How does cancer spread to other parts of the body?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
All cancers begin in a single organ or tissue, such as the lungs or skin. When these cancers are confined in their original organ or tissue, they are generally more treatable.
But a cancer that spreads is much more dangerous, as the organs it spreads to may be vital organs. A skin cancer, for example, might spread to the brain.
This new growth makes the cancer much more challenging to treat, as it can be difficult to find all the new tumours. If a cancer can invade different organs or tissues, it can quickly become lethal.
When cancer spreads in this way, it’s called metastasis. Metastasis is responsible for the majority (67%) of cancer deaths.
Cells are supposed to stick to surrounding tissue
Our bodies are made up of trillions of tiny cells. To keep us healthy, our bodies are constantly replacing old or damaged cells.
Each cell has a specific job and a set of instructions (DNA) that tells it what to do. However, sometimes DNA can get damaged.
This damage might change the instructions. A cell might now multiply uncontrollably, or lose a property known as adherence. This refers to how sticky a cell is, and how well it can cling to other surrounding cells and stay where it’s supposed to be.
If a cancer cell loses its adherence, it can break off from the original tumour and travel through the bloodstream or lymphatic system to almost anywhere. This is how metastasis happens.
Many of these travelling cancer cells will die, but some will settle in a new location and begin to form new cancers.
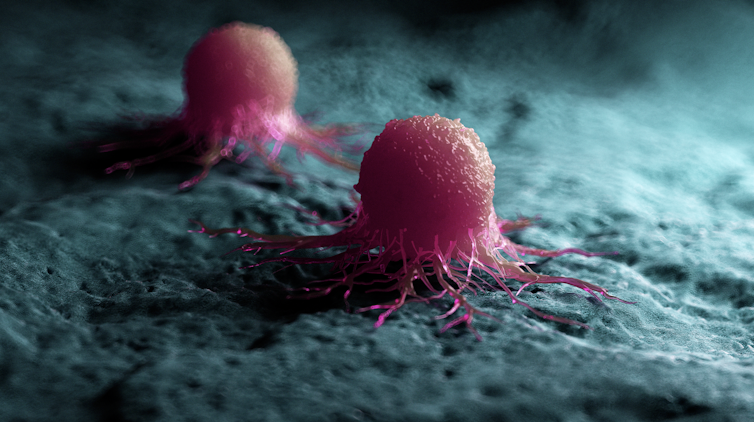
Scipro/Shutterstock
Particular cancers are more likely to metastasise to particular organs that help support their growth. Breast cancers commonly metastasise to the bones, liver, and lungs, while skin cancers like melanomas are more likely to end up in the brain and heart.
Unlike cancers which form in solid organs or tissues, blood cancers like leukaemia already move freely through the bloodstream, but can escape to settle in other organs like the liver or brain.
When do cancers metastasise?
The longer a cancer grows, the more likely it is to metastasise. If not caught early, a patient’s cancer may have metastasised even before it’s initially diagnosed.
Metastasis can also occur after cancer treatment. This happens when cancer cells are dormant during treatment – drugs may not “see” those cells. These invisible cells can remain hidden in the body, only to wake up and begin growing into a new cancer months or even years later.
For patients who already have cancer metastases at diagnosis, identifying the location of the original tumour – called the “primary site” – is important. A cancer that began in the breast but has spread to the liver will probably still behave like a breast cancer, and so will respond best to an anti-breast cancer therapy, and not anti-liver cancer therapy.
As metastases can sometimes grow faster than the original tumour, it’s not always easy to tell which tumour came first. These cancers are called “cancers of unknown primary” and are the 11th most commonly diagnosed cancers in Australia.
One way to improve the treatment of metastatic cancer is to improve our ways of detecting and identifying cancers, to ensure patients receive the most effective drugs for their cancer type.
What increases the chances of metastasis and how can it be prevented?
If left untreated, most cancers will eventually acquire the ability to metastasise.
While there are currently no interventions that specifically prevent metastasis, cancer patients who have their tumours surgically removed may also be given chemotherapy (or other drugs) to try and weed out any hidden cancer cells still floating around.
The best way to prevent metastasis is to diagnose and treat cancers early. Cancer screening initiatives such as Australia’s cervical, bowel, and breast cancer screening programs are excellent ways to detect cancers early and reduce the chances of metastasis.

Peakstock/Shutterstock
New screening programs to detect cancers early are being researched for many types of cancer. Some of these are simple: CT scans of the body to look for any potential tumours, such as in England’s new lung cancer screening program.
Using artificial intelligence (AI) to help examine patient scans is also possible, which might identify new patterns that suggest a cancer is present, and improve cancer detection from these programs.
More advanced screening methods are also in development. The United States government’s Cancer Moonshot program is currently funding research into blood tests that could detect many types of cancer at early stages.
One day there might even be a RAT-type test for cancer, like there is for COVID.
Will we be able to prevent metastasis in the future?
Understanding how metastasis occurs allows us to figure out new ways to prevent it. One idea is to target dormant cancer cells and prevent them from waking up.
Directly preventing metastasis with drugs is not yet possible. But there is hope that as research efforts continue to improve cancer therapies, they will also be more effective at treating metastatic cancers.
For now, early detection is the best way to ensure a patient can beat their cancer.![]()
Sarah Diepstraten, Senior Research Officer, Blood Cells and Blood Cancer Division, Walter and Eliza Hall Institute and John (Eddie) La Marca, Senior Resarch Officer, Walter and Eliza Hall Institute
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

“Recovery is possible when we replace judgment with compassion”: How this mother turned pain into service for others

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is the second installment in a series about Pennsylvanians in recovery from substance use disorder and how stigma affected their recovery. The series is a collaboration between Public Good News, Centro Integral de la Mujer Madre Tierra, and Life Unites Us. If you’d like to share your story, contact us at mailto:[email protected].
[Editor’s note: The contents of this interview have been edited for length and clarity. This interview was originally conducted in Spanish.]
Carmen Albrecht, 58
Outreach bilingual coordinator at Peace and Harmony House in Berks County
Reading, PennsylvaniaI am a mother of five children. I have 22 grandchildren, six great-grandchildren, and I have been married for 16 years. I came to the United States from Puerto Rico in 1979, when my parents separated. My father struggled a lot with alcohol and was abusive toward my mother.
I stayed in the United States with my father, and during that time, I decided to start a family at a very young age. By the age of 21, I already had five children. Very shortly after having my children, I was introduced to cocaine. Less than a year later, I was completely addicted.
By 1996, I had lost my five children to social services because I had become consumed by my addiction.
It controlled me completely—not only mentally, but also physically and emotionally. It numbed so much of the sadness, pain, and loneliness I had back then as a single mother.
There were many times I tried to leave it behind because people wanted me to change so I could get my children back and move forward. I was a young person, only 27 years old. With addiction, I didn’t just lose my dignity—I lost my pride and my faith.
There were many blows along the way because my own people looked at me differently and no one respected me anymore. The stigma crushed me completely, and I kept going with that pain.
I was treated badly. People called me “drug addict,” “dirty,” and told me I was worthless. They said, “They took your children away because you deserved it,” and, “Your family will never accept you like that.” There was a time in 2002 when I sought help, and my children were returned to me—but about a year and a half later, or less, I lost them again.
This is something I wrote:
“During the struggle with addiction for more than 10 years, one of the deepest wounds did not come only from the drugs, but from the stigma that surrounded me. People who called me an ‘addict’ looked at me with contempt, as if I were less than human. Over time, those words began to feel like the truth. I felt useless. I felt worthless, convinced that this was the only future waiting for me. Stigma doesn’t just hurt—it completely crushes you. It makes you believe you don’t deserve help. It makes you hide from people, hide like a worm all tangled up, making you think there is no way out. And when you are already at your lowest point, that judgment can push you even deeper—and it does. It wasn’t until I went through many jails and institutions that I was able to slow down enough to see what I could do and realize that there was hope for me. There, I received structure and support and the opportunity to begin to rebuild myself.”
When I left prison, I had already met someone—and that person did not judge me for who I was. That person supported me. I remember thinking, “That can’t be real because nobody loves me.” But he was the only one who stayed there, standing strong with me. That’s how my recovery began.

Carmen with her husband. Courtesy of Carmen Albrecht. I had to go to court, see the judge, report to parole, deal with social services, take care of my mental health, keep a job, and maintain a home—and for me, that was overwhelming. But with the support of the person who is now my husband, and the support of the job I had, I was able to complete all those programs in 18 months.
Then I said to myself, “I have to make a change in my life. I have to help those who are where I once was.” If I don’t help them, they won’t find a way out because this is incredibly hard.
So I set aside all the things that hurt me so much. Those names people called me and the ways they hurt me, that was the addiction, that wasn’t who I truly was. I am different. I am a strong person, and I can do this. Little by little, I kept going. I started studying and went back to school. I earned my GED. I completed an 18-month program in drug and alcohol counseling and got my first job serving people with mental health needs. By 2008, I was working as an assistant to social workers in a halfway house.
I had a deep hunger to keep moving forward and to keep learning more about what drugs do to people, about the damage I had done to myself, and how I was able to overcome the stigma of how people treated me and how they saw me. I had to learn to walk with my head held high, not look back, and give myself the pride of knowing that I am not that person anymore. I had to look at myself in the mirror every morning and say, “Wow, I am beautiful.”
So I kept studying. I also graduated as a Certified Recovery Specialist. I have a diploma in drug and alcohol counseling, and I also have more than 200 certificates related to working with addiction, alcohol, mental health, and homelessness because I went through all of that myself.
Until recently, I worked at the Hope Rescue Mission with people struggling with addiction, homelessness, and mental health. And now I am working as a bilingual community outreach coordinator at Peace and Harmony House in Berks County.
Even at the age I am now, I want to keep going forward. I want to help in every way I can. I have been able to help thousands and thousands of people, and I have helped send many people to rehabilitation centers who trust me deeply. I have a family that loves me unconditionally. My grandchildren love me. And by the grace of God, today I have been sober for 21 years.
I have spent 18 years working in the field of addiction, walking alongside people who are living what I once lived. Every day I see how stigma continues to be a huge barrier for those seeking help. That’s why I speak about this because no one should be defined by their worst moments. Recovery is possible when we replace judgment with compassion.
If you or anyone you know is considering suicide or self-harm or is anxious, depressed, upset, or needs to talk, call the Suicide & Crisis Lifeline at 988 or text the Crisis Text Line at 741-741. For international resources, here is a good place to begin.
If you’re looking for substance use disorder or mental health help in Pennsylvania, find a list of resources here.
This article first appeared on Public Good News and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.
Share This Post
-

Younger Next Year: The Exercise Program – by Chris Crowley & Dr. Henry Lodge
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We previously reviewed the same authors’ original “Younger Next Year”, and now here’s the more specific book about exercise for increasing healthspan and reversing markers of biological aging, going into much more detail in that regard.
How much more? Well, it’s a very hand-holding book in the sense that it walks the reader through everything step-by-step, tells not only what kind of exercise and how much, but also how to do, what things to do to prepare, how to avoid not erring in various ways, what metrics to keep an eye on to ensure you are making progress, and more.
There are also whole sections on specific common age-related issues including osteoporosis and arthritis, as well as how to train around injuries (especially of the kind that basically aren’t likely to ever fully go away).
As with the previous book, there’s a blend of motivational pep talk and science—this book is heavily weighted towards the former. It has, however, enough science to keep it on the right track throughout. Hence the two authors! Crowley for motivational pep and training tips, and Dr. Lodge for the science.
Bottom line: if you’d like to be biologically younger next year, that exercise will be an important component of that, and this book is really quite comprehensive for its relative brevity (weighing in at 176 pages).
Click here to check out Younger Next Year: The Exercise Program, and make that progress!
Share This Post
-

Total Recovery – by Dr. Gary Kaplan
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, know: Dr. Kaplan is an osteopath, and as such, will be mostly approaching things from that angle. That said, he is also board certified in other things too, including family medicine, so he’s by no means a “one-trick pony”, nor are there “when your only tool is a hammer, everything starts to look like a nail” problems to be found here. Instead, the scope of the book is quite broad.
Dr. Kaplan talks us through the diagnostic process that a doctor goes through when presented with a patient, what questions need to be asked and answered—and by this we mean the deeper technical questions, e.g. “what do these symptoms have in common”, and “what mechanism was at work when the pain become chronic”, not the very basic questions asked in the initial debriefing with the patient.
He also asks such questions (and questions like these get chapters devoted to them) as “what if physical traumas build up”, and “what if physical and emotional pain influence each other”, and then examines how to interrupt the vicious cycles that lead to deterioration of one’s condition.
The style of the book is very pop-science and often narrative in its presentation, giving lots of anecdotes to illustrate the principles. It’s a “sit down and read it cover-to-cover” book—or a chapter a day, whatever your preferred pace; the point is, it’s not a “dip directly to the part that answers your immediate question” book; it’s not a textbook or manual.
Bottom line: a lot of this work is about prompting the reader to ask the right questions to get to where we need to be, but there are many illustrative possible conclusions and practical advices to be found and given too, making this a useful read if you and/or a loved one suffers from chronic pain.
Click here to check out Total Recovery, and solve your own mysteries!
Share This Post


Related Posts
-
How does the hair-loss drug finasteride work? Can it affect my mental health?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For many men the gradual thinning of hair is about more than just their appearance. Finasteride, a drug widely prescribed for the treatment of male pattern baldness has been used effectively for many years for this deeply personal problem.
Yet, behind its use are growing concerns about its link to the development of depression, anxiety, and even suicidal thoughts.
There is now critical discussion among both users and health-care professionals about the potential hazards associated with its continued use.
So how does the drug work? And what does the evidence say about the risk of developing a mental health problem?
agrobacter/Getty How does finasteride work?
Finasteride is used to treat androgenetic alopecia, also known as male pattern baldness. It works to regrow hair and prevent the further loss of hair.
One of the key causes of pattern baldness is the production of a hormone called dihydrotestosterone which the body makes from testosterone. When it binds to the follicles of hairs, it initiates a process called hair follicle miniaturisation. This is where the growth cycle of the hair becomes progressively shorter, resulting in thinner and weaker hair.
Finasteride works by blocking the enzyme that converts testosterone to dihydrotestosterone. By blocking the enzyme, dihydrotestosterone concentrations can be reduced by around 60–70% for the majority of men.
Finasteride was first approved in the late 1990s as a prescription-only medicine and is taken as a daily 1 milligram oral tablet. Medications available at a higher 5 mg daily dose are not used for baldness, but as a treatment for non-cancerous prostate enlargement.
This medication is not indicated for women, even though they can also have this type of hair loss.
How can it impact your mental health?
Changes in mental health are not listed as an established side effect in Australian guidance given to health-care professionals.
Based on clinical trials, the most common effects include:
- decreased libido
- erectile dysfunction
- reduced semen production.
The guidance also describes an increased risk of prostate cancer and a potential risk for breast cancer. Yes, men can get breast cancer too.
While initial clinical trials conducted to obtain approval for the drug didn’t demonstrate mental health concerns, monitoring of patients using the drug has since indicated a potential increased risk of depression and suicidal thoughts. But as this is based on patients self-reporting symptoms, according to the guidance there is no definitive link.
However, in May 2025, the European Medicines Agency safety committee stated suicidal thoughts was a confirmed side effect of finasteride. The European Union also advises patients that finasteride can cause a depressed mood and depression.
Similarly, in a warning about compounded finasteride, the United States Food and Drug Administration stated in April 2025 that topical formulations of the drug has similar side effects to the oral version. These include depression, anxiety and suicidal thoughts.
What should you do if it is affecting your mental health?
If you notice changes in your mental health while taking the drug, try not to handle significant mood changes by yourself. If you’re feeling unusually low, anxious or emotionally unstable, check in with a doctor so they can help you figure out whether finasteride is contributing to your mood and what support you may need.
If the symptoms are mild, they may suggest pausing finasteride to see whether things improve, or continuing with additional mental health support. If your symptoms are more severe, stopping the medication and getting prompt medical review may be appropriate.
If you are taking finasteride and are worried about its side effects, it is safe to stop immediately. Most side effects ease once the medication is out of your system, although a small number of people have reported symptoms that persist.
If you do decide to stop, this will mean that your hormone levels will gradually return to baseline and the hair growth seen with the drug will be lost over time.
If finasteride is not the right fit for you, there is another evidence-based alternative.
Topical minoxidil is a first-line treatment that can be used on its own or with other treatments and is available from pharmacies over the counter. It only works while it’s being used and may irritate the scalp, but its effectiveness is well-established and widely recommended.
While depression and anxiety are associated with minoxidil, the incidence is much lower because of their topical application.
There is also a medication called dutasteride. However, as it works in a similar way to finasteride, it may also increase your risk of developing mental health problems. So it is best to avoid dutasteride if finasteride is not suitable for you.
If this story has raised any issues for you, please contact one of the services below:
- Lifeline: 13 11 14 or lifeline.org.au
- Suicide Call Back Service (ages 15+): 1300 659 467 or suicidecallbackservice.org.au
Nial Wheate, Professor, School of Natural Sciences, Macquarie University and Jasmine Lee, Pharmacist and PhD Candidate, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Say That Again: Using Hearing Aids Can Be Frustrating for Older Adults, but Necessary
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It was an every-other-day routine, full of frustration.
Every time my husband called his father, who was 94 when he died in 2022, he’d wait for his dad to find his hearing aids and put them in before they started talking.
Even then, my father-in-law could barely hear what my husband was saying. “What?” he’d ask over and over.
Then, there were the problems my father-in-law had replacing the devices’ batteries. And the times he’d end up in the hospital, unable to understand what people were saying because his hearing aids didn’t seem to be functioning. And the times he’d drop one of the devices and be unable to find it.
How many older adults have problems of this kind?
There’s no good data about this topic, according to Nicholas Reed, an assistant professor of epidemiology at Johns Hopkins Bloomberg School of Public Health who studies hearing loss. He did a literature search when I posed the question and came up empty.
Reed co-authored the most definitive study to date of hearing issues in older Americans, published in JAMA Open Network last year. Previous studies excluded people 80 and older. But data became available when a 2021 survey by the National Health and Aging Trends Study included hearing assessments conducted at people’s homes.
The results, based on a nationally representative sample of 2,803 people 71 and older, are eye-opening. Hearing problems become pervasive with advancing age, exceeding 90% in people 85 and older, compared with 53% of 71- to 74-year-olds. Also, hearing worsens over time, with more people experiencing moderate or severe deficits once they reach or exceed age 80, compared with people in their 70s.
However, only 29% of those with hearing loss used hearing aids. Multiple studies have documented barriers that inhibit use. Such devices, which Medicare doesn’t cover, are pricey, from nearly $1,000 for a good over-the-counter set (OTC hearing aids became available in 2022) to more than $6,000 for some prescription models. In some communities, hearing evaluation services are difficult to find. Also, people often associate hearing aids with being old and feel self-conscious about wearing them. And they tend to underestimate hearing problems that develop gradually.
Barbara Weinstein, a professor of audiology at the City University of New York Graduate Center and author of the textbook “Geriatric Audiology,” added another concern to this list when I reached out to her: usability.
“Hearing aids aren’t really designed for the population that most needs to use them,” she told me. “The move to make devices smaller and more sophisticated technologically isn’t right for many people who are older.”
That’s problematic because hearing loss raises the risk of cognitive decline, dementia, falls, depression, and social isolation.
What advice do specialists in hearing health have for older adults who have a hard time using their hearing aids? Here are some thoughts they shared.
Consider larger, customized devices. Many older people, especially those with arthritis, poor fine motor skills, compromised vision, and some degree of cognitive impairment, have a hard time manipulating small hearing aids and using them properly.
Lindsay Creed, associate director of audiology practices at the American Speech-Language-Hearing Association, said about half of her older clients have “some sort of dexterity issue, whether numbness or reduced movement or tremor or a lack of coordination.” Shekinah Mast, owner of Mast Audiology Services in Seaford, Delaware, estimates nearly half of her clients have vision issues.
For clients with dexterity challenges, Creed often recommends “behind-the-ear hearing aids,” with a loop over the ear, and customized molds that fit snugly in the ear. Customized earpieces are larger than standardized models.
“The more dexterity challenges you have, the better you’ll do with a larger device and with lots of practice picking it up, orienting it, and putting it in your ear,” said Marquitta Merkison, associate director of audiology practices at ASHA.
For older people with vision issues, Mast sometimes orders hearing aids in different colors for different ears. Also, she’ll help clients set up stands at home for storing devices, chargers, and accessories so they can readily find them each time they need them.
Opt for ease of use. Instead of buying devices that require replacing tiny batteries, select a device that can be charged overnight and operate for at least a day before being recharged, recommended Thomas Powers, a consultant to the Hearing Industries Association. These are now widely available.
People who are comfortable using a smartphone should consider using a phone app to change volume and other device settings. Dave Fabry, chief hearing health officer at Starkey, a major hearing aid manufacturer, said he has patients in their 80s and 90s “who’ve found that being able to hold a phone and use larger visible controls is easier than manipulating the hearing aid.”
If that’s too difficult, try a remote control. GN ReSound, another major manufacturer, has designed one with two large buttons that activate the volume control and programming for its hearing aids, said Megan Quilter, the company’s lead audiologist for research and development.
Check out accessories. Say you’re having trouble hearing other people in restaurants. You can ask the person across the table to clip a microphone to his shirt or put the mike in the center of the table. (The hearing aids will need to be programmed to allow the sound to be streamed to your ears.)
Another low-tech option: a hearing aid clip that connects to a piece of clothing to prevent a device from falling to the floor if it becomes dislodged from the ear.
Wear your hearing aids all day. “The No. 1 thing I hear from older adults is they think they don’t need to put on their hearing aids when they’re at home in a quiet environment,” said Erika Shakespeare, who owns Audiology and Hearing Aid Associates in La Grande, Oregon.
That’s based on a misunderstanding. Our brains need regular, not occasional, stimulation from our environments to optimize hearing, Shakespeare explained. This includes noises in seemingly quiet environments, such as the whoosh of a fan, the creak of a floor, or the wind’s wail outside a window.
“If the only time you wear hearing aids is when you think you need them, your brain doesn’t know how to process all those sounds,” she told me. Her rule of thumb: “Wear hearing aids all your waking hours.”
Consult a hearing professional. Everyone’s needs are different, so it’s a good idea to seek out an audiologist or hearing specialist who, for a fee, can provide guidance.
“Most older people are not going to know what they need” and what options exist without professional assistance, said Virginia Ramachandran, the head of audiology at Oticon, a major hearing aid manufacturer, and a past president of the American Academy of Audiology.
Her advice to older adults: Be “really open” about your challenges.
If you can’t afford hearing aids, ask a hearing professional for an appointment to go over features you should look for in over-the-counter devices. Make it clear you want the appointment to be about your needs, not a sales pitch, Reed said. Audiology practices don’t routinely offer this kind of service, but there’s good reason to ask since Medicare started covering once-a-year audiologist consultations last year.
We’re eager to hear from readers about questions you’d like answered, problems you’ve been having with your care, and advice you need in dealing with the health care system. Visit http://kffhealthnews.org/columnists to submit your requests or tips.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What should I do if I can’t see a psychiatrist?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
People presenting at emergency with mental health concerns are experiencing the longest wait times in Australia for admission to a ward, according to a new report from the Australasian College of Emergency Medicine.
But with half of New South Wales’ public psychiatrists set to resign next week after ongoing pay disputes – and amid national shortages in the mental health workforce – Australians who rely on psychiatry support may be wondering where else to go.
If you can’t get in to see a psychiatrist and you need help, there are some other options. However in an emergency, you should call 000.
Why do people see a psychiatrist?
Psychiatrists are doctors who specialise in mental health and can prescribe medication.
People seek or require psychiatry support for many reasons. These may include:
- severe depression, including suicidal thoughts or behaviours
- severe anxiety, panic attacks or phobias
- post-traumatic stress disorder (PTSD)
- eating disorders, such as anorexia or bulimia
- attention deficit hyperactivity disorder (ADHD).
Psychiatrists complement other mental health clinicians by prescribing certain medications and making decisions about hospital admission. But when psychiatry support is not available a range of team members can contribute to a person’s mental health care.
Can my GP help?
Depending on your mental health concerns, your GP may be able to offer alternatives while you await formal psychiatry care.
GPs provide support for a range of mental health concerns, regardless of formal diagnosis. They can help address the causes and impact of issues including mental distress, changes in sleep, thinking, mood or behaviour.
The GP Psychiatry Support Line also provides doctors advice on care, prescription medication and how support can work.
It’s a good idea to book a long consult and consider taking a trusted person. Be explicit about how you’ve been feeling and what previous supports or medication you’ve accessed.
What about psychologists, counsellors or community services?
Your GP should also be aware of supports available locally and online.
For example, Head to Health is a government initiative, including information, a nationwide phone line, and in-person clinics in Victoria. It aims to improve mental health advice, assessment and access to treatment.
Medicare Mental Health Centres provide in-person care and are expanding across Australia.
There are also virtual care services in some areas. This includes advice on individualised assessment including whether to go to hospital.
Some community groups are led by peers rather than clinicians, such as Alternatives to Suicide.
How about if I’m rural or regional?
Accessing support in rural or regional areas is particularly tough.
Beyond helplines and formal supports, other options include local Suicide Prevention Networks and community initiatives such as ifarmwell and Men’s sheds.
Should I go to emergency?
As the new report shows, people who present at hospital emergency departments for mental health should expect long wait times before being admitted to a ward.
But going to a hospital emergency department will be essential for some who are experiencing a physical or mental health crisis.
Managing suicide-related distress
With the mass resignation of NSW psychiatrists looming, and amid shortages and blown-out emergency waiting times, people in suicide-related distress must receive the best available care and support.
Roughly nine Australians die by suicide each day. One in six have had thoughts of suicide at some point in their lives.
Suicidal thoughts can pass. There are evidence-based strategies people can immediately turn to when distressed and in need of ongoing care.
Safety planning is a popular suicide prevention strategy to help you stay safe.
What is a safety plan?
This is a personalised, step-by-step plan to remain safe during the onset or worsening of suicidal urges.
You can develop a safety plan collaboratively with a clinician and/or peer worker, or with loved ones. You can also make one on your own – many people like to use the Beyond Now app.
Safety plans usually include:
- recognising personal warning signs of a crisis (for example, feeling like a burden)
- identifying and using internal coping strategies (such as distracting yourself by listening to favourite music)
- seeking social supports for distraction (for example, visiting your local library)
- letting trusted family or friends know how you’re feeling – ideally, they should know they’re in your safety plan
- knowing contact details of specific mental health services (your GP, mental health supports, local hospital)
- making the environment safer by removing or limiting access to lethal means
- identifying specific and personalised reasons for living.
Our research shows safety planning is linked to reduced suicidal thoughts and behaviour, as well as feelings of depression and hopelessness, among adults.
Evidence from people with lived experience shows safety planning helps people to understand their warning signs and practice coping strategies.
Sharing your safety plan with loved ones may help understand warning signs of a crisis. Dragana Gordic/Shutterstock Are there helplines I can call?
There are people ready to listen, by phone or online chat, Australia-wide. You can try any of the following (most are available 24 hours a day, seven days a week):
Suicide helplines:
- Lifeline 13 11 14
- Suicide Call Back Service 1300 659 467
There is also specialised support:
- for men: MensLine Australia 1300 78 99 78
- children and young people: Kids’ Helpline 1800 55 1800
- Aboriginal and Torres Strait Islander people: 13YARN 13 92 76
- veterans and their families: Open Arms 1800 011 046
- LGBTQIA+ community: QLife 1300 184 527
- new and expecting parents: PANDA 1300 726 306
- people experiencing eating disorders: Butterfly Foundation 1800 33 4673.
Additionally, each state and territory will have its own list of mental health resources.
With uncertain access to services, it’s helpful to remember that there are people who care. You don’t have to go it alone.
Monika Ferguson, Senior Lecturer in Mental Health, University of South Australia and Nicholas Procter, Professor and Chair: Mental Health Nursing, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: