscalculia (the purely numerical equivalent), to the point I’ll sometimes use a calculator to do single-digit calculations, and I am so bad at calculating ages or other differences between dates (I will have to count on my fingers or else run the severe risk of out-by-one errors). I have also been known to make mistakes counting down from 10, which really ruins dramatic tension.
In contrast, the left-right thing is interesting, because when I was first learning Arabic, I had no trouble reading/writing right-to-left, but I initially struggled so much to remember which way the “backspace” key would take me (in Arabic the backspace key backspaces to the right, despite still pointing to the left).
Anyway, for the test itself, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Reading, Better (Reading As A Cognitive Exercise)
Take care!
Share This Post
Related Posts
-

How to Read a Book – by Mortimer J. Adler and Charles Van Doren
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Are you a cover-to-cover person, or a dip-in-and-out person?
Mortimer Adler and Charles van Doren have made a science out of getting the most from reading books.
They help you find what you’re looking for (Maybe you want to find a better understanding of PCOS… maybe you want to find the definition of “heuristics”… maybe you want to find a new business strategy… maybe you want to find a romantic escape… maybe you want to find a deeper appreciation of 19th century poetry, maybe you want to find… etc).
They then help you retain what you read, and make sure that you don’t miss a trick.
Whether you read books so often that optimizing this is of huge value for you, or so rarely that when you do, you want to make it count, this book could make a real difference to your reading experience forever after.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What Actually Causes High Cholesterol?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In 1968, the American Heart Association advised limiting egg consumption to three per week due to cholesterol concerns linked to cardiovascular disease. Which was reasonable based on the evidence available back then, but it didn’t stand the test of time.
Eggs are indeed high in cholesterol, but that doesn’t mean that those who eat them will also be high in cholesterol, because…
It’s not quite what many people think
Some quite dietary pointers to start with:
- Egg yolks are high in cholesterol but have a minimal impact on blood cholesterol.
- Saturated and trans fats (as found in fatty meats or dairy, and some processed foods) have a greater influence on LDL levels than dietary cholesterol.
And on the other hand:
- Unsaturated fats (e.g. from fish, nuts, seeds) have anti-inflammatory benefits
- Fiber-rich foods help lower LDL by affecting fat absorption in the digestive tract
A quick primer on LDL and other kinds of cholesterol:
- VLDL (Very Low-Density Lipoprotein):
- delivers triglycerides and cholesterol to muscle and fat cells for energy
- is converted into LDL after delivery
- LDL (Low-Density Lipoprotein):
- is called “bad cholesterol”, which we call that due to its role in arterial plaque formation
- in excess leads to inflammation, overworked macrophage activity, and artery narrowing
- HDL (High-Density Lipoprotein):
- known as “good cholesterol,” picks up excess LDL and returns it to the liver for excretion
- is anti-inflammatory, in addition to regulating LDL levels
There are other factors too, for example:
- Smoking and drinking increase LDL buildup and cause oxidative damage to lipids in general and the blood vessels through which they travel
- Regular exercise, meanwhile, can lower LDL and raise HDL
- Statins and other medications can help lower LDL and manage cholesterol when lifestyle changes and genetics require additional support—but they often come with serious side effects, and the usefulness varies from person to person.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Science-Backed Anti-Inflammatory Diet for Beginners – by Dr. Yasmine Elamir & Dr. William Grist
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We have written about how to eat to beat inflammation, but what we didn’t do is include 75 recipes and a plan for building up one’s culinary repertoire around those core dishes!
That’s what this book does. It covers briefly the science of inflammation and anti-inflammatory diet, discusses experimental elimination diets (e.g. you eliminate likely culprits of triggering your inflammation, then reintroduce them one by one to see which it was), and ingredients likely to increase or decrease inflammation.
The 75 recipes are good, and/but a caveat is “yes, one of the recipes is ketchup and another is sour cream” so it’s not exactly 75 mains.
However! Where this book excels is in producing anti-inflammatory versions of commonly inflammatory dishes. That ketchup? Not sugary. The sour cream? Vegan. And so forth. We also see crispy roast potatoes, an array of desserts, and sections for popular holiday dishes too, so you will not need to be suddenly inflamed into the next dimension when it comes to festive eating.
The recipes are what the title claims them to be, “science-backed anti-inflammatory”, and that is clearly the main criterion for their inclusion. They are not by default vegan, vegetarian, dairy-free, nut-free, gluten-free, etc. For this reason, all recipes are marked with such tags as “V, VG, DF, GF, EF, NF” etc as applicable.
Bottom line: we’d consider this book more of a jumping-off point than a complete repertoire, but it’s a very good jumping-off point, and will definitely get you “up and running” (there’s a 21-day meal plan, for example).
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: