

How To Look After Your Health When Your Life Falls Apart
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Ruth Machin of “Wise Woman Wellbeing” is here with advice from recent experience:
Holding it together
For Dr. Machin, grief after her father’s death understandably disrupted her previously consistent habits like regular exercise, healthy eating, and 7–8 hours of sleep, leading to poor sleep, reduced appetite, increased cravings, and less movement.
These sorts of things tend to unravel together, because stress and poor sleep raise cortisol and adrenaline levels, increase the hunger hormone ghrelin, and impair decision-making, which in turn drives cravings for high-fat, sugar, and salty foods, thus causing multiple habits to collapse in a chain reaction.
In other words, these habit lapses don’t happen in isolation, but rather stack on top of each other, making it harder to restart, and turning a short disruption into a prolonged break from routines.
- What to not do: the all-or-nothing approach fails because waiting for the “right time” delays action indefinitely, while going all-in sets unrealistic standards that lead to overwhelm and burnout.
- What to do instead: adopting a “minimum viable routine” reframes health as part of your identity by maintaining small, consistent actions even during difficult periods.
The core principle here is that consistency matters more than perfection, especially during challenging times when maintaining anything is more valuable than aiming for ideal habits and ending up crashing and burning instead.
So, she recommends to identify the smallest reasonably possible set of daily actions that support your physical and mental health, and keep them going regardless of circumstances.
This is critical, because maintaining even minimal habits during hard times prevents complete resets, making it easier to return to fuller routines when life stabilizes.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
- How To Keep On Keeping On
- How To Bounce Back After A Setback
- What Grief Does To Your Body (And How To Manage It)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Voluntary assisted dying is different to suicide. But federal laws conflate them and restrict access to telehealth

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Voluntary assisted dying is now lawful in every Australian state and will soon begin in the Australian Capital Territory.
However, it’s illegal to discuss it via telehealth. That means people who live in rural and remote areas, or those who can’t physically go to see a doctor, may not be able to access the scheme.
A federal private members bill, introduced to parliament last week, aims to change this. So what’s proposed and why is it needed?
What’s wrong with the current laws?
Voluntary assisted dying doesn’t meet the definition of suicide under state laws.
But the Commonwealth Criminal Code prohibits the discussion or dissemination of suicide-related material electronically.
This opens doctors to the risk of criminal prosecution if they discuss voluntary assisted dying via telehealth.
Successive Commonwealth attorneys-general have failed to address the conflict between federal and state laws, despite persistent calls from state attorneys-general for necessary clarity.
This eventually led to voluntary assistant dying doctor Nicholas Carr calling on the Federal Court of Australia to resolve this conflict. Carr sought a declaration to exclude voluntary assisted dying from the definition of suicide under the Criminal Code.
In November, the court declared voluntary assisted dying was considered suicide for the purpose of the Criminal Code. This meant doctors across Australia were prohibited from using telehealth services for voluntary assisted dying consultations.
Last week, independent federal MP Kate Chaney introduced a private members bill to create an exemption for voluntary assisted dying by excluding it as suicide for the purpose of the Criminal Code. Here’s why it’s needed.
Not all patients can physically see a doctor
Defining voluntary assisted dying as suicide in the Criminal Code disproportionately impacts people living in regional and remote areas. People in the country rely on the use of “carriage services”, such as phone and video consultations, to avoid travelling long distances to consult their doctor.
Other people with terminal illnesses, whether in regional or urban areas, may be suffering intolerably and unable to physically attend appointments with doctors.
The prohibition against telehealth goes against the principles of voluntary assisted dying, which are to minimise suffering, maximise quality of life and promote autonomy.

Some people aren’t able to attend doctors’ appointments in person.
Jeffrey M Levine/ShutterstockDoctors don’t want to be involved in ‘suicide’
Equating voluntary assisted dying with suicide has a direct impact on doctors, who fear criminal prosecution due to the prohibition against using telehealth.
Some doctors may decide not to help patients who choose voluntary assisted dying, leaving patients in a state of limbo.
The number of doctors actively participating in voluntary assisted dying is already low. The majority of doctors are located in metropolitan areas or major regional centres, leaving some locations with very few doctors participating in voluntary assisted dying.
It misclassifies deaths
In state law, people dying under voluntary assisted dying have the cause of their death registered as “the disease, illness or medical condition that was the grounds for a person to access voluntary assisted dying”, while the manner of dying is recorded as voluntary assisted dying.
In contrast, only coroners in each state and territory can make a finding of suicide as a cause of death.
In 2017, voluntary assisted dying was defined in the Coroners Act 2008 (Vic) as not a reportable death, and thus not suicide.
The language of suicide is inappropriate for explaining how people make a decision to die with dignity under the lawful practice of voluntary assisted dying.
There is ongoing taboo and stigma attached to suicide. People who opt for and are lawfully eligible to access voluntary assisted dying should not be tainted with the taboo that currently surrounds suicide.
So what is the solution?
The only way to remedy this problem is for the federal government to create an exemption in the Criminal Code to allow telehealth appointments to discuss voluntary assisted dying.
Chaney’s private member’s bill is yet to be debated in federal parliament.
If it’s unsuccessful, the Commonwealth attorney-general should pass regulations to exempt voluntary assisted dying as suicide.
A cooperative approach to resolve this conflict of laws is necessary to ensure doctors don’t risk prosecution for assisting eligible people to access voluntary assisted dying, regional and remote patients have access to voluntary assisted dying, families don’t suffer consequences for the erroneous classification of voluntary assisted dying as suicide, and people accessing voluntary assisted dying are not shrouded with the taboo of suicide when accessing a lawful practice to die with dignity.
Failure to change this will cause unnecessary suffering for patients and doctors alike.

Michaela Estelle Okninski, Lecturer of Law, University of Adelaide; Marc Trabsky, Associate professor, La Trobe University, and Neera Bhatia, Associate Professor in Law, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

How safe are the chemicals in sunscreen? A pharmacology expert explains
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Last week, the Therapeutic Goods Administration (TGA) released its safety review of seven active ingredients commonly used in sunscreens.
It found five were low-risk and appropriate for use in sunscreens at their current concentrations.
However, the TGA recommended tighter restrictions on two ingredients – homosalate and oxybenzone – to reduce how much can be used in a product. This is based on uncertainty about their potential effects on the endocrine system, which creates and releases hormones.
This news, together with recent reports some products may have inflated their claims of SPF coverage, might make Australians worried about whether their sunscreen products are working – and safe.
But it’s not time to abandon sunscreens. In Australia, all sunscreens must pass a strict approval process before going on the market. The TGA tests the safety and efficacy of all ingredients, and this recent review is part of the TGA’s continuing commitment to safety.
The greatest threat sunscreen poses to Australians’ health is not using it.
Australia has the highest incidence of melanoma and non-melanoma skin cancer worldwide, and approximately 95% of melanoma cases in Australia are linked to ultraviolet (UV) exposure.
Still, it’s understandable people want to know what’s in their products, and any changes that might affect them. So let’s take a closer look at the safety review and what it found.
aquaArts studio/Getty What are the active ingredients in sunscreen?
There are two main types of sunscreen: physical and chemical. This is based on the different active ingredients they use.
An active ingredient is a chemical component in a product that has an effect on the body – basically, what makes the product “work”.
In sunscreens, this is the compound that absorbs UV rays from the Sun. The other ingredients – for example, those that give the sunscreen its smell or help the skin absorb it – are “inactive”.
Physical sunscreens typically use minerals, such as titanium dioxide and zinc oxide, that can absorb the Sun’s rays but also reflect some of them.
Chemical sunscreens use a variety of chemical ingredients to absorb or scatter UV light, both long wave (UVA) or short wave (UVB).
The seven active ingredients in this review are in chemical sunscreens.
Why did the TGA do the review?
Our current limits for the concentrations of these chemicals in sunscreen are generally consistent with other regulatory agencies, such as the European Union and the US Food and Drug Administration.
However, safety is an evolving subject. The TGA periodically reexamines the safety of all therapeutic goods.
Last year, the TGA revised its method of estimating sunscreen exposure to more closely model how skin is exposed to sunscreens over time.
This model considers how much sunscreen someone typically applies, how much skin they cover (whole body versus face and hands, or just face) and how it’s absorbed through the skin.
Given this new model – along with changes in the EU and US approaches to sunscreen regulation – the TGA selected seven common sunscreen ingredients to investigate in depth.
Determining what’s safe
When evaluating whether chemicals are safe for human use, testing will often consider studies in animals – especially when there is no or limited data on humans. These animal tests are done by the manufacturers, not the TGA.
To take into account any unforeseen sensitivity humans may have to these chemicals, a “margin of safety” is built in. This is typically a concentration 50–100 times lower than the dose at which no negative effect was seen in animals.
The sunscreen review used a margin of safety 100 times lower than this dose as the safety threshold.
For most of the seven investigated sunscreen chemicals, the TGA found the margin of safety was above 100.
This means they’re considered safe and low-risk for long-term use.
However, two ingredients, homosalate and oxybenzone, were found to be below 100. This was based on the highest estimated sunscreen exposure, applied to the body at the maximum permitted concentration: 15% for homosalate, 10% for oxybenzone.
At lower concentrations, other uses – such as just the hands and face – could be considered low-risk for both ingredients.
What are the health concerns?
Homosalate and oxybenzone have low acute oral toxicity – meaning you would need to swallow a lot of it to experience toxic effects, nearly half a kilogram of these chemicals – and don’t cause irritation to eyes or skin.
There is inconclusive evidence about oxybenzone potentially causing cancer in rats and mice – but only at concentrations to which humans will never be exposed via sunscreens.
The key issue is whether the two ingredients affect the endocrine system.
While effects have been seen at high concentrations in animal studies, it is not clear whether these translate to humans exposed to sunscreen levels.
No effect has been seen in clinical studies on fertility, hormones, weight gain and, in pregnant women, fetal development.
The TGA is being very cautious here, using a very wide margin of safety under worst-case scenarios.
What are the recommendations?
The TGA recommends the allowed concentration of homosalate and oxybenzone be reduced.
But exactly how much it will be lowered is complicated, depending on whether the product is intended for adults or children, specifically for face, or the whole body, and so on.
However, some sunscreens would need to be reformulated or warning labels placed on particular formulations. The exact changes will be decided after public consultation. Submissions close on August 12.
What about benzophenone?
There is also some evidence benzophenone – a chemical produced when sunscreen that contains octocrylene degrades – may cause cancer at high concentrations.
This is based on studies in which mice and rats were fed benzophenone well above the concentration in sunscreens.
Octocrylene degrades slowly over time to benzophenone. Heat makes it degrade faster, especially at temperatures above 40°C.
The TGA has recommended restricting benzophenone to 0.0383% in sunscreens to ensure it remains safe during the product’s shelf life.
The Cancer Council advises storing sunscreens below 30°C.
The bottom line
The proposed restrictions are very conservative, based on worst-case scenarios.
But even in worst-case scenarios, the margin of safety for these ingredients is still below the level at which any negative effect was seen in animals.
The threat of cancer from sun exposure is far more serious than any potential negative effect from sunscreens.
If you do wish to avoid these chemicals before new limits are imposed, several sunscreens are available that provide high levels of protection with little or no homosalate and oxybenzone. For more information, consult product labels.
Ian Musgrave, Senior Lecturer in Pharmacology, University of Adelaide
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

What’s the difference between vegan and vegetarian?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
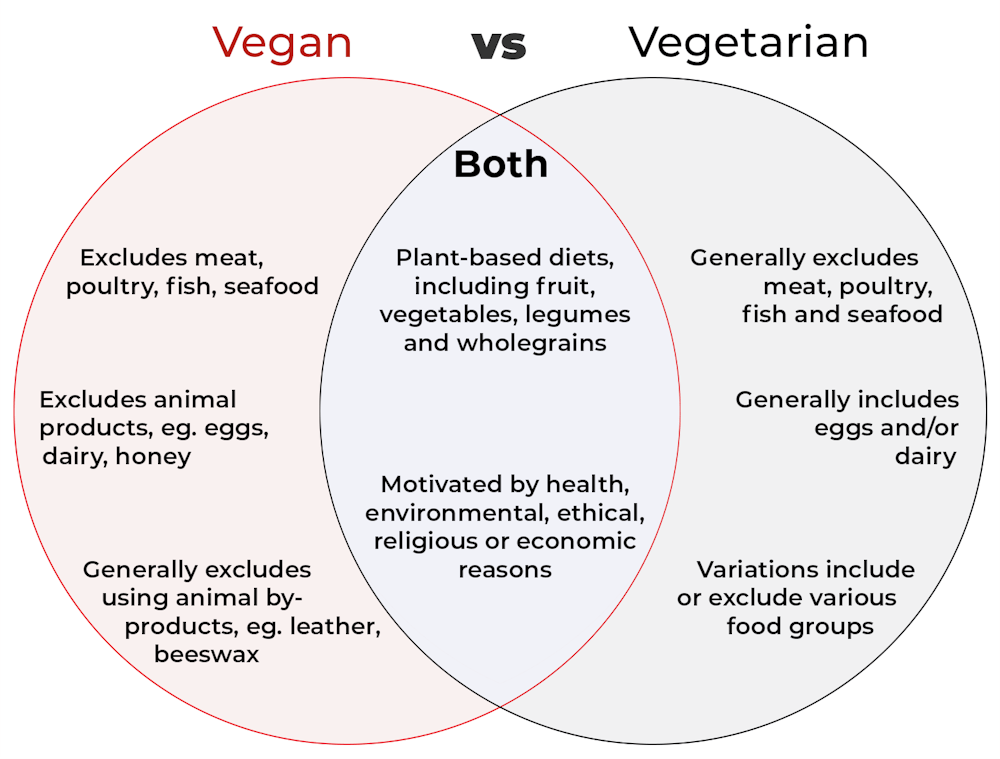
Vegan and vegetarian diets are plant-based diets. Both include plant foods, such as fruits, vegetables, legumes and whole grains.
But there are important differences, and knowing what you can and can’t eat when it comes to a vegan and vegetarian diet can be confusing.
So, what’s the main difference?
Creative Cat Studio/Shutterstock What’s a vegan diet?
A vegan diet is an entirely plant-based diet. It doesn’t include any meat and animal products. So, no meat, poultry, fish, seafood, eggs, dairy or honey.
What’s a vegetarian diet?
A vegetarian diet is a plant-based diet that generally excludes meat, poultry, fish and seafood, but can include animal products. So, unlike a vegan diet, a vegetarian diet can include eggs, dairy and honey.
But you may be wondering why you’ve heard of vegetarians who eat fish, vegetarians who don’t eat eggs, vegetarians who don’t eat dairy, and even vegetarians who eat some meat. Well, it’s because there are variations on a vegetarian diet:
- a lacto-ovo vegetarian diet excludes meat, poultry, fish and seafood, but includes eggs, dairy and honey
- an ovo-vegetarian diet excludes meat, poultry, fish, seafood and dairy, but includes eggs and honey
- a lacto-vegetarian diet excludes meat, poultry, fish, seafood and eggs, but includes dairy and honey
- a pescatarian diet excludes meat and poultry, but includes eggs, dairy, honey, fish and seafood
- a flexitarian, or semi-vegetarian diet, includes eggs, dairy and honey and may include small amounts of meat, poultry, fish and seafood.
Are these diets healthy?
A 2023 review looked at the health effects of vegetarian and vegan diets from two types of study.
Observational studies followed people over the years to see how their diets were linked to their health. In these studies, eating a vegetarian diet was associated with a lower risk of developing cardiovascular disease (such as heart disease or a stroke), diabetes, hypertension (high blood pressure), dementia and cancer.
For example, in a study of 44,561 participants, the risk of heart disease was 32% lower in vegetarians than non-vegetarians after an average follow-up of nearly 12 years.
Further evidence came from randomised controlled trials. These instruct study participants to eat a specific diet for a specific period of time and monitor their health throughout. These studies showed eating a vegetarian or vegan diet led to reductions in weight, blood pressure, and levels of unhealthy cholesterol.
For example, one analysis combined data from seven randomised controlled trials. This so-called meta-analysis included data from 311 participants. It showed eating a vegetarian diet was associated with a systolic blood pressure (the first number in your blood pressure reading) an average 5 mmHg lower compared with non-vegetarian diets.
It seems vegetarian diets are more likely to be healthier, across a number of measures.
For example, a 2022 meta-analysis combined the results of several observational studies. It concluded a vegetarian diet, rather than vegan diet, was recommended to prevent heart disease.
There is also evidence vegans are more likely to have bone fractures than vegetarians. This could be partly due to a lower body-mass index and a lower intake of nutrients such as calcium, vitamin D and protein.
But it can be about more than just food
Many vegans, where possible, do not use products that directly or indirectly involve using animals.
So vegans would not wear leather, wool or silk clothing, for example. And they would not use soaps or candles made from beeswax, or use products tested on animals.
The motivation for following a vegan or vegetarian diet can vary from person to person. Common motivations include health, environmental, ethical, religious or economic reasons.
And for many people who follow a vegan or vegetarian diet, this forms a central part of their identity.
More than a diet: veganism can form part of someone’s identity. Shutterstock So, should I adopt a vegan or vegetarian diet?
If you are thinking about a vegan or vegetarian diet, here are some things to consider:
- eating more plant foods does not automatically mean you are eating a healthier diet. Hot chips, biscuits and soft drinks can all be vegan or vegetarian foods. And many plant-based alternatives, such as plant-based sausages, can be high in added salt
- meeting the nutrient intake targets for vitamin B12, iron, calcium, and iodine requires more careful planning while on a vegan or vegetarian diet. This is because meat, seafood and animal products are good sources of these vitamins and minerals
- eating a plant-based diet doesn’t necessarily mean excluding all meat and animal products. A healthy flexitarian diet prioritises eating more whole plant-foods, such as vegetables and beans, and less processed meat, such as bacon and sausages
- the Australian Dietary Guidelines recommend eating a wide variety of foods from the five food groups (fruit, vegetables, cereals, lean meat and/or their alternatives and reduced-fat dairy products and/or their alternatives). So if you are eating animal products, choose lean, reduced-fat meats and dairy products and limit processed meats.
Katherine Livingstone, NHMRC Emerging Leadership Fellow and Senior Research Fellow at the Institute for Physical Activity and Nutrition, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post






Related Posts
-

5 Steps To Quit Sugar Easily
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sugar is one of the least healthy things that most people consume, yet because it’s so prevalent, it can also be tricky to avoid at first, and the cravings can also be a challenge. So, how to quit it?
Step by step
Dr. Mike Hansen recommends the following steps:
- Be aware: a lot of sugar consumption is without realizing it or thinking about it, because of how common it is for there to be added sugar in things we might purchase ready-made, even supposedly healthy things like yogurts, or easy-to-disregard things like condiments.
- Recognize sugar addiction: a controversial topic, but Dr. Hansen comes down squarely on the side of “yes, it’s an addiction”. He wants us to understand more about the mechanics of how this happens, and what it does to us.
- Reduce gradually: instead of going “cold turkey”, he recommends we avoid withdrawal symptoms by first cutting back on liquid sugars like sodas, juices, and syrups, before eliminating solid sugar-heavy things like candy, sugar cookies, etc, and finally the more insidious “why did they put sugar in this?” added-sugar products.
- Find healthy alternatives: simple like-for-like substitutions; whole fruits instead of juices/smoothies, for example. 10almonds tip: stuffing dates with an almond each makes it very much like eating chocolate, experientially!
- Manage cravings: Dr. Hansen recommends distraction, and focusing on upping other healthy habits such as hydration, exercise, and getting more vegetables.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Which Sugars Are Healthier, And Which Are Just The Same?
- Mythbusting The Not-So-Sweet Science Of Sugar Addiction
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Can’t Do The Middle Splits? Two Anatomy Tricks To Get You Deeper In Seconds
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Flexibility coach Aleks Brzezinska—who first got flexible as an adult herself—explains how:
To the floor
First, understand four factors that affect how easy or hard the middle splits will be:
- Muscles: flexibility partly depends on inherent muscle stretchability, which varies between individuals. Stretching regularly works for everyone, but heavy weightlifting can hinder flexibility progress.
- Ligaments: ligament length and mobility affect joint flexibility. Longer ligaments offer more mobility but less stability, increasing injury risk. Hypermobile people tend to progress faster in flexibility. Ligaments can be stretched over time, though excessive stretching without strengthening can reduce joint stability, so it’s important to do both.
- Hormones: estrogen makes connective tissue more flexible, improving flexibility in women.
- Bone Structure: the biggest limitation in achieving full middle splits can be bone structure, particularly hip socket depth and femur shape. Shallower sockets and longer femur necks generally allow more movement. Children have more cartilage in the hips, which does aid flexibility if trained early, but it’s not too late for the rest of us, either.
Now, the two tips:
- Arch your back while attempting the split. This can help you slide deeper into the position regardless of your current level.
- Conversely, round your back and sit your hips backward. This shifts the stretch from the inner thighs to the hamstrings and mimics a wide pancake position, helping those whose hip anatomy prevents full middle splits.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Test For Whether You Will Be Able To Achieve The Splits
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What you should know about bipolar disorder
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Bipolar disorder is a mental health condition characterized by dramatic mood shifts. It affects approximately 40 million people worldwide, often significantly disrupting their daily life. But medication, therapy, and lifestyle changes can help many people manage their symptoms and live healthy lives.
Read on to learn more about its symptoms, treatment options, and more.
What are the symptoms?
People with bipolar disorder typically experience periods of high energy and an elevated mood (mania), which may be followed by periods of depression.
Symptoms of mania may include:
- Increased energy or agitation
- Excessive self-confidence
- Needing much less sleep than usual
- Speaking quickly or talking more than usual
- Racing thoughts
- Making risky or impulsive decisions
Symptoms of depression may include:
- Feeling sad, hopeless, or worthless
- Losing interest in things that typically bring you joy
- Weight loss
- Sleeping too much or too little
- Tiredness
- Having trouble concentrating
- Suicidal thoughts
These symptoms can be debilitating without treatment.
“Bipolar disorder can often significantly impair your ability to work, function in your daily life (including things like self-care), and hinder your ability to maintain personal and professional relationships,” said Marie A. Fowler, a licensed clinical social worker, in a February HealthCentral article.
While symptoms can emerge at any time, most people start experiencing them in late adolescence or early adulthood.
What are the types of bipolar disorder?
Bipolar I disorder: People with bipolar I disorder experience mania. Some may also experience periods of depression or “mixed states” of both depression and mania.
Bipolar II disorder: People with bipolar II experience periods of depression and hypomanic episodes, which are a less severe form of mania.
Cyclothymic disorder, or cyclothymia: People with cyclothymic disorder have an unstable mood most of the time, experiencing hypomania and mild depression for at least two years.
People who experience significant mood changes and do not fit the criteria above may be diagnosed with unspecified bipolar disorder.
What causes it?
Researchers don’t know the exact cause of bipolar disorder, but genetics likely play a role. More than two-thirds of people with the condition have at least one family member who has also been diagnosed with it.
Other potential contributing factors include structural brain differences, traumatic life events, and stress.
How is it diagnosed?
If you have symptoms of bipolar disorder, talk to a health care provider first to rule out illnesses like hyperthyroidism, which can cause similar symptoms.
In addition to running lab tests, your health care provider will ask questions about your symptoms and may refer you to a psychologist or psychiatrist for further evaluation. To receive a diagnosis, you must have experienced at least one episode of mania or hypomania.
Early diagnosis and intervention is important since living with bipolar disorder increases your risk of substance use disorder, anxiety, and suicide.
How is it treated?
Bipolar disorder is a lifelong mental health condition, but you can manage symptoms with therapy and medications like antidepressants and mood stabilizers. Talk to your health care provider about your medical history and other other medications you take before starting any new protocol.
Some health care providers may also recommend practices like exercise, meditation, and maintaining a regular sleep schedule to support treatment.
Maintaining treatment is important, even when you’re feeling stable. “Staying active in bipolar disorder treatment will reduce [the] recurrence of manic and depressive episodes and improve your overall quality of life,” Fowler said.
If you or anyone you know is considering suicide or self-harm or is anxious, depressed, or upset, or needs to talk, call the Suicide & Crisis Lifeline at 988 or text the Crisis Text Line at 741-741. For international resources, here is a good place to begin.
This article first appeared on Public Good News and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:


