How to Stay Sane – by Philippa Perry
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, what this book is not: a guide of “how to stay sane” in the popular use of the word “sane”, meaning free from serious mental illness of all and any kinds in general, and especially free from psychotic delusions. Alas, this book will not help with those.
What, then, is it? A guide of “how to stay sane” in the more casual sense of resiliently and adaptively managing stress, anxiety, and suchlike. The “light end” of mental health struggles, that nonetheless may not always feel light when dealing with them.
The author, a psychotherapist, draws from her professional experience and training to lay out psychological tools for our use, as well as giving the reader a broader understanding of the most common ills that may ail us.
The writing style is relaxed and personable; it’s not at all like reading a textbook.
The psychotherapeutic style is not tied to one model, and rather hops from one to another, per what is most likely to help for a given thing. This is, in this reviewer’s opinion at least, far better than the (all-too common) attempt made by a lot of writers to try to present their personal favorite model as the cure for all ills, instead of embracing the whole toolbox as this one does.
Bottom line: if your mental health is anywhere between “mostly good” and “a little frayed around the edges but hanging on by at least a few threads”, then this book likely can help you gain/maintain the surer foundation you’re surely seeking.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Climate Change Threatens the Mental Well-Being of Youths. Here’s How To Help Them Cope.

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve all read the stories and seen the images: The life-threatening heat waves. The wildfires of unprecedented ferocity. The record-breaking storms washing away entire neighborhoods. The melting glaciers, the rising sea levels, the coastal flooding.
As California wildfires stretch into the colder months and hurricane survivors sort through the ruins left by floodwaters, let’s talk about an underreported victim of climate change: the emotional well-being of young people.
A nascent but growing body of research shows that a large proportion of adolescents and young adults, in the United States and abroad, feel anxious and worried about the impact of an unstable climate in their lives today and in the future.
Abby Rafeek, 14, is disquieted by the ravages of climate change, both near her home and far away. “It’s definitely affecting my life, because it’s causing stress thinking about the future and how, if we’re not addressing the problem now as a society, our planet is going to get worse,” says Abby, a high school student who lives in Gardena, California, a city of 58,000 about 15 miles south of downtown Los Angeles.
She says wildfires are a particular worry for her. “That’s closer to where I live, so it’s a bigger problem for me personally, and it also causes a lot of damage to the surrounding areas,” she says. “And also, the air gets messed up.”
In April, Abby took a survey on climate change for kids ages 12-17 during a visit to the emergency room at Children’s Hospital of Orange County.
Rammy Assaf, a pediatric emergency physician at the hospital, adapted the survey from one developed five years ago for adults. He administered his version last year to over 800 kids ages 12-17 and their caregivers. He says initial results show climate change is a serious cause of concern for the emotional security and well-being of young people.
Assaf has followed up with the kids to ask more open-ended questions, including whether they believe climate change will be solved in their lifetimes; how they feel when they read about extreme climate events; what they think about the future of the planet; and with whom they are able to discuss their concerns.
“When asked about their outlook for the future, the first words they will use are helpless, powerless, hopeless,” Assaf says. “These are very strong emotions.”
Assaf says he would like to see questions about climate change included in mental health screenings at pediatricians’ offices and in other settings where children get medical care. The American Academy of Pediatrics recommends that counseling on climate change be incorporated into the clinical practice of pediatricians and into medical school curriculums, but not with specific regard to mental health screening.
Assaf says anxiety about climate change intersects with the broader mental health crisis among youth, which has been marked by a rise in depression, loneliness, and suicide over the past decade, though there are recent signs it may be improving slightly.
A 2022 Harris Poll of 1,500 U.S. teenagers found that 89% of them regularly think about the environment, “with the majority feeling more worried than hopeful.” In addition, 69% said they feared they and their families would be affected by climate change in the near future. And 82% said they expected to have to make key life decisions — including where to live and whether to have children — based on the state of the environment.
And the impact is clearly not limited to the U.S. A 2021 survey of 10,000 16- to 25-year-olds across 10 countries found “59% were very or extremely worried and 84% were at least moderately worried” about climate change.
Susan Clayton, chair of the psychology department at the College of Wooster in Ohio, says climate change anxiety may be more pronounced among younger people than adults. “Older adults didn’t grow up being as aware of climate change or thinking about it very much, so there’s still a barrier to get over to accept it’s a real thing,” says Clayton, who co-created the adult climate change survey that Assaf adapted for younger people.
By contrast, “adolescents grew up with it as a real thing,” Clayton says. “Knowing you have the bulk of your life ahead of you gives you a very different view of what your life will be like.” She adds that younger people in particular feel betrayed by their government, which they don’t think is taking the problem seriously enough, and “this feeling of betrayal is associated with greater anxiety about the climate.”
Abby believes climate change is not being addressed with sufficient resolve. “I think if we figure out how to live on Mars and explore the deep sea, we could definitely figure out how to live here in a healthy environment,” she says.
If you are a parent whose children show signs of climate anxiety, you can help.
Louise Chawla, professor emerita in the environmental design program at the University of Colorado-Boulder, says the most important thing is to listen in an open-ended way. “Let there be space for kids to express their emotions. Just listen to them and let them know it’s safe to express these emotions,” says Chawla, who co-founded the nonprofit Growing Up Boulder, which works with the city’s schools to encourage kids to engage civically, including to help shape their local environment.
Chawla and others recommend family activities that reinforce a commitment to the environment. They can be as simple as walking or biking and participating in cleanup or recycling efforts. Also, encourage your children to join activities and advocacy efforts sponsored by environmental, civic, or religious organizations.
Working with others can help alleviate stress and feelings of powerlessness by reassuring kids they are not alone and that they can be proactive.
Worries about climate change should be seen as a learning opportunity that might even lead some kids to their life’s path, says Vickie Mays, professor of psychology and health policy at UCLA, who teaches a class on climate change and mental health — one of eight similar courses offered recently at UC campuses.
“We should get out of this habit of ‘everything’s a mental health problem,’” Mays says, “and understand that often a challenge, a stress, a worry can be turned into advocacy, activism, or a reach for new knowledge to change the situation.”
This article was produced by KFF Health News, which publishes California Healthline, an editorially independent service of the California Health Care Foundation.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Share This Post
-

How To Clean Your Brain (Glymphatic Health Primer)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
That’s not a typo! The name “glymphatic system” was coined by the Danish neuroscientist Dr. Maiken Nedergaard, and is a nod to its use of glial cells to do a similar job to that of the peripheral lymphatic system—but this time, in the CNS. Today, we have Dr. Jin Sung to tell us more:
Brainwashing (but not like that)
The glymphatic system may sound like a boring job, but so does “sanitation worker” in a city—yet the city would grind to a messy halt very very quickly without them. Same goes for your brain.
Diseases that are prevalent when this doesn’t happen the way it should include Alzheimer’s (beta-amyloid clearance) and Parkinson’s (alpha-synuclein clearance) amongst others.
Things Dr. Sung recommends for optimal glymphatic function include: sleep (7–9 hours), exercise (30–45 minutes daily), hydration (half your bodyweight in pounds, in ounces, so if your body weighs 150 lbs, that means 75 oz of water), good posture (including the use of good ergonomics, e.g. computer monitor at right height, car seat correct, etc), stress reduction (reduces inflammatory cytokines), getting enough omega-3 (the brain needs certain fats to work properly, and this is the one most likely to see a deficit), vagal stimulation (methods include humming, gargling, and gagging—please note we said vagal stimulation; easy to misread at a glance!), LED light therapy, and fasting (intermittent or prolonged).
For more on each of these, including specific tips, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Ask Not What Your Lymphatic System Can Do For You…
- The Vagus Nerve (And How You Can Make Use Of It)
- Casting Yourself In A Healthier Light
- Intermittent Fasting: How Does It Work?
Take care!
Share This Post
-

Black Cohosh vs The Menopause
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Black Cohosh, By Any Other Name…
Black cohosh is a flowering plant whose extracts are popularly used to relieve menopausal (and postmenopausal) symptoms.
Note on terms: we’ll use “black cohosh” in this article, but if you see the botanical names in studies, the reason it sometimes appears as Actaea racemosa and sometimes as Cimicfuga racemosa, is because it got changed and changed back on account of some disagreements between botanists. It’s the same plant, in any case!
Read: Reclassification of Actaea to include Cimicifuga and Souliea (Ranunculaceae)
Does it work?
In few words: it works for physical symptoms, but not emotional ones, based on this large (n=2,310) meta-analysis of studies:
❝Black cohosh extracts were associated with significant improvements in overall menopausal symptoms (Hedges’ g = 0.575, 95% CI = 0.283 to 0.867, P < 0.001), as well as in hot flashes (Hedges’ g = 0.315, 95% CIs = 0.107 to 0.524, P = 0.003), and somatic symptoms (Hedges’ g = 0.418, 95% CI = 0.165 to 0.670, P = 0.001), compared with placebo.
However, black cohosh did not significantly improve anxiety (Hedges’ g = 0.194, 95% CI = -0.296 to 0.684, P = 0.438) or depressive symptoms (Hedges’ g = 0.406, 95% CI = -0.121 to 0.932, P = 0.131)❞
~ Dr. Ryochi Sadahiro et al., 2023
Source: Black cohosh extracts in women with menopausal symptoms: an updated pairwise meta-analysis
Here’s an even larger (n=43,759) one that found similarly, and also noted on safety:
❝Treatment with iCR/iCR+HP was well tolerated with few minor adverse events, with a frequency comparable to placebo. The clinical data did not reveal any evidence of hepatotoxicity.
Hormone levels remained unchanged and estrogen-sensitive tissues (e.g. breast, endometrium) were unaffected by iCR treatment.
As benefits clearly outweigh risks, iCR/iCR+HP should be recommended as an evidence-based treatment option for natural climacteric symptoms.
With its good safety profile in general and at estrogen-sensitive organs, iCR as a non-hormonal herbal therapy can also be used in patients with hormone-dependent diseases who suffer from iatrogenic climacteric symptoms.❞
~ Dr. Castelo-Branco et al., 2020
(iCR = isopropanolic Cimicifuga racemosa)
So, is this estrogenic or not?
This is the question many scientists were asking, about 20 or so years ago. There are many papers from around 2000–2005, but here’s a good one that’s quite representative:
❝These new data dispute the estrogenic theory and demonstrate that extracts of black cohosh do not bind to the estrogen receptor in vitro, up-regulate estrogen-dependent genes, or stimulate the growth of estrogen-dependent tumors❞
Source: Is Black Cohosh Estrogenic?
(the abstract is a little vague, but if you click on the PDF icon, you can read the full paper, which is a lot clearer and more detailed)
The short answer: no, black cohosh is not estrogenic
Is it safe?
As ever, check with your doctor as everyone’s situation can vary, but broadly speaking, yes, it has a very good safety profile—including for breast cancer patients, at that. See for example:
- Black cohosh efficacy and safety for menopausal symptoms: the Spanish Menopause Society statement
- Black cohosh (Cimicifuga racemosa): safety and efficacy for cancer patients
- The safety of black cohosh (Actaea racemosa, Cimicifuga racemosa)
Where can I get some?
We don’t sell it, but here for your convenience is an example product on Amazon
Enjoy!
Share This Post
Related Posts
-

Generation M – by Dr. Jessica Shepherd
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Menopause is something that very few people are adequately prepared for despite its predictability, and also something that very many people then neglect to take seriously enough.
Dr. Shepherd encourages a more proactive approach throughout all stages of menopause and beyond; she discusses “the preseason, the main event, and the after-party” (perimenopause, menopause, and postmenopause), which is important, because typically people take up an interest in perimenopause, are treating it like a marathon by menopause, and when it comes to postmenopause, it’s easy to think “well, that’s behind me now”, and it’s not, because untreated menopause will continue to have (mostly deleterious) cumulative effects until death.
As for HRT, there’s a chapter on that of course, going into quite some detail. There is also plenty of attention given to popular concerns such as managing weight changes and libido changes, as well as oft-neglected topics such as brain changes, as well as things considered more cosmetic but that can have a big impact on mental health, such as skin and hair.
The style throughout is pop-science; friendly without skimping on detail and including plenty of good science.
Bottom line: if you’d like a fairly comprehensive overview of the changes that occur from perimenopause all the way to menopause and well beyond, then this is a great book for that.
Click here to check out Generation M, and live well at every stage of life!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What’s the difference between vegan and vegetarian?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
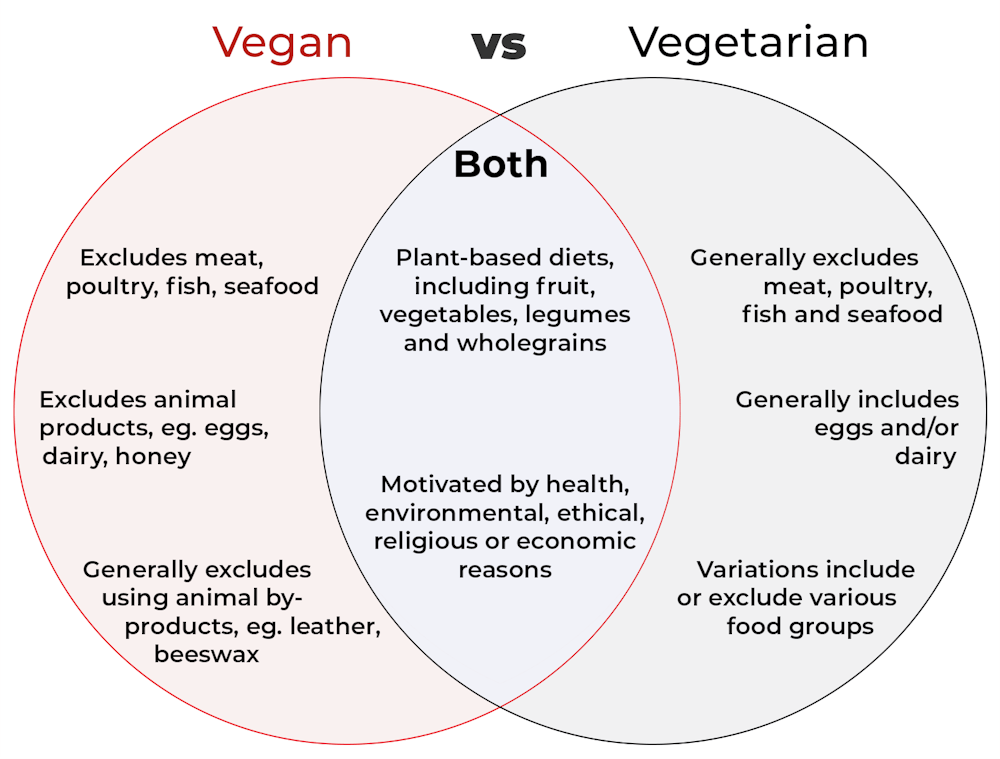
Vegan and vegetarian diets are plant-based diets. Both include plant foods, such as fruits, vegetables, legumes and whole grains.
But there are important differences, and knowing what you can and can’t eat when it comes to a vegan and vegetarian diet can be confusing.
So, what’s the main difference?

Creative Cat Studio/Shutterstock What’s a vegan diet?
A vegan diet is an entirely plant-based diet. It doesn’t include any meat and animal products. So, no meat, poultry, fish, seafood, eggs, dairy or honey.
What’s a vegetarian diet?
A vegetarian diet is a plant-based diet that generally excludes meat, poultry, fish and seafood, but can include animal products. So, unlike a vegan diet, a vegetarian diet can include eggs, dairy and honey.
But you may be wondering why you’ve heard of vegetarians who eat fish, vegetarians who don’t eat eggs, vegetarians who don’t eat dairy, and even vegetarians who eat some meat. Well, it’s because there are variations on a vegetarian diet:
- a lacto-ovo vegetarian diet excludes meat, poultry, fish and seafood, but includes eggs, dairy and honey
- an ovo-vegetarian diet excludes meat, poultry, fish, seafood and dairy, but includes eggs and honey
- a lacto-vegetarian diet excludes meat, poultry, fish, seafood and eggs, but includes dairy and honey
- a pescatarian diet excludes meat and poultry, but includes eggs, dairy, honey, fish and seafood
- a flexitarian, or semi-vegetarian diet, includes eggs, dairy and honey and may include small amounts of meat, poultry, fish and seafood.
Are these diets healthy?
A 2023 review looked at the health effects of vegetarian and vegan diets from two types of study.
Observational studies followed people over the years to see how their diets were linked to their health. In these studies, eating a vegetarian diet was associated with a lower risk of developing cardiovascular disease (such as heart disease or a stroke), diabetes, hypertension (high blood pressure), dementia and cancer.
For example, in a study of 44,561 participants, the risk of heart disease was 32% lower in vegetarians than non-vegetarians after an average follow-up of nearly 12 years.
Further evidence came from randomised controlled trials. These instruct study participants to eat a specific diet for a specific period of time and monitor their health throughout. These studies showed eating a vegetarian or vegan diet led to reductions in weight, blood pressure, and levels of unhealthy cholesterol.
For example, one analysis combined data from seven randomised controlled trials. This so-called meta-analysis included data from 311 participants. It showed eating a vegetarian diet was associated with a systolic blood pressure (the first number in your blood pressure reading) an average 5 mmHg lower compared with non-vegetarian diets.
It seems vegetarian diets are more likely to be healthier, across a number of measures.
For example, a 2022 meta-analysis combined the results of several observational studies. It concluded a vegetarian diet, rather than vegan diet, was recommended to prevent heart disease.
There is also evidence vegans are more likely to have bone fractures than vegetarians. This could be partly due to a lower body-mass index and a lower intake of nutrients such as calcium, vitamin D and protein.
But it can be about more than just food
Many vegans, where possible, do not use products that directly or indirectly involve using animals.
So vegans would not wear leather, wool or silk clothing, for example. And they would not use soaps or candles made from beeswax, or use products tested on animals.
The motivation for following a vegan or vegetarian diet can vary from person to person. Common motivations include health, environmental, ethical, religious or economic reasons.
And for many people who follow a vegan or vegetarian diet, this forms a central part of their identity.
More than a diet: veganism can form part of someone’s identity. Shutterstock So, should I adopt a vegan or vegetarian diet?
If you are thinking about a vegan or vegetarian diet, here are some things to consider:
- eating more plant foods does not automatically mean you are eating a healthier diet. Hot chips, biscuits and soft drinks can all be vegan or vegetarian foods. And many plant-based alternatives, such as plant-based sausages, can be high in added salt
- meeting the nutrient intake targets for vitamin B12, iron, calcium, and iodine requires more careful planning while on a vegan or vegetarian diet. This is because meat, seafood and animal products are good sources of these vitamins and minerals
- eating a plant-based diet doesn’t necessarily mean excluding all meat and animal products. A healthy flexitarian diet prioritises eating more whole plant-foods, such as vegetables and beans, and less processed meat, such as bacon and sausages
- the Australian Dietary Guidelines recommend eating a wide variety of foods from the five food groups (fruit, vegetables, cereals, lean meat and/or their alternatives and reduced-fat dairy products and/or their alternatives). So if you are eating animal products, choose lean, reduced-fat meats and dairy products and limit processed meats.
Katherine Livingstone, NHMRC Emerging Leadership Fellow and Senior Research Fellow at the Institute for Physical Activity and Nutrition, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Palliative care as a true art form
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How do you ease the pain from an ailment amidst lost words? How can you serve the afflicted when lines start to blur? When the foundation of communication begins to crumble, what will be the pillar health-care professionals can lean on to support patients afflicted with dementia during their final days?
The practice of medicine is both highly analytical and evidence based in nature. However, it is considered a “practice” because at the highest level, it resembles a musician navigating an instrument. It resembles art. Between lab values, imaging techniques and treatment options, the nuances for individualized patient care so often become threatened.
Dementia, a non-malignant terminal illness, involves the progressive cognitive and social decline in those afflicted. Though there is no cure, dementia is commonly met in the setting of end-of-life care. During this final stage of life, the importance of comfort via symptomatic management and communication usually is a priority in patient care. But what about the care of a patient suffering from dementia? While communication serves as the vehicle to deliver care at a high level, medical professionals are suddenly met with a roadblock. And there … behind the pieces of shattered communication and a dampened map of ethical guidelines, health-care providers are at a standstill.
It’s 4:37 a.m. You receive a text message from the overnight nurse at a care facility regarding a current seizure. After lorazepam is ordered and administered, Mr. H, a quick-witted 76-year-old, stabilizes. Phenobarbital 15mg SC qhs was also added to prevent future similar events. You exhale a sigh of relief.
Mr. H. has been admitted to the floor 36 hours earlier after having a seizure while playing poker with colleagues. Since he became your patient, he’s shared many stories from professional and family life with you, along with as many jokes as he could fit in between. However, over the course of the next seven days, Mr. H. would develop aspiration pneumonia, progressing to ventilator dependency and, ultimately, multi-organ failure with rapid cognitive decline.
What strategies and tools would you use to maximize the well-being of your patient during his decline? How would you bridge the gap of understanding between the patient’s family and health-care team to provide the standard of care that all patients are owed?
To give Mr. H. the type of care he would have wanted, upon his hospital admission, he should have been questioned about his understanding of illness along with the goals of care of the medical team. The patient should have been informed that it is imperative to adhere to the medical regimen implemented by his team along with the risks of not doing so. In the event disease-related complications arose, advanced directives should have been documented to avoid any unnecessary measures.
It is important to note, that with each change in status of the patient’s health status, the goal of treatment must be reassessed. The patient or surrogate decision-maker’s understanding of these goals is paramount in maintaining the patient’s autonomy. It is often said that effective communication is the bedrock of a healthy relationship. This is true regardless of type of relationship.
This is why I and Megan Vierhout wrote Integrated End of Life Care in Dementia: A Comprehensive Guide, a book targeted at providing a much-needed road map to navigate the many challenges involved in end-of-life care for individuals with dementia. Ultimately, our aim is to provide a compass for both health-care professionals and the families of those affected by the progressive effects of dementia. We provide practical advice on optimizing communication with individuals with dementia while taking their cognitive limitations, preferences and needs into account.
I invite you to explore the unpredictable terrain of end-of-life care for patients with dementia. Together, we can pave a smoother, sturdier path toward the practice of medicine as a true art form.
This article is republished from healthydebate under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: