HBD: The Human Being Diet – by Petronella Ravenshear
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We don’t often review diet books, so why did this one catch our attention? The answer lies in its comprehensive nature without being excessively long and complex.
Ravenshear (a nutritionist) brings a focus on metabolic balance, and what will and won’t work for keeping it healthy.
The first part of the book is mostly informational; covering such things as blood sugar balance, gut health, hormones, and circadian rhythm considerations, amongst others.
The second, larger part of the book is mostly instructional; do this and that, don’t do the other, guidelines on quantities and timings, and what things may be different for some people, and what to do about those.
The style is conversational and light, but well-grounded in good science.
Bottom line: if you’d like a “one-stop shop” for giving your diet an overhaul, this book is a fine choice.
Click here to check out the Human Being Diet, and enjoy the best of health!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

AI: The Doctor That Never Tires?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
AI: The Doctor That Never Tires?

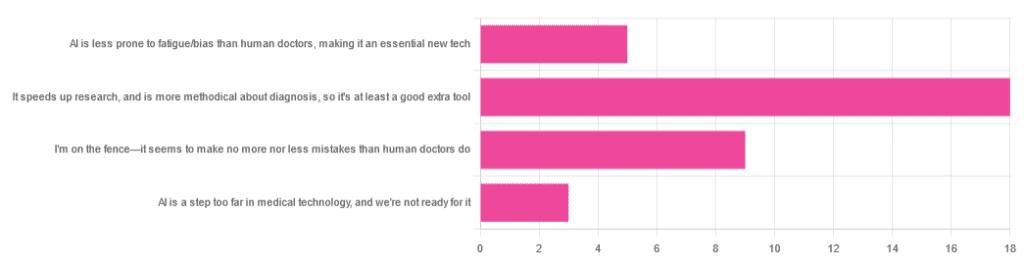
We asked you for your opinion on the use of Artificial Intelligence (AI) in healthcare, and got the above-depicted, below-described set of results:
- A little over half of respondents to the poll voted for “It speeds up research, and is more methodical about diagnosis, so it’s at least a good extra tool”
- A quarter of respondents voted for “I’m on the fence—it seems to make no more nor less mistakes than human doctors do”
- A little under a fifth of respondents voted for “AI is less prone to fatigue/bias than human doctors, making it an essential new tech”
- Three respondents voted for “AI is a step too far in medical technology, and we’re not ready for it”
Writer’s note: I’m a professional writer (you’d never have guessed, right?) and, apparently, I really did write “no more nor less mistakes”, despite the correct grammar being “no more nor fewer mistakes”. Now, I know this, and in fact, people getting less/fewer wrong is a pet hate of mine. Nevertheless, I erred.
Yet, now that I’m writing this out in my usual software, and not directly into the poll-generation software, my (AI!) grammar/style-checker is highlighting the error for me.
Now, an AI could not do my job. ChatGPT would try, and fail miserably. But can technology help me do mine better? Absolutely!
And still, I dismiss a lot of the AI’s suggestions, because I know my field and can make informed choices. I don’t follow it blindly, and I think that’s key.
AI is less prone to fatigue/bias than human doctors, making it an essential new tech: True or False?
True—with one caveat.
First, a quick anecdote from a subscriber who selected this option in the poll:
❝As long as it receives the same data inputs as my doctor (ie my entire medical history), I can see it providing a much more personalised service than my human doctor who is always forgetting what I have told him. I’m also concerned that my doctor may be depressed – not an ailment that ought to affect AI! I recently asked my newly qualified doctor goddaughter whether she would prefer to be treated by a human or AI doctor. No contest, she said – she’d go with AI. Her argument was that human doctors leap to conclusions, rather than properly weighing all the evidence – meaning AI, as long as it receives the same inputs, will be much more reliable❞
Now, an anecdote is not data, so what does the science say?
Well… It says the same:
❝Of 6695 responding physicians in active practice, 6586 provided information on the areas of interest: 3574 (54.3%) reported symptoms of burnout, 2163 (32.8%) reported excessive fatigue, and 427 (6.5%) reported recent suicidal ideation, with 255 of 6563 (3.9%) reporting a poor or failing patient safety grade in their primary work area and 691 of 6586 (10.5%) reporting a major medical error in the prior 3 months. Physicians reporting errors were more likely to have symptoms of burnout (77.6% vs 51.5%; P<.001), fatigue (46.6% vs 31.2%; P<.001), and recent suicidal ideation (12.7% vs 5.8%; P<.001).❞
See the damning report for yourself: Physician Burnout, Well-being, and Work Unit Safety Grades in Relationship to Reported Medical Errors
AI, of course, does not suffer from burnout, fatigue, or suicidal ideation.
So, what was the caveat?
The caveat is about bias. Humans are biased, and that goes for medical practitioners just the same. AI’s machine learning is based on source data, and the source data comes from humans, who are biased.
See: Bias and Discrimination in AI: A Cross-Disciplinary Perspective
So, AI can perpetuate human biases and doesn’t have a special extra strength in this regard.
The lack of burnout, fatigue, and suicidal ideation, however, make a big difference.
AI speeds up research, and is more methodical about diagnosis: True or False?
True! AI is getting more and more efficient at this, and as has been pointed out, doesn’t make errors due to fatigue, and often comes to accurate conclusions near-instantaneously. To give just one example:
❝Deep learning algorithms achieved better diagnostic performance than a panel of 11 pathologists participating in a simulation exercise designed to mimic routine pathology workflow; algorithm performance was comparable with an expert pathologist interpreting whole-slide images without time constraints. The area under the curve was 0.994 (best algorithm) vs 0.884 (best pathologist).❞
About that “getting more and more efficient at this”; it’s in the nature of machine learning that every new piece of data improves the neural net being used. So long as it is getting fed new data, which it can process at rate far exceeding humans’ abilities, it will always be constantly improving.
AI makes no more nor
lessfewer mistakes than humans do: True or False?False! AI makes fewer, now. This study is from 2021, and it’s only improved since then:
❝Professionals only came to the same conclusions [as each other] approximately 75 per cent of the time. More importantly, machine learning produced fewer decision-making errors than did all the professionals❞
See: AI can make better clinical decisions than humans: study
All that said, we’re not quite at Star Trek levels of “AI can do a human’s job entirely” just yet:
BMJ | Artificial intelligence versus clinicians: pros and cons
To summarize: medical AI is a powerful tool that:
- Makes healthcare more accessible
- Speeds up diagnosis
- Reduces human error
…and yet, for now at least, still requires human oversights, checks and balances.
Essentially: it’s not really about humans vs machines at all. It’s about humans and machines giving each other information, and catching any mistakes made by the other. That way, humans can make more informed decisions, and still keep a “hand on the wheel”.
Share This Post
-

Demystifying Cholesterol
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
All About Cholesterol
When it comes to cholesterol, the most common lay understanding (especially under a certain age) is “it’s bad”.
A more informed view (and more common after a certain age) is “LDL cholesterol is bad; HDL cholesterol is good”.
A more nuanced view is “LDL cholesterol is established as significantly associated with (and almost certainly a causal factor of) atherosclerotic cardiovascular disease and related mortality in men; in women it is less strongly associated and may or may not be a causal factor”
You can read more about that here:
Statins: His & Hers? ← we highly recommend reading this, especially if you are a woman and/or considering/taking statins. To be clear, we’re not saying “don’t take statins!”, because they might be the right medical choice for you and we’re not your doctors. But we are saying: here’s something to at least know about and consider.
Beyond HDL & LDL
Aside from high density lipoprotein (HDL) and low-density lipoprotein (LDL) here is also VLDL cholesterol, which as you might have guessed, stands for “very low-density lipoprotein”. It has a high, unhealthy triglyceride content, and it increases atherosclerotic plaque. In other words, it hardens your arteries more quickly.
The term “hardening the arteries” is an insufficient descriptor of what’s happening though, because while yes it is hardening the arteries, it’s also narrowing them. Because minerals and detritus passing through in the blood (the latter sounds bad, but there is supposed to be detritus passing through in the blood; it’s got to get out of the body somehow, and it’s off to get filtered and excreted) get stuck in the cholesterol (which itself is a waxy substance, by the way) and before you know it, those minerals and other things have become a solid part of the interior of your artery wall, like a little plastering team came and slapped plaster on the inside of the walls, then when it hardened, slapped more plaster on, and so on. Macrophages (normally the body’s best interior clean-up team) can’t eat things much bigger than themselves, so that means they can’t tackle the build-up of plaque.
Impact on the heart
Narrower less flexible arteries means very poor circulation, which means that organs can start having problems, which obviously includes your heart itself as it is not only having to do a harder job to keep the blood circulating through the narrower blood vessels, but also, it is not immune to also being starved of oxygen and nutrients along with the rest of the body when the circulation isn’t good enough. It’s a catch 22.
What if LDL is low and someone is getting heart disease anyway?
That’s often a case of apolipoprotein B, and unlike lipoprotein A, which is bound to LDL so usually* isn’t a problem if LDL is in “safe” ranges, Apo-B can more often cause problems even when LDL is low. Neither of these are tested for in most standard cholesterol tests by the way, so you might have to ask for them.
*Some people, around 1 in 20 people, have hereditary extra risk factors for this.
What to do about it?
Well, get those lipids tests! Including asking for the LpA and Apo-B tests, especially if you have a history of heart disease in your family, or otherwise know you have a genetic risk factor.
With or without extra genetic risks, it’s good to get lipids tests done annually from 40 onwards (earlier, if you have extra risk factors).
See also: Understanding your cholesterol numbers
Wondering whether you have an increased genetic risk or not?
Genetic Testing: Health Benefits & Methods ← we think this is worth doing; it’s a “one-off test tells many useful things”. Usually done from a saliva sample, but some companies arrange a blood draw instead. Cost is usually quite affordable; do shop around, though.
Additionally, talk to your pharmacist to check whether any of your meds have contraindications or interactions you should be aware of in this regard. Pharmacists usually know contraindications/interactions stuff better than doctors, and/but unlike doctors, they don’t have social pressure on them to know everything, which means that if they’re not sure, instead of just guessing and reassuring you in a confident voice, they’ll actually check.
Lastly, shocking nobody, all the usual lifestyle medicine advice applies here, especially get plenty of moderate exercise and eat a good diet, preferably mostly if not entirely plant-based, and go easy on the saturated fat.
Note: while a vegan diet contains zero dietary cholesterol (because plants don’t make it), vegans can still get unhealthy blood lipid levels, because we are animals and—like most animals—our body is perfectly capable of making its own cholesterol (indeed, we do need some cholesterol to function), and it can make its own in the wrong balance, if for example we go too heavy on certain kinds of (yes, even some plant-based) saturated fat.
Read more: Can Saturated Fats Be Healthy? ← see for example how palm oil and coconut oil are both plant-based, and both high in saturated fat, but palm oil’s is heart-unhealthy on balance, while coconut oil’s is heart-healthy on balance (in moderation).
Want to know more about your personal risk?
Try the American College of Cardiology’s ASCVD risk estimator (it’s free)
Take care!
Share This Post
-

5 Surprising Symptoms of Hypertonic Pelvic Floor
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You’ve doubtlessly heard about “pelvic floor problems” as being a matter of weak pelvic floor muscles.
And while that’s certainly most common, the opposite (after a fashion) can also be a problem:
Too much of a good thing
The pelvic floor is normally a bowl-shaped group of muscles that contract upwards when activated and relax downwards at rest. In the “hypertonic” state, they are already contracted at rest, more like a flat plate than a bowl, similar to shoulders that sit shrugged up without the person realizing.
The five symptoms, or rather the categories of symptoms, are:
- bladder problems: urgency and overactive bladder, painful bladder syndrome, pain while filling or emptying, interstitial cystitis, and urinary retention where muscles can’t relax enough to fully empty the bladder.
- bowel problems: rectal obstruction (feeling that nothing can come out), constipation, non-relaxing puborectalis muscle, and/or recurrent fissures or hemorrhoids, due to the poor muscle relaxation and resultantly reduced blood flow for healing.
- sexual problems: painful intercourse (dyspareunia), vaginismus (muscles so tight that penetration isn’t possible), pain with tampon or similar insertion, and/or vulvodynia or vestibulodynia, characterized by pain localized to vulvar or vestibular area, rather than the vagina itself.
- neurological problems: constant tension can compress the pudendal, iliohypogastric, and genitofemoral nerves (amongst others), leading to neuralgia and nerve pain in their distribution areas (i.e. where the nerves run to and from these parts).
- orthopedic problems: pelvic floor muscles connect to the pelvis and core, so hypertonicity can contribute to unresolved low back pain, tailbone pain, sacroiliac joint pain, hip pain, or pubic symphysis dysfunction.
What to do about these things? Pelvic relaxation exercises can help. Massage is usually beneficial (yes, there, and yes, that kind can also help), and assessment and treatment with a pelvic physical therapist can restore a more relaxed resting state and thus reduce the symptoms.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
To Pee Or Not To Pee ← there is, in fact, a flood of reasons not to hold
Take care!
Share This Post


Related Posts
-
Try This At Home: ABI Test For Clogged Arteries
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Arterial plaque is a big deal, and statistically it’s more of a risk as we get older, often coming to a head around age 72 for women and 65 for men—these are the median ages at which people who are going to get heart attacks, get them. Or get it, because sometimes one is all it takes.
The Ankle-Brachial Index Test
Dr. Brewer recommends a home test for detecting arterial plaque called the Ankle-Brachial Index (ABI), which uses a blood pressure monitor. The test involves measuring blood pressure in both the arms and ankles, then calculating the ratio of these measurements:
- A healthy ABI score is between 1.0 and 1.4; anything outside this range may indicate arterial problems.
- Low ABI scores (below 0.8) suggest plaque is likely obstructing blood flow
- High ABI scores (above 1.4) may indicate artery hardening
Peripheral Artery Disease (PAD), associated with poor ABI results (be they high or low), can cause a whole lot of problems that are definitely better tackled sooner rather than later—remember that atherosclerosis is a self-worsening thing once it gets going, because narrower walls means it’s even easier for more stuff to get stuck in there (and thus, the new stuff that got stuck also becomes part of the walls, and the problem gets worse).
If you need a blood pressure monitor, by the way, here’s an example product on Amazon.
Do note also that yes, if you have plaque obstructing blood flow and hardened arteries, your scores may cancel out and give you a “healthy” score, despite your arteries being very much not healthy. For this reason, this test can be used to raise the alarm, but not to give the “all clear”.
For more on all of the above, plus a demonstration and more in-depth explanation of the test, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
7-Minute Face Fitness For Lymphatic Drainage & Youthful Jawline
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Valeriia Veksler is a registered nurse with a background in cosmetic medicine. She’s been practicing for 7 years, and on the strength of that, is going to teach us how to give our face some love for 7 minutes:
The routine, step by step
Preparation: clean your face and apply your usual moisturizer. Breathe deeply: Inhale through the nose, exhale to release tension.
Neck massage: use fingertips in circular motion from the bottom of the neck to the hairline and back for 30 seconds. This helps promote blood flow to the face.
Sternocleidomastoid massage: use knuckles to massage in circles from the sternal area up to the jawline and down to the collarbone for 30 seconds. Keep posture straight, shoulders down, and relax muscles.
Collarbone pressure: apply and release pressure with fingertips above the collarbones for 30 seconds. This stimulates lymphatic flow and helps reduce puffiness.
Under-chin massage: use knuckles to massage side-to-side under the chin for 30 seconds. Relax the under-chin area and promote lymphatic drainage.
Jawline massage: with knuckles, massage from the chin towards the ears in circular motion for 30 seconds. Relax the jaw.
Nasolabial fold and nose massage: place index fingers near nostrils and move mouth in a “O” shape, then massage around the nostrils and up the nose for 30 seconds.
Smile line lift: press palms on the smile lines and slide hands up towards the temples for 30 seconds. This helps lift the face and sculpt cheekbones.
Under-eye massage: use index fingers in a hook shape, massaging under the eyes along the bone structure for 30 seconds. This promotes blood flow and lymphatic drainage.
Temple lift: use fingertips to lift the area near the left temple for 30 seconds, then assist with the opposite hand to lift further. Repeat on the other side. This reduces crow’s feet and lifts the corners of the eyes.
Forehead lift: place hands on the forehead, lock fingers, and gently elevate the skin upwards. Glide fingers towards the hairline for 30 seconds. This promotes blood flow and smooths the forehead.
Relax 11 Lines: place fingers at the center of the forehead, gently press into the tissue, and let them glide away from each other towards the eyebrows for 30 seconds.
Bonus:
- Ensure good posture throughout.
- Relax, stay mindful, and breathe deeply during the exercises.
- Feel the warmth and energy from improved circulation, after the routine.
For more on all of this plus a visual demonstration of everything, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Top 10 Foods That Promote Lymphatic Drainage and Lymph Flow
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What’s Really Keeping You Awake? The Brain’s Role in Sleepless Nights
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Tracey Marks, psychiatrist, explains:
All in your head (which is the least helpful place for it to be when trying to sleep)
Why You Can’t Sleep: sleeplessness often stems from a conflict between your brain’s sleep drive (powered by adenosine and melatonin) and wake drive (powered by orexin and serotonin), which are normally balanced by your circadian rhythm.
About that tech: blue light gets a bad reputation, and indeed it suppresses melatonin, but this is quickly resolved once you turn it off. However, being accustomed to constant notifications triggers dopamine, keeping your brain in a heightened state of alertness, even if you’ve now put your phone aside, if you’re still expecting notifications.
About your worries: worrying at night activates the brain’s stress response (HPA axis), releasing cortisol and adrenaline that override sleep signals—especially when you miss your natural sleep window and are trying to sleep at a slightly different time than you normally do.
This can then become a self-perpetuating cycle, because after poor sleep, your brain can start associating your bed with stress, reinforcing insomnia through classical conditioning.
Some advices that Dr. Marks gives include:
- Follow natural sleep rhythms where possible, rather than trying to force something different.
- Use paradoxical intention (stop trying so hard to sleep).
- Practise calming techniques like box breathing (4 seconds breathing in, 4 seconds holding, 4 seconds breathing out, 4 seconds holding)
Chronic insomnia (3+ nights/week for 3+ months) with significant daytime effects may require treatment like Cognitive Behavioral Therapy for Insomnia (CBT-I), so that’s a thing to bear in mind too.
In short: sleep isn’t just about being tired—it’s about working with your brain’s systems, not against them.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
How to Fall Asleep Faster: CBT-I Treatment For Insomnia
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: