Goji Berries vs Cherries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing goji berries to cherries, we picked the goji berries.
Why?
Looking at the macros first, goji berries have more protein, fiber, and carbs, as well as the lower glycemic index, although cherries are great too. Still, a clear and easy win here.
In the category of vitamins, goji berries have more of vitamins A and C, while cherries have more of vitamin K; in the other vitamins these two fruits are close enough to equal that variants in what kind of cherry it is will push it slightly one way or the other. However, it’s worth noting that goji berries have 1,991% more vitamin A and 16,033% more vitamin C, while cherries have only 20% more vitamin K. So, all in all, another clear win for goji berries.
When it comes to minerals, goji berries have more calcium and iron, while cherries have more copper. Again, the margins of difference are very much in goji berries’ favor, with 1,088% more calcium and 2,025% more iron, while cherries have 35% more copper. So, again, a win for goji berries.
The polyphenol contents of cherries differ far too much to comment here, but as a general rule of thumb, goji berries have more antioxidant powers than cherries, but cherries are also excellent for this.
In short, enjoy either or both, but goji berries are the more nutritionally dense!
Want to learn more?
You might like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Miracle of Flexibility – by Miranda Esmonde-White

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve reviewed books about stretching before, so what makes this one different?
Mostly, it’s that this one takes a holistic approach, making the argument for looking after all parts of flexibility (even parts that might seem useless) because if one bit of us isn’t flexible, the others will start to suffer in compensation because of how that affects our posture, or movement, or in many cases our lack of movement.
Esmonde-White’s “flexibility, from your toes to your shoulders” approach is very consistent with her background as a professional ballet dancer, and now she brings it into her profession as a coach.
The book’s not just about stretching, though. It looks at problems and what can go wrong with posture and the body’s “musculoskeletal trifecta”, and also shares daily training routines that are tailored for specific sporting interests, and/or for those with specific chronic conditions and/or chronic pain. Working around what needs to be worked around, but also looking at strengthening what can be strengthened and fixing what can be fixed along the way.
Bottom line: if your flexibility needs an overhaul, this book is a very good “one-stop shop” for that.
Click here to check out The Miracle Of Flexibility, and discover what you can do!
Share This Post
-

Stop Sabotaging Your Weight Loss – by Jennifer Powter, MSc
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is not a dieting book, and it’s not a motivational pep talk.
The book starts with the assumption that you do want to lose weight (it also assumes you’re a woman, and probably over 40… that’s just the book’s target market, but the same advice is good even if that’s not you), and that you’ve probably been trying, on and off, for a while. Her position is simple:
❝I don’t believe that you have a weight loss problem. I believe that you have a self-sabotage problem❞
As to how this sabotage may be occurring, Powter talks about fears that may be holding you back, including but not limited to:
- Fear of failure
- Fear of the unknown
- Fear of loss
- Fear of embarrassment
- Fear of your weight not being the reason your life sucks
Far from putting the reader down, though, Powter approaches everything with compassion. To this end, her prescription starts with encouraging self-love. Not when you’re down to a certain size, not when you’re conforming perfectly to a certain diet, but now. You don’t have to be perfect to be worthy of love.
On the topic of perfection: a recurring theme in the book is the danger of perfectionism. In her view, perfectionism is nothing more nor less than the most justifiable way to hold yourself back in life.
Lastly, she covers mental reframes, with useful questions to ask oneself on a daily basis, to ensure progressing step by step into your best life.
In short: if you’d like to lose weight and have been trying for a while, maybe on and off, this book could get you out of that cycle and into a much better state of being.
Get your copy of “Stop Sabotaging Your Weight Loss” from Amazon today!
Share This Post
-

Speedy Easy Ratatouille
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One of the biggest contributing factors to unhealthy eating? The convenience factor. To eat well, it seems, one must have at least two of the following: money, time, and skill. So today we have a health dish that’s cheap, quick, and easy!
(You won’t need a rat in a hat to help you with this one)
You will need
- 3 ripe tomatoes, roughly chopped
- 2 zucchini, halved and chopped into thick batons
- 2 portobello mushrooms, sliced into ½” slices
- 1 large red pepper, cut into thick chunks
- 3 tbsp extra virgin olive oil
- 2 tbsp finely chopped parsley
- 2 tsp garlic paste
- 2 tsp thyme leaves, destalked
- 1 tsp rosemary leaves, destalked
- 1 tsp red chili flakes
- 1 tsp black pepper
- Optional: 1 tsp MSG, or 1 tsp low sodium salt (the MSG is the healthier option as it contains less sodium than even low sodium salt)
- Optional: other vegetables, chopped. Use what’s in your fridge! This is a great way to use up leftovers. Particularly good options include chopped eggplant, chopped red onion, and/or chopped carrot.
Method
(we suggest you read everything at least once before doing anything)
1) Put the olive oil into a sauté pan and set the heat on medium. When hot but smoking, add the mushrooms and any optional vegetables (but not the others from the list yet), and fry for 5 minutes.
Note: if you aren’t pressed for time, then you can diverge from the “speedy” part of this by cooking each of the vegetables separately before combining, which allows each to keep its flavor more distinct.
2) Add the garlic, followed by the zucchini, red pepper, chili flakes, and thyme; stir periodically (you shouldn’t have to stir constantly) for 10 minutes.
3) Add the tomatoes and a cup of water to the pan, along with any MSG/salt. Cover with the lid and allow to simmer for a further 10 minutes.
4) Serve, adding the garnish.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Level-Up Your Fiber Intake! (Without Difficulty Or Discomfort)
- The Magic Of Mushrooms: “The Longevity Vitamin” (That’s Not A Vitamin)
- Our Top 5 Spices: How Much Is Enough For Benefits? ← we had 3/5 today!
- Monosodium Glutamate: Sinless Flavor-Enhancer Or Terrible Health Risk?
- MSG vs Salt: Sodium Comparison
Take care!
Share This Post


Related Posts
-

How To Leverage Placebo Effect For Yourself
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Placebo Effect: Making Things Work Since… Well, A Very Long Time Ago
The placebo effect is a well-known, well-evidenced factor that is very relevant when it comes to the testing and implementation of medical treatments:
NIH | National Center for Biotechnology Information | Placebo Effect
Some things that make placebo effect stronger include:
- Larger pills instead of small ones: because there’s got to be more going on in there, right?
- Thematically-colored pills: e.g. red for stimulant effects, blue for relaxing effects
- Things that seem expensive: e.g. a well-made large heavy machine, over a cheap-looking flimsy plastic device. Similarly, medication from a small glass jar with a childproof lock, rather than popped out from a cheap blister-pack.
- Things that seem rational: if there’s an explanation for how it works that you understand and find rational, or at least you believe you understand and find rational ← this works in advertising, too; if there’s a “because”, it lands better almost regardless of what follows the word “because”
- Things delivered confidently by a professional: this is similar to the “argument from authority” fallacy (whereby a proposed authority will be more likely trusted, even if this is not their area of expertise at all, e.g. celebrity endorsements), but in the case of placebo trials, this often looks like a well-dressed middle-aged or older man with an expensive haircut calling for a young confident-looking aide in a lab coat to administer the medicine, and is received better than a slightly frazzled academic saying “and, uh, this one’s yours” while handing you a pill.
- Things with ritual attached: this can be related to the above (the more pomp and circumstance is given to the administration of the treatment, the better), but it can also be as simple as an instruction on an at-home-trial medication saying “take 20 minutes before bed”. Because, if it weren’t important, they wouldn’t bother to specify that, right? So it must be important!
And now for a quick personality test
Did you see the above as a list of dastardly tricks to watch out for, or did you see the above as a list of things that can make your actual medication more effective?
It’s arguably both, of course, but the latter more optimistic view is a lot more useful than the former more pessimistic one.
Since placebo effect works at least somewhat even when you know about it, there is nothing to stop you from leveraging it for your own benefit when taking medication or doing health-related things.
Next time you take your meds or supplements or similar, pause for a moment for each one to remember what it is and what it will be doing for you. This is a lot like the principles (which are physiological as well as psychological) of mindful eating, by the way:
How To Get More Nutrition From The Same Food
Placebo makes some surprising things evidence-based
We’ve addressed placebo effect sometimes as part of an assessment of a given alternative therapy, often in our “Mythbusting Friday” edition of 10almonds.
- In some cases, placebo is adjuvant to the therapy, i.e. it is one of multiple mechanisms of action (example: chiropractic or acupuncture)
- In some cases, placebo is the only known mechanism of action (example: homeopathy)
- In some cases, even placebo can’t help (example: ear candling)
One other fascinating and far-reaching (in a potentially good way) thing that placebo makes evidence-based is: prayer
…which is particularly interesting for something that is fundamentally faith-based, i.e. the opposite of evidence-based.
Now, we’re a health science publication, not a theological publication, so we’ll consider actual divine intervention to be beyond the scope of mechanisms of action we can examine, but there’s been a lot of research done into the extent to which prayer is beneficial as a therapy, what things it may be beneficial for, and what factors affect whether it helps:
Prayer and healing: A medical and scientific perspective on randomized controlled trials
👆 full paper here, and it is very worthwhile reading if you have time, whether or not you are religious personally
Placebo works best when there’s a clear possibility for psychosomatic effect
We’ve mentioned before, and we’ll mention again:
- psychosomatic effect does not mean: “imagining it”
- psychosomatic effect means: “your brain regulates almost everything else in your body, directly or indirectly, including your autonomic functions, and especially notably when it comes to illness, your immune responses”
So, a placebo might well heal your rash or even shrink a tumor, but it probably won’t regrow a missing limb, for instance.
And, this is important: it’s not about how credible/miraculous the outcome will be!
Rather, it is because we have existing pre-programmed internal bodily processes for healing rashes and shrinking tumors, that just need to be activated—whereas we don’t have existing pre-programmed internal bodily processes for regrowing a missing limb, so that’s not something our brain can just tell our body to do.
So for this reason, in terms of what placebo can and can’t do:
- Get rid of cancer? Yes, sometimes—because the body has a process for doing that; enjoy your remission
- Fix a broken nail? No—because the body has no process for doing that; you’ll just have to cut it and wait for it to grow again
With that in mind, what will you use the not-so-mystical powers of placebo for? What ever you go for… Enjoy, and take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Eat Dirt – by Dr. Josh Axe
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Axe describes leaky gut as “a serious disease with a silly name”, and hopes for people to take increased intestinal permeability (as it is otherwise known) seriously, because it can be found at the root of very many diseases, especially inflammatory / autoimmune diseases, which obviously also has significant implications for dementia (of which neuroinflammation is a fair part of the pathogenesis) and cancer (which has been described as largely a matter of immune dysfunction).
He starts strong, albeit anecdotally, with the story of his own mother’s battle with cancer and other diseases, and how her health did a U-turn (for the better) upon taking care of her gut as per the methods described in this book. Dr. Axe doesn’t go so far as to claim the gut-healthy protocol cured her cancer, but makes the (very reasonable) argument that it was a major contributory factor, especially as it was the main input variable that changed.
The book describes the various things that can go wrong with our gut and why, and for each of them presents a solution.
Some of it is as you might guess from the title—live a little dirtier, because the ubiquity of antimicrobials is leaving our immune system slack and maladjusted, causing it to varyingly a) turn on us b) not rise to the occasion when an actual pathogen arrives c) often both. Other matters of consideration include normal gut health nutrition (prebiotics and probiotics, skipping inflammatory foods), matters of medication (especially those that harm the gut), nutraceuticals such as Boswellia serrata, and even stress management.
He provides a program so that the reader can follow along step-by-step, and even a chapter of recipes, but the greatest value in the book is the explanation of gut pathology—because understanding that is foundational to recognizing a lot of things (and he does provide diagnostic questionnaires also, which are helpful).
Bottom line: if you’d like to improve almost any aspect of your health, then your gut is almost always an excellent place to start, and this book will set you on the right path.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Qigong: A Breath Of Fresh Air?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Qigong: Breathing Is Good (Magic Remains Unverified)

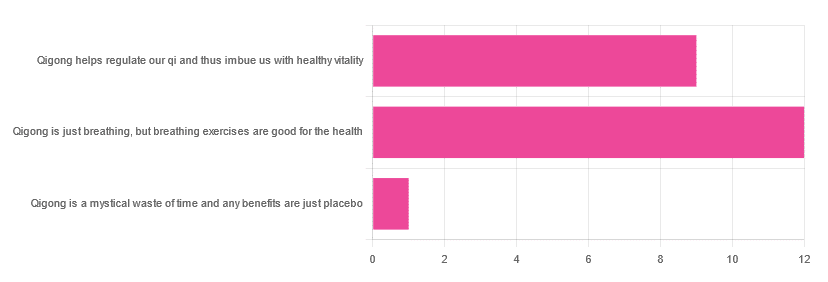
In Tuesday’s newsletter, we asked you for your opinions of qigong, and got the above-depicted, below-described, set of responses:
- About 55% said “Qigong is just breathing, but breathing exercises are good for the health”
- About 41% said “Qigong helps regulate our qi and thus imbue us with healthy vitality”
- One (1) person said “Qigong is a mystical waste of time and any benefits are just placebo”
The sample size was a little low for this one, but the results were quite clearly favorable, one way or another.
So what does the science say?
Qigong is just breathing: True or False?
True or False, depending on how we want to define it—because qigong ranges in its presentation from indeed “just breathing exercises”, to “breathing exercises with visualization” to “special breathing exercises with visualization that have to be exactly this way, with these hand and sometimes body movements also, which also must be just right”, to far more complex definitions that involve qi by various mystical definitions, and/or an appeal to a scientific analog of qi; often some kind of bioelectrical field or such.
There is, it must be said, no good quality evidence for the existence of qi.
Writer’s note, lest 41% of you want my head now: I’ve been practicing qigong and related arts for about 30 years and find such to be of great merit. This personal experience and understanding does not, however, change the state of affairs when it comes to the availability (or rather, the lack) of high quality clinical evidence to point to.
Which is not to say there is no clinical evidence, for example:
Acute Physiological and Psychological Effects of Qigong Exercise in Older Practitioners
…found that qigong indeed increased meridian electrical conductance!
Except… Electrical conductance is measured with galvanic skin responses, which increase with sweat. But don’t worry, to control for that, they asked participants to dry themselves with a towel. Unfortunately, this overlooks the fact that a) more sweat can come where that came from, because the body will continue until it is satisfied of adequate homeostasis, and b) drying oneself with a towel will remove the moisture better than it’ll remove the salts from the skin—bearing in mind that it’s mostly the salts, rather than the moisture itself, that improve the conductivity (pure distilled water does conduct electricity, but not very well).
In other words, this was shoddy methodology. How did it pass peer review? Well, here’s an insight into that journal’s peer review process…
❝The peer-review system of EBCAM is farcical: potential authors who send their submissions to EBCAM are invited to suggest their preferred reviewers who subsequently are almost invariably appointed to do the job. It goes without saying that such a system is prone to all sorts of serious failures; in fact, this is not peer-review at all, in my opinion, it is an unethical sham.❞
~ Dr. Edzard Ernst, a founding editor of EBCAM (he since left, and decries what has happened to it since)
One of the other key problems is: how does one test qigong against placebo?
Scientists have looked into this question, and their answers have thus far been unsatisfying, and generally to the tune of the true-but-unhelpful statement that “future research needs to be better”:
Problems of scientific methodology related to placebo control in Qigong studies: A systematic review
Most studies into qigong are interventional studies, that is to say, they measure people’s metrics (for example, blood pressure, heart rate, maybe immune function biomarkers, sleep quality metrics of various kinds, subjective reports of stress levels, physical biomarkers of stress levels, things like that), then do a course of qigong (perhaps 6 weeks, for example), then measure them again, and see if the course of qigong improved things.
This almost always results in an improvement when looking at the before-and-after, but it says nothing for whether the benefits were purely placebo.
We did find one study that claimed to be placebo-controlled:
…but upon reading the paper itself carefully, it turned out that while the experimental group did qigong, the control group did a reading exercise. Which is… Saying how well qigong performs vs reading (qigong did outperform reading, for the record), but nothing for how well it performs vs placebo, because reading isn’t a remotely credible placebo.
See also: Placebo Effect: Making Things Work Since… Well, A Very Long Time Ago ← this one explains a lot about how placebo effect does work
Qigong is a mystical waste of time: True or False?
False! This one we can answer easily. Interventional studies invariably find it does help, and the fact remains that even if placebo is its primary mechanism of action, it is of benefit and therefore not a waste of time.
Which is not to say that placebo is its only, or even necessarily primary, mechanism of action.
Even from a purely empirical evidence-based medicine point of view, qigong is at the very least breathing exercises plus (usually) some low-impact body movement. Those are already two things that can be looked at, mechanistic processes pointed to, and declarations confidently made of “this is an activity that’s beneficial for health”.
See for example:
- Effects of Qigong practice in office workers with chronic non-specific low back pain: A randomized control trial
- Qigong for the Prevention, Treatment, and Rehabilitation of COVID-19 Infection in Older Adults
- Impact of Medical Qigong on quality of life, fatigue, mood and inflammation in cancer patients: a randomized controlled trial
…and those are all from respectable journals with meaningful peer review processes.
None of them are placebo-controlled, because there is no real option of “and group B will only be tricked into believing they are doing deep breathing exercises with low-impact movements”; that’s impossible.
But! They each show how doing qigong reliably outperforms not doing qigong for various measurable metrics of health.
And, we chose examples with physical symptoms and where possible empirically measurable outcomes (such as COVID-19 infection levels, or inflammatory responses); there are reams of studies showings qigong improves purely subjective wellbeing—but the latter could probably be claimed for any enjoyable activity, whereas changes in inflammatory biomarkers, not such much.
In short: for most people, it indeed reliably helps with many things. And importantly, it has no particular risks associated with it, and it’s almost universally framed as a complementary therapy rather than an alternative therapy.
This is critical, because it means that whereas someone may hold off on taking evidence-based medicines while trying out (for example) homeopathy, few people are likely to hold off on other treatments while trying out qigong—since it’s being viewed as a helper rather than a Hail-Mary.
Want to read more about qigong?
Here’s the NIH’s National Center for Complementary and Integrative Health has to say. It cites a lot of poor quality science, but it does mention when the science it’s citing is of poor quality, and over all gives quite a rounded view:
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: