What Most People Don’t Know About HIV
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What To Know About HIV This World AIDS Day
Yesterday, we asked 10almonds readers to engage in a hypothetical thought experiment with us, and putting aside for a moment any reason you might feel the scenario wouldn’t apply for you, asked:
❝You have unprotected sex with someone who, afterwards, conversationally mentions their HIV+ status. Do you…❞
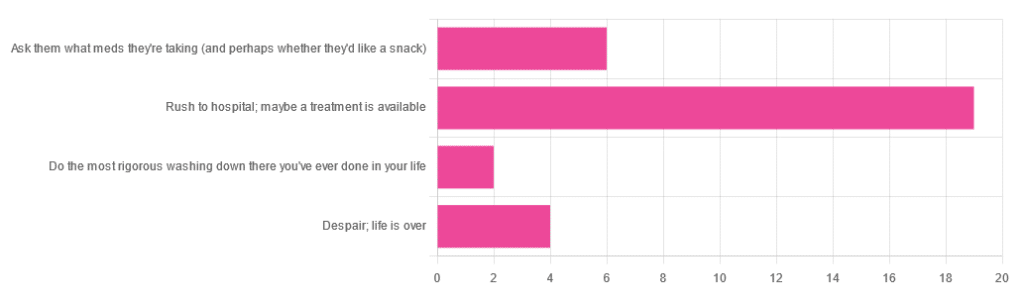
…and got the above-depicted, below-described, set of responses. Of those who responded…
- Just over 60% said “rush to hospital; maybe a treatment is available”
- Just under 20% said “ask them what meds they’re taking (and perhaps whether they’d like a snack)”
- Just over 10% said “despair; life is over”
- Two people said “do the most rigorous washing down there you’ve ever done in your life”
So, what does science say about it?
First, a quick note on terms
- HIV is the Human Immunodeficiency Virus. It does what it says on the tin; it gives humans immunodeficiency. Like many viruses that have become epidemic in humans, it started off in animals (called SIV, because there was no “H” involved yet), which were then eaten by humans, passing the virus to us when it one day mutated to allow that.
- It’s technically two viruses, but that’s beyond the scope of today’s article; for our purposes they are the same. HIV-1 is more virulent and infectious than HIV-2, and is the kind more commonly found in most of the world.
- AIDS is Acquired Immunodeficiency Syndrome, and again, is what it sounds like. When a person is infected with HIV, then without treatment, they will often develop AIDS.
- Technically AIDS itself doesn’t kill people; it just renders people near-defenseless to opportunistic infections (and immune-related diseases such as cancer), since one no longer has a properly working immune system. Common causes of death in AIDS patients include cancer, influenza, pneumonia, and tuberculosis.
People who contract HIV will usually develop AIDS if untreated. Untreated life expectancy is about 11 years.
HIV/AIDS are only a problem for gay people: True or False?
False, unequivocally. Anyone can get HIV and develop AIDS.
The reason it’s more associated with gay men, aside from homophobia, is that since penetrative sex is more likely to pass it on, then if we go with the statistically most likely arrangements here:
- If a man penetrates a woman and passes on HIV, that woman will probably not go on to penetrate someone else
- If a man penetrates a man and passes on HIV, that man could go on to penetrate someone else—and so on
- This means that without any difference in safety practices or promiscuity, it’s going to spread more between men on average, by simple mathematics.
- This is why “men who have sex with men” is the generally-designated higher-risk category.
There is medication to cure HIV/AIDS: True or False?
False so far (though there have been individual case studies of gene treatments that may have cured people—time will tell).
But! There are medications that can prevent HIV from being a life-threatening problem:
- PrEP (Pre-Exposure Prophylaxis) is a medication that one can take in advance of potential exposure to HIV, to guard against it.
- This is a common choice for people aren’t sure about their partners’ statuses, or people working in risky environments.
- PEP (Post-Exposure Prophylaxis) is a medication that one can take after potential exposure to HIV, to “nip it in the bud”.
- Those of you who were rushing to hospital in our poll, this is what you’re rushing there for.
- ARVs (Anti-RetroVirals) are a class of medications (there are different options; we don’t have room to distinguish them) that reduce an HIV+ person’s viral load to undetectable levels.
- Those of you who were asking what meds your partner was taking, these will be those meds. Also, most of them are to be taken in the morning with food, so that’s what the snack was for.
If someone is HIV+, the risk of transmission in unprotected sex is high: True or False?
True or False, with false being the far more likely. It depends on their medications, and this is why you were asking. If someone is on ARVs and their viral load is undetectable (as is usual once someone has been on ARVs for 6 months), they cannot transmit HIV to you.
U=U is not a fancy new emoticon, it means “undetectable = untransmittable”, which is a mathematically true statement in the case of HIV viral loads.
See: NIH | HIV Undetectable=Untransmittable (U=U)
If you’re thinking “still sounds risky to me”, then consider this:
You are safer having unprotected sex with someone who is HIV+ and on ARVs with an undetectable viral load, than you are with someone you are merely assuming is HIV- (perhaps you assume it because “surely this polite blushing young virgin of a straight man won’t give me cooties” etc)
Note that even your monogamous partner of many decades could accidentally contract HIV due to blood contamination in a hospital or an accident at work etc, so it’s good practice to also get tested after things that involve getting stabbed with needles, cut in a risky environment, etc.
If you’re concerned about potential stigma associated with HIV testing, you can get kits online:
CDC | How do I find an HIV self-test?
(these are usually fingerprick blood tests, and you can either see the results yourself at home immediately, or send it in for analysis, depending on the kit)
If I get HIV, I will get AIDS and die: True or False?
False, assuming you get treatment promptly and keep taking it. So those of you who were at “despair; life is over” can breathe a sigh of relief now.
However, if you get HIV, it does currently mean you will have to take those meds every day for the rest of your (no reason it shouldn’t be long and happy) life.
So, HIV is definitely still something to avoid, because it’s not great to have to take a life-saving medication every day. For a little insight as to what that might be like:
HIV.gov | Taking HIV Medication Every Day: Tips & Challenges
(as you’ll see there, there are also longer-lasting injections available instead of daily pulls, but those are much less widely available)
Summary
Some quick take-away notes-in-a-nutshell:
- Getting HIV may have been a death sentence in the 1980s, but nowadays it’s been relegated to the level of “serious inconvenience”.
- Happily, it is very preventable, with PrEP, PEP, and viral loads so low that they can’t transmit HIV, thanks to ARVs.
- Washing will not help, by the way. Safe sex will, though!
- As will celibacy and/or sexual exclusivity in seroconcordant relationships, e.g. you have the same (known! That means actually tested recently! Not just assumed!) HIV status as each other.
- If you do get it, it is very manageable with ARVs, but prevention is better than treatment
- There is no certain cure—yet. Some people (small number of case studies) may have been cured already with gene therapy, but we can’t know for sure yet.
Want to know more? Check out:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Dial Down Your Pain

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

This is Dr. Christiane Wolf. Is than an MD or a PhD, you ask? The answer is: yes (it is both; the latter being in psychosomatic medicine).
She also teaches Mindfulness-Based Stress Reduction, which as you may recall is pretty much the most well-evidenced* form of meditation there is, in terms of benefits:
No-Frills, Evidence-Based Mindfulness
*which is not to claim it is necessarily the best (although it also could be); rather, this means that it is the form of meditation that’s accumulated the most scientific backing in total. If another equal or better form of meditation enjoyed less scientific scrutiny, then there could an alternative out there languishing with only two and a half scientific papers to its name. However, we at 10almonds are not research scientists, and thus can only comment on the body of evidence that has been published.
In any case, today is going to be about pain.
What does she want us to know?
Your mind does matter
It’s easy to think that anything you can do with your mind is going to be quite small comfort when your nerves feel like they’re on fire.
However, Dr. Wolf makes the case for pain consisting of three components:
- the physical sensation(s)
- the emotions we have about those
- the meaning we give to such (or “the story” that we use to describe it)
To clarify, let’s give an example:
- the physical sensations of burning, searing, and occasionally stabbing pains in the lower back
- the emotions of anguish, anger, despair, self-pity
- the story of “this pain has ruined my life, is making it unbearable, will almost certainly continue, and may get worse”
We are not going to tell you to throw any of those out of the window for now (and, would that you could throw the first line out, of course).
The first thing Dr. Wolf wants us to do to make this more manageable is to break it down.
Because presently, all three of those things are lumped together in a single box labelled “pain”.
If each of those items is at a “10” on the scale of pain, then this is 10×10×10=1000.
If our pain is at 1000/10, that’s a lot. We want to leave the pain in the box, not look at it, and try to distract ourselves. That is one possible strategy, by the way, and it’s not always bad when it comes to giving oneself a short-term reprieve. We balanced it against meditation, here:
Managing Chronic Pain (Realistically)
However, back to the box analogy, if we open that box and take out each of those items to examine them, then even without changing anything, even with them all still at 10, they can each be managed for what they are individually, so it’s now 10+10+10=30.
If our pain is at 30/10, that’s still a lot, but it’s a lot more manageable than 1000/10.
On rating pain, by the way, see:
Get The Right Help For Your Pain
Dealing with the separate parts
It would be nice, of course, for each of those separate parts to not be at 10.
With regard to the physical side of pain, this is not Dr. Wolf’s specialty, but we have some good resources here at 10almonds:
- The 7 Approaches To Pain Management
- 10 Tips To Reduce Morning Pain & Stiffness With Arthritis
- Science-Based Alternative Pain Relief: When Painkillers Aren’t Helping, These Things Might
When it comes to emotions associated with pain, Dr. Wolf (who incidentally is a Buddhist and also a teacher of same, and runs meditation retreats for such), recommends (of course) mindfulness, and what in Dialectical Behavior Therapy (DBT) is called “radical acceptance” (in Buddhism, it may be referred to as being at one with things). We’ve written about this here:
“Hello, Emotions”: Radical Acceptance In CBT & DBT
Once again, the aim here is still not to throw the (often perfectly valid) emotions out of the window (unless you want to), but rather, to neutrally note and acknowledge the emotions as they arrive, á la “Hello, despair. Depression, my old foe, we meet again. Hello again, resentment.” …and so on.
The reason this helps is because emotions, much like the physical sensations of pain, are first and foremost messengers, and sometimes (as in the case of chronic pain) they get broken and keep delivering the message beyond necessity. Acknowledging the message helps your brain (and all that is attached to it) realize “ok, this message has been delivered now; we can chill about it a little”.
Having done that, if you can reasonably tweak any of the emotions (for example, perhaps that self-pity we mentioned could be turned into self-compassion, which is more useful), that’s great. If not, at least you know what’s on the battlefield now.
When we examine the story of our pain, lastly, Dr. Wolf invites us to look at how one of the biggest drivers of distress under pain is the uncertainty of how long the pain will last, whether it will get worse, whether what we are doing will make it worse, and so forth. See for example:
How long does back pain last? And how can learning about pain increase the chance of recovery?
And of course, many things we do specifically in response to pain can indeed make our pain worse, and spread:
Dr. Wolf’s perspective says:
- Life involves pain
- Pain invariably has a cause
- What has a cause, can have an end
- We just need to go through that process
This may seem like small comfort when we are in the middle of the pain, but if we’ve broken it down into parts with Dr. Wolf’s “box method”, and dealt with the first two parts (the sensations and the emotions) as well as reasonably possible, then we can tackle the third one (the story) a little more easily than we could if we were trying to come at it with no preparation.
What used to be:
“This pain has ruined my life, is making it unbearable, will almost certainly continue, and may get worse”
…can now become:
“This pain is a big challenge, but since I’m here for it whether I want to be or not, I will suffer as I must, while calmly looking for ways to reduce that suffering as I go.”
In short: you cannot “think healing thoughts” and expect your pain to go away. But you can do a lot more than you might (if you left it unexamined) expect.
Want to know more from Dr. Wolf?
We reviewed a book of hers recently, which you might enjoy:
Outsmart Your Pain – by Dr. Christiane Wolf
Take care!
Share This Post
-

The Off-Button For Your Brain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Off-Button For Your Brain
We evolved our emotions for our own benefit as a species. Even the “negative” ones:
- Stress keeps us safe by making sure we take important situations seriously
- Anger keeps us safe by protecting us from threats
- Disgust keeps us safe by helping us to avoid things that might cause disease
- Anxiety keeps us safe by ensuring we don’t get complacent
- Guilt keeps us safe by ensuring we can function as a community
- Sadness keeps us safe by ensuring we value things that are important to us, and learn to become averse to losing them
- …and so on
But that’s not always useful. What was once a very good response to a common source of fear (for example, a sabre-toothed tiger) is no longer a helpful response to a modern source of fear (for example, an important interview).
Sometimes it’s good to take the time and energy to process our feelings and the event(s) that prompted those feelings. Sometimes, we don’t have that luxury.
For example, if you are stressed about your workload? Then staying awake half the night thinking about it is only going to make your problems worse the next day.
So, how to switch that off, or at least put a pause on it?
The human mind tends to have a “negative bias”, evolved for our own protection. If something is “good enough”, we don’t need to worry about it, so we move on to the next thing, until we find something that is a problem, then we dwell on that. That’s not always helpful, and the good news is, there’s a way to flip the switch on this process:
Identifying the positive, and releasing the rest
This exercise can be done when you’re trying to sleep, or at any time you need a calmer, quieter mind.
Take a moment to notice whatever you’re experiencing.
If it’s something that feels good, or neutral, identify it with a single word. For example:
- Warmth
- Soft
- Security
- Smile
- Peace
If it’s something that feels bad, then instead of identifying it, simply say (or think) to yourself “release”.
You can’t fight bad feelings with force, and you can’t “just not think about them”, but you can dismiss them as soon as they arrive and move onto the next thing. So where your train of thought may previously have been:
It’s good to be in bed ➔ I have eight hours to sleep before my meeting ➔ Have I done everything I was supposed to? ➔ I hope that what I’ve done is good enough ➔ [Mentally rehearsing how the meeting might go] ➔ [various disaster preparations] ➔ What am I even going to wear? ➔ Ugh I forgot to do the laundry ➔ That reminds the electricity bill is due ➔ Etc
Now your train of thought may be more like:
Relief ➔ Rest ➔ But my meeti—release ➔ If I—release ➔ soft ➔ comfort ➔ release ➔ pillow ➔ smile ➔ release ➔ [and before you know it you’re asleep]
And if you do this in a situation where you’re not going to sleep? Same process, just a more wakeful result, for example, let’s move the scene to an office where your meeting will shortly take place:
Five minutes to go ➔ What a day ➔ Ok, I’d better clear my head a bit ➔ release ➔ release ➔ breath ➔ light ➔ chair ➔ what if—release ➔ prepared ➔ ready ➔ calm ➔ [and before you know it you’re impressing your work associate with your calm preparedness]
In summary:
If you need to stop a train of thought, this method may help. Especially if you’re in a situation where you can’t use some external distraction to keep you from thinking about the bad thing!
You’re probably still going to have to deal with the Bad Thing™ at some point—you’ve just recognized that now isn’t the time for that. Mentally postpone that so that you will be well-rested when you choose to deal with the Bad Thing™ later at your convenience.
So remember: identify the positive (with a single word), and anything else, just release.
Share This Post
-
Chickpeas vs Mung Beans – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing chickpeas to mung beans, we picked the chickpeas.
Why?
Both are great! But there’s a clear winner here:
In terms of macros, chickpeas have more protein, carbs, and fiber, as well as the lower glycemic index. The difference is very small, but it’s a nominal win for chickpeas.
When it comes to vitamins, chickpeas have more of vitamins A, B2, B6, B9, C, E, K, and choline, while mung beans have more of vitamins B1, B3, and B5. Again the differences aren’t huge, but by strength of numbers they’re in chickpeas’ favor, so it’s another win for chickpeas here.
In the category of minerals, chickpeas have more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while mung beans are not higher in any mineral. An easy win for chickpeas on this one.
Adding up the sections makes for a clear overall win for chickpeas, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like to read:
Plant vs Animal Protein: Head to Head
Enjoy!
Share This Post
Related Posts
-

Apples vs Carrots – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apples to carrots, we picked the carrots.
Why?
Both are sweet crunchy snacks, both rightly considered very healthy options, but one comes out clearly on top…
Both contain lots of antioxidants, albeit mostly different ones. They’re both good for this.
Looking at their macros, however, apples have more carbs while carrots have more fiber. The carb:fiber ratio in apples is already sufficient to make them very healthy, but carrots do win.
In the category of vitamins, carrots have many times more of vitamins A, B1, B2, B3, B5, B6, B9, C, E, K, and choline. Apples are not higher in any vitamins.
In terms of minerals, carrots have a lot more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. Apples are not higher in any minerals.
If “an apple a day keeps the doctor away”, what might a carrot a day do?
Want to learn more?
You might like to read:
Sugar: From Apples to Bees, and High-Fructose C’s
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Blood, urine and other bodily fluids: how your leftover pathology samples can be used for medical research
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A doctor’s visit often ends with you leaving with a pathology request form in hand. The request form soon has you filling a sample pot, having blood drawn, or perhaps even a tissue biopsy taken.
After that, your sample goes to a clinical pathology lab to be analysed, in whichever manner the doctor requested. All this is done with the goal of getting to the bottom of the health issue you’re experiencing.
But after all the tests are done, what happens with the leftover sample? In most cases, leftover samples go in the waste bin, destined for incineration. Sometimes though, they may be used again for other purposes, including research.

Kaboompics.com/Pexels Who can use my leftover samples?
The samples we’re talking about here cover the range of samples clinical labs receive in the normal course of their testing work. These include blood and its various components (including plasma and serum), urine, faeces, joint and spinal fluids, swabs (such as from the nose or a wound), and tissue samples from biopsies, among others.
Clinical pathology labs often use leftover samples to practise or check their testing methods and help ensure test accuracy. This type of use is a vital part of the quality assurance processes labs need to perform, and is not considered research.
Leftover samples can also be used by researchers from a range of agencies such as universities, research institutes or private companies.
They may use leftover samples for research activities such as trying out new ideas or conducting small-scale studies (more on this later). Companies that develop new or improved medical diagnostic tests can also use leftover samples to assess the efficacy of their test, generating data needed for regulatory approval.
What about informed consent?
If you’ve ever participated in a medical research project such as a clinical trial, you may be familiar with the concept of informed consent. In this process, you have the opportunity to learn about the study and what your participation involves, before you decide whether or not to participate.
So you may be surprised to learn using leftover samples for research purposes without your consent is permitted in most parts of Australia, and elsewhere. However, it’s only allowed under certain conditions.
In Australia, the National Health and Medical Research Council (NHMRC) offers guidance around the use of leftover pathology samples.
One of the conditions for using leftover samples without consent for research is that they were received and retained by an accredited pathology service. This helps ensure the samples were collected safely and properly, for a legitimate clinical reason, and that no additional burdens or risk of harm to the person who provided the sample will be created with their further use.
Another condition is anonymity: the leftover samples must be deidentified, and not easily able to be reidentified. This means they can only be used in research if the identity of the donor is not needed.
Leftover pathology samples are sometimes used in medical research. hedgehog94/Shutterstock The decision to allow a particular research project to use leftover pathology samples is made by an independent human research ethics committee which includes consumers and independent experts. The committee evaluates the project and weighs up the risks and potential benefits before permitting an exemption to the need for informed consent.
Similar frameworks exist in the United States, the United Kingdom, India and elsewhere.
What research might be done on my leftover samples?
You might wonder how useful leftover samples are, particularly when they’re not linked to a person and their medical history. But these samples can still be a valuable resource, particularly for early-stage “discovery” research.
Research using leftover samples has helped our understanding of antibiotic resistance in a bacterium that causes stomach ulcers, Helicobacter pylori. It has helped us understand how malaria parasites, Plasmodium falciparum, damage red blood cells.
Leftover samples are also helping researchers identify better, less invasive ways to detect chronic diseases such as pulmonary fibrosis. And they’re allowing scientists to assess the prevalence of a variant in haemoglobin that can interfere with widely used diagnostic blood tests.
All of this can be done without your permission. The kinds of tests researchers do on leftover samples will not harm the person they were taken from in any way. However, using what would otherwise be discarded allows researchers to test a new method or treatment and avoid burdening people with providing fresh samples specifically for the research.
When considering questions of ethics, it could be argued not using these samples to derive maximum benefit is in fact unethical, because their potential is wasted. Using leftover samples also minimises the cost of preliminary studies, which are often funded by taxpayers.
The use of leftover pathology samples in research has been subject to some debate. Andrey_Popov/Shutterstock Inconsistencies in policy
Despite NHMRC guidance, certain states and territories have their own legislation and guidelines which differ in important ways. For instance, in New South Wales, only pathology services may use leftover specimens for certain types of internal work. In all other cases consent must be obtained.
Ethical standards and their application in research are not static, and they evolve over time. As medical research continues to advance, so too will the frameworks that govern the use of leftover samples. Nonetheless, developing a nationally consistent approach on this issue would be ideal.
Striking a balance between ensuring ethical integrity and fostering scientific discovery is essential. With ongoing dialogue and oversight, leftover pathology samples will continue to play a crucial role in driving innovation and advances in health care, while respecting the privacy and rights of individuals.
Christine Carson, Senior Research Fellow, School of Medicine, The University of Western Australia and Nikolajs Zeps, Professor, School of Public Health and Preventive Medicine, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Boundary-Setting Beyond “No”
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
More Than A “No”
A lot of people struggle with boundary-setting, and it’s not always the way you might think.
The person who “can’t say no” to people probably comes to mind, but the problem is more far-reaching than that, and it’s rooted in not being clear over what a boundary actually is.
For example: “Don’t bring him here again!”
Pretty clear, right?
And while it is indeed clear, it’s not a boundary; it’s a command. Which may or may not be obeyed, and at the end of the day, what right have we to command people in general?
Same goes for less dramatic things like “Don’t talk to me about xyz”, which can still be important or trivial, depending on whether the topic of xyz is deeply traumatizing for you, or mildly annoying, or something else entirely.
Why this becomes a problem
It becomes a problem not because of any lack of clarity about your wishes, but rather, because it opens the floor for a debate. The listener may be given to wonder whether your right to not experience xyz is greater or lesser than their right to do/say/etc xyz.
“My right to swing my fist ends where someone else’s nose begins”
…does not help here, firstly because both sides will believe themself (or nobody) to be the injured party; for the fist-swinger, the other person’s nose made a vicious assault on their freedom. Or secondly, maybe there was some higher principle at stake; a reason why violence was justified. And then ten levels of philosophical debate. We see this a lot when it comes to freedom of expression, and vigorous debate over whether this entails freedom from social consequences of one’s words/actions.
How a good boundary-setting works (if this, then that)
Consider two signs:
- No trespassing!
- Trespassers will be shot!
Superficially, the second just seems like a more violent rendition of the first. But in fact, the second is more informationally useful: it explains what will happen if the boundary is not respected, and allows the reader to make their own informed decision with regard to what to do with that information.
We can employ this method (and can even do so gently, if we so wish and hopefully we mostly do wish to be gentle) when it comes to social and interpersonal boundary-setting:
- If you bring him here again, I will refuse you entrance
- If you bring up that topic again, I will ask you to leave
- If you do that, I will never speak to you again
- If you don’t stop drinking, I will divorce you
This “if-this-then-that” model does the very first thing that any good boundary does: make itself clear.
It doesn’t rely on moral arguments; it doesn’t invite debate. For example in that last case, it doesn’t argue that the partner doesn’t have the right to drink—it simply expresses what the speaker will exercise their own right to do, in that eventuality.
(as an aside, the situation that occurs when one is enmeshed with someone who is dependent on a substance is a complex topic, and if you’re interested in that, check out: Codependency Isn’t What Most People Think)
Back on track: boundary-setting is not about what’s right or good—it’s about nothing more nor less than a clear delineation between what we will and won’t accept, and how we’ll enforce that.
We can also, in particularly personal boundary-setting (such as with sexual boundaries’ oft-claimed “gray areas”), fix an improperly-set boundary that forgot to do the above, e.g:
“How about [proposition]?”
“No thank you” ← casually worded answer; contextually reasonable, and yet not a clear boundary per what we discussed above
“Come on, I think you’d like it”
“I said no. No means no. Ask me again and I will [consequences that are appropriate and actionable]”What’s “appropriate and actionable” may vary a lot from one situation to another, but it’s important that it’s something you can do and are prepared to do and will do if the condition for doing it is met.
Anything less than that is not a boundary—it’s just a request.
Note: this does not require that we have power, by the way. If we have zero power in a situation, well, that definitely sucks, but even then we can still express what is actionable, e.g. “I will never trust you again”.
“Price of entry”
You may have wondered, upon reading “boundary-setting is not about what’s right or good—it’s about nothing more nor less than a clear delineation between what we will and won’t accept, and how we’ll enforce that”, can’t that be used to control and manipulate people, essentially coercing them to do or not do things with the threat of consequences (specifically: bad ones)?
And the answer is: yes, yes it can.
But that’s where the flipside comes into play—the other person gets to set their boundaries, too.
For all of us, if we have any boundaries at all, there is a “price of entry” and all who want to be in our lives, or be close to us, have to decide for themselves whether that price of entry is worth it.
- If a person says “do not talk about topic xyz to me or I will leave”, that is a price of entry for being close to them.
- If you are passionate about talking about topic xyz to the point that you are unwilling to shelve it when in their presence, then that is the price of entry for being close to you.
- If one or more of you is not willing to pay the price of entry, then guess what, you’re just not going to be close.
In cases of forced proximity (e.g. workplaces or families) this is likely to get resolved by the workplace’s own rules (i.e. the price of entry that you agreed to when signing a contract to work there), and if something like that doesn’t exist (such as in families), well, that forced proximity is going to reach a breaking point, and somebody may discover it wasn’t enforceable after all.
See also: Family Estrangement: More Common Than Most People Think
…which also details how to fix it, where possible.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: