How To Stand Up From The Floor Without Kneeling (3 Simple Methods)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Getting up off the ground without using your hands is an important skill and is considered very protective against some serious age-related woes. But, what if the body part you need to avoid putting pressure on is your knees? This can be important in the case of an injury, or arthritis, or a knee replacement, or any combination of the above.
With this in mind, Dr. Alyssa Kuhn, arthritis specialist, advises:
Take a stand
Depending on your circumstances and surroundings, you might have reason to choose one of these methods over the others, so we’ll present all three:
Method 1: Using a couch or chair for support
- Sit on the floor near a couch or chair.
- Bend the outside leg up as far as possible.
- If possible, tuck the other leg underneath you for added leverage.
- Place the hand closest to the support on the surface, and bring the other hand over as well.
- Push through your bent leg and both arms to lift yourself up into a sitting or standing position on the surface.
Method 2: Modified plank roll
- Sit with your legs in front of you.
- Bend the outside leg (opposite the direction you’ll roll).
- Reach across your body with your arm and roll onto your hands into a modified plank or all-fours position.
- Walk your feet closer in or use your hands to walk up your legs.
- Gradually push yourself up to standing.
Method 3: Double knee bend with rotation
- Bend both knees as much as you comfortably can*
- Reach across your body with one arm and rotate your torso in that direction.
- Use your arms and feet to help spin and shift into a standing position.
- Shuffle your feet and stand up fully.
*if one or more of your knees won’t bend meaningfully, then this third method is just not for you
For more on each of these, plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
4 Tips To Stand Without Using Hands
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Art and Science of Connection – by Kasley Killam, MPH

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We can eat well, exercise well, and even sleep well, and we’ll still have a +53% increased all-cause mortality if we lack social connection—even if we technically have support and access to social resources, just not the real human connection itself. And as we get older, it gets increasingly easy to find ourselves isolated.
The author is a social scientist by profession, and it shows. None of what she shares in the book is wishy-washy; it has abundant scientific references coming thick and fast, and a great deal of clarity with regard to terms, something often not found in books of this genre that lean more towards the art than the science.
On which note, for the reader who may be thinking “I am indeed quite alone”, she also offers proven techniques for remedying that; not in the way that many books use the word “proven” to mean “we got some testimonials”, but rather, proven in the sense of “we did science to it and based on these 17 large population-based retrospective cohort studies, we can say with 99% confidence that this is an effective tool to mediate improved social bonds and social health outcomes”.
To this end, it’s a very practical book also, and should bestow upon any isolated reader a sense of confidence that in fact, things can be better. A particular strength is that it also looks at many different scenarios, so for the “what if I…” people with clear reasons why social connection is not abundantly available, yes, she has such cases covered too.
Bottom line: if you’d like to live more healthily for longer, social health is an underrated and oft-forgotten way of greatly increasing those things, by science.
Click here to check out The Art And Science Of Social Connection, and get connected!
Share This Post
-

Never Too Old?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Age Limits On Exercise?
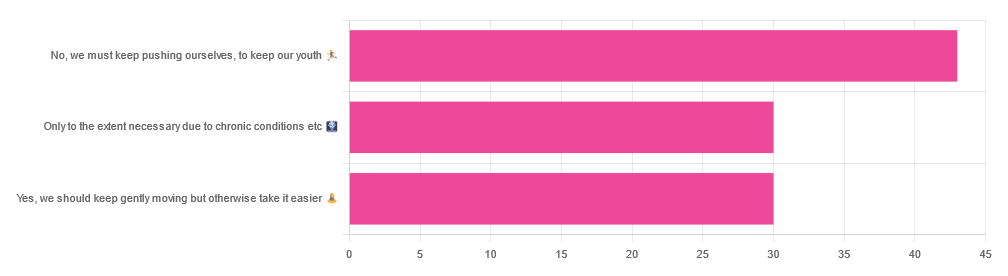
In Tuesday’s newsletter, we asked you your opinion on whether we should exercise less as we get older, and got the above-depicted, below-described, set of responses:

- About 42% said “No, we must keep pushing ourselves, to keep our youth“
- About 29% said “Only to the extent necessary due to chronic conditions etc”
- About 29% said “Yes, we should keep gently moving but otherwise take it easier”
One subscriber who voted for “No, we must keep pushing ourselves, to keep our youth“ wrote to add:
❝I’m 71 and I push myself. I’m not as fast or strong as I used to be but, I feel great when I push myself instead of going through the motions. I listen to my body!❞
~ 10almonds subscriber
One subscriber who voted for “Only to the extent necessary due to chronic conditions etc” wrote to add:
❝It’s never too late to get stronger. Important to keep your strength and balance. I am a Silver Sneakers instructor and I see first hand how helpful regular exercise is for seniors.❞
~ 10almonds subscriber
One subscriber who voted to say “Yes, we should keep gently moving but otherwise take it easier” wrote to add:
❝Keep moving but be considerate and respectful of your aging body. It’s a time to find balance in life and not put yourself into a positon to damage youself by competing with decades younger folks (unless you want to) – it will take much longer to bounce back.❞
~ 10almonds subscriber
These will be important, because we’ll come back to them at the end.
So what does the science say?
Endurance exercise is for young people only: True or False?
False! With proper training, age is no barrier to serious endurance exercise.
Here’s a study that looked at marathon-runners of various ages, and found that…
- the majority of middle-aged and elderly athletes have training histories of less than seven years of running
- there are virtually no relevant running time differences (p<0.01) per age in marathon finishers from 20 to 55 years
- after 55 years, running times did increase on average, but not consistently (i.e. there were still older runners with comparable times to the younger age bracket)
The researchers took this as evidence of aging being indeed a biological process that can be sped up or slowed down by various lifestyle factors.
See also:
Age & Aging: What Can (And Can’t) We Do About It?
this covers the many aspects of biological aging (it’s not one number, but many!) and how our various different biological ages are often not in sync with each other, and how we can optimize each of them that can be optimized
Resistance training is for young people only: True or False?
False! In fact, it’s not only possible for older people, but is also associated with a reduction in all-cause mortality.
Specifically, those who reported strength-training at least once per week enjoyed longer lives than those who did not.
You may be thinking “is this just the horse-riding thing again, where correlation is not causation and it’s just that healthier people (for other reasons) were able to do strength-training more, rather than the other way around?“
…which is a good think to think of, so well-spotted if you were thinking that!
But in this case no; the benefits remained when other things were controlled for:
❝Adjusted for demographic variables, health behaviors and health conditions, a statistically significant effect on mortality remained.
Although the effects on cardiac and cancer mortality were no longer statistically significant, the data still pointed to a benefit.
Importantly, after the physical activity level was controlled for, people who reported strength exercises appeared to see a greater mortality benefit than those who reported physical activity alone.❞
See the study: Is strength training associated with mortality benefits? A 15 year cohort study of US older adults
And a pop-sci article about it: Strength training helps older adults live longer
Closing thoughts
As it happens… All three of the subscribers we quoted all had excellent points!
Because in this case it’s less a matter of “should”, and more a selection of options:
- We (most of us, at least) can gain/regain/maintain the kind of strength and fitness associated with much younger people, and we need not be afraid of exercising accordingly (assuming having worked up to such, not just going straight from couch to marathon, say).
- We must nevertheless be mindful of chronic conditions or even passing illnesses/injuries, but that goes for people of any age
- We also can’t argue against a “safety first” cautious approach to exercise. After all, sure, maybe we can run marathons at any age, but that doesn’t mean we have to. And sure, maybe we can train to lift heavy weights, but if we’re content to be able to carry the groceries or perhaps take our partner’s weight in the dance hall (or the bedroom!), then (if we’re also at least maintaining our bones and muscles at a healthy level) that’s good enough already.
Which prompts the question, what do you want to be able to do, now and years from now? What’s important to you?
For inspiration, check out: Train For The Event Of Your Life!
Take care!
Share This Post
-

Beetroot vs Tomato – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing beetroot to tomato, we picked the beetroot.
Why?
Both are great! But we say beetroot comes out on top:
In terms of macros, beetroot has more protein, carbs, and fiber, making it the more nutritionally dense option. It has a slightly higher glycemic index, but also has specific phytochemicals that lower blood sugars and increase insulin sensitivity, more than cancelling that out. So, a clear win for beetroot in this regard.
In the category of vitamins, beetroot has more of vitamins B2, B5, B7, and B9, while tomato has more of vitamins A, C, E, and K. We’d call that a 4:4 tie, but tomato’s margins of difference are greater, so we say tomato wins this round.
When it comes to minerals, beetroot has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while tomatoes are not higher in any mineral. An easy win for beetroot here.
Looking at polyphenols and other remaining phytochemicals, beetroot has most, and especially its betalain content goes a long way. Tomatoes, meanwhile, have a famously high lycopene content (a highly beneficial carotenoid). All in all, it could swing either way based on subjective factors, so we’re saying it’s a tie this time.
Adding up the sections makes for an overall win for beetroot, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
- Beetroot For More Than Just Your Blood Pressure
- Lycopene’s Benefits For The Gut, Heart, Brain, & More
Enjoy!
Share This Post
Related Posts
-
Raspberries vs Starfruit – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing raspberries to starfruit, we picked the raspberries.
Why?
It’s quite a straightforward one today:
In terms of macros, raspberries have more than 2x the fiber, as well as slightly more carbs, and for what it’s worth which isn’t much because the numbers are truly tiny for this one, slightly more protein. In any case, an easy win for raspberries mainly by virtue of the fiber.
In the category of vitamins, raspberries have more of vitamins B1, B2, B3, B6, B7, B9, E, and K, while starfruit has more of vitamins A, B5, and C, yielding an 8:1 win for raspberries in this second round.
Looking at minerals next, raspberries have more calcium, iron, magnesium, manganese, phosphorus, potassium, and zinc, while starfruit has more calcium and selenium, meaning it’s a tidy 7:2 win for raspberries here.
In other considerations, raspberries are much higher in polyphenols, so that’s another point in their favor.
Adding up the sections makes for an overwhelming overall win for raspberries, but by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like:
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Art and music therapies can be ‘life changing’ for people with disability
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
From November, music and art therapists will be able to charge the National Disability Insurance Scheme (NDIS) the same as counsellors, after an independent review found they can be effective and “even life changing” for some people with disability.
The National Disability Insurance Agency commissioned the review, led by health economist Stephen Duckett, after widespread criticism of pricing changes it announced last year.
In November last year, the federal government announced it would slash the maximum therapists could bill per hour from A$193.99 to $67.56, citing insufficient evidence they were effective.
This week, the National Disability Insurance Agency (NDIA) has accepted the Duckett Review’s 19 recommendations, and the finding these therapies are effective and beneficial for people with specific conditions and disabilities.
Here’s what we know, and what will change.
Halfpoint/Getty What’s changing
Art and music therapies will be restored to the “therapy supports” funding category, following last year’s unexpected announcement they would be restricted to the “community participation” category.
These NDIS funding categories are different in two important ways.
The first relates to the maximum hourly rate for an individual session. Therapy supports can cost a maximum of $193.99 an hour. In contrast, “community participation” costs are capped at $67.56 an hour.
The review recommended a new hourly rate of $156.16 for individual art and music therapy sessions – the same hourly rate as counselling. However this remains significantly lower than other allied health services with similar levels of training, such as occupational therapy.
The second difference is that therapy services and community participation programs have very different requirements for providing evidence they are beneficial, and for providers’ qualifications levels and training.
The review also recommended a clearer distinction between art and music as a therapeutic support, and art and music as an activity.
And it recommended these therapies should be delivered by a qualified and registered music or art therapist.
So, what’s the difference?
As a music therapy researcher, I am often asked to explain the difference between “music therapy” and “music activity”.
People can be confused because music activities might also make us feel good. For example, music activities such as singing in a community choir can have mental health benefits for adults. Learning to play the ukulele has been shown to build stronger empathic skills in children.
Music activities like these are valuable for many people, but they are not music therapy.
Music therapy practice is informed by research into the benefits of specific methods and techniques for people with disability. These include autistic children, people with profound disabilities, and people recovering from major injury.
For example, if a client is non-speaking, the therapist might use a vocal improvisation technique, creating supportive music to encourage the person to make sounds with their voice. The back-and-forth musical dialogue at first doesn’t rely on words. But the therapist may help the client extend to more expressive vocalisations and even word production.
In Australia, music therapists must complete a two-year master’s degree before they are able to register with the Australian Music Therapy Association, and engage in continuous professional development.
The review said artists or musicians who do not have relevant qualifications to register with their professional bodies should not charge the new hourly rate for therapy.
So, what does the evidence say?
The new review acknowledged that establishing the evidence for therapy and disability is a complex task.
Around one in five Australians live with disability. Each person has unique needs and strengths, and disability occurs across the lifespan, meaning needs can also change. But when studying whether a particular kind of therapy is beneficial, researchers will focus on a particular group of people, such as adults with cerebral palsy.
This means the quantity and quality of evidence available will vary across different age groups and conditions – and there may be gaps. So care needs to be taken when interpreting the research to consider whether findings from one study might be applicable to other people with similar goals, needs, or conditions.
Qualified therapists are trained to interpret this evidence. They may be working with a client whose condition or needs differ from what’s in the existing research literature. So, they will consider whether a study showing benefits for music therapy with one group (such as non-speaking autistic children) could be relevant to another (for example, other people who have limitations in verbal expression).
The Duckett Review acknowledges this challenge of generalising evidence across different therapies. But it also warns of possible discrimination against people with rare conditions that attract limited research funding, and calls for more research.
Grace Thompson, Associate Professor in Music Therapy; Senior Academic Fellow at Melbourne Centre for the Study of Higher Education, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

At The Heart Of Women’s Health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A woman’s heart is a particular thing
For the longest time (and still to a large degree now), “women’s health” is assumed to refer to the health of organs found under a bikini. But there’s a lot more to it than that. We are whole people, with such things as brains and hearts and more.
Today (Valentine’s Day!) we’re focusing on the heart.
A quick recap:
We’ve talked previously about some of these sex differences when it comes to the heart, for example:
Heart Attack: His & Hers (Be Prepared!)
…but that’s fairly common knowledge at least amongst those who are attentive to such things, whereas…
…is much less common knowledge, especially with the ways statins are more likely to make things worse for a lot of women (not all though; see the article for some nuance about that).
We also talked about:
What Menopause Does To The Heart
…which is well worth reading too!
A question:
Why are women twice as likely to die from a heart attack as their age-equivalent male peers? Women develop heart disease later, but die from it sooner. Why is that?
That’s been a question scientists have been asking (and tentatively answering, as scientists do—hypotheses, theories, conclusions even sometimes) for 20 years now. Likely contributing factors include:
- A lack of public knowledge of the different symptoms
- A lack of confidence of bystanders to perform CPR on a woman
- A lack of public knowledge (including amongst prescribers) about the sex-related differences for statins
- A lack of women in cardiology, comparatively.
- A lack of attention to it, simply. Men get heart disease earlier, so it’s thought of as a “man thing”, by health providers as much as by individuals. Men get more regular cardiovascular check-ups, women get a mammogram and go.
Statistically, women are much more likely to die from heart disease than breast cancer:
- Breast cancer kills around 0.02% of us.
- Heart disease kills one in three.
And yet…
❝In a nationwide survey, only 22% of primary care doctors and 42% of cardiologists said they feel extremely well prepared to assess cardiovascular risks in women.
We are lagging in implementing risk prevention guidelines for women.
A lot of women are being told to just watch their cholesterol levels and see their doctor in a year. That’s a year of delayed care.❞
Source: The slowly evolving truth about heart disease and women
(there’s a lot more in that article than we have room for in ours, so do check it out!)
Some good news:
The “bystanders less likely to feel confident performing CPR on a woman” aspect may be helped by the deployment of new automatic external defibrillator, that works from four sides instead of one.
It’s called “double sequential external defibrillation”, and you can learn about it here:
A new emergency procedure for cardiac arrests aims to save more lives—here’s how it works
(it’s in use already in Canada and Aotearoa)
Gentlemen-readers, thank you for your attention to this one even if it was mostly not about you! Maybe someone you love will benefit from being aware of this
On a lighter note…
Since it’s Valentine’s Day, a little more on affairs of the heart…
Is chocolate good for the heart? And is it really an aphrodisiac?
We answered these questions and more in our previous main feature:
Chocolate & Health: Fact or Fiction?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: