MSG vs. Salt: Sodium Comparison
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Q: Is MSG healthier than salt in terms of sodium content or is it the same or worse?
Great question, and for that matter, MSG itself is a great topic for another day. But your actual question, we can readily answer here and now:
- Firstly, by “salt” we’re assuming from context that you mean sodium chloride.
- Both salt and MSG do contain sodium. However…
- MSG contains only about a third of the sodium that salt does, gram-for-gram.
- It’s still wise to be mindful of it, though. Same with sodium in other ingredients!
- Baking soda contains about twice as much sodium, gram for gram, as MSG.
Wondering why this happens?
Salt (sodium chloride, NaCl) is equal parts sodium and chlorine, by atom count, but sodium’s atomic mass is lower than chlorine’s, so 100g of salt contains only 39.34g of sodium.
Baking soda (sodium bicarbonate, NaHCO₃) is one part sodium for one part hydrogen, one part carbon, and three parts oxygen. Taking each of their diverse atomic masses into account, we see that 100g of baking soda contains 27.4g sodium.
MSG (monosodium glutamate, C₅H₈NO₄Na) is only one part sodium for 5 parts carbon, 8 parts hydrogen, 1 part nitrogen, and 4 parts oxygen… And all those other atoms put together weigh a lot (comparatively), so 100g of MSG contains only 12.28g sodium.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

You’re Not Forgetful: How To Remember Everything

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Elizabeth Filips, medical student busy learning a lot of information, explains how in today’s video:
Active processing
An important thing to keep in mind is that forgetting is an active process, not passive as once believed. It has its own neurotransmitters and pathways, and as such, to improve memory, it’s essential to understand and manage forgetting.
So, how does forgetting occur? Memories are stored with cues or tags, which help retrieve information. However, overloading cues with too much information can cause “transient forgetting”—that is to say, the information is still in there somewhere; you just don’t have the filing system required to retrieve the data. This is the kind of thing that you will try hard to remember at some point in the day when you need it, fail, and then wake up at 3am with an “Aha!” because your brain finally found what you were looking for. So, to avoid that, use unique and strong cues to help improve recall (mnemonics are good for this, as are conceptual anchors).
While memory does not appear to actually be finite, there is some practical truth in the “finite storage” model insofar as learning new information can overwrite previous knowledge, iff your brain mistakes it for an update rather than addition. So for that reason, it’s good to periodically go over old information—in psychology this is called rehearsal, which may conjure theatrical images, but it can be as simple as mentally repeating a phone number, a mnemonic, or visually remembering a route one used to take to go somewhere.
Self-perception affects memory performance. Negative beliefs about one’s memory can worsen performance (so don’t say “I have a bad memory”, even to yourself, and in contrast, find more positive affirmations to make about your memory), and mental health in general plays a significant role in memory. For example, if you have ever had an extended period of depression, then chances are good you have some huge gaps in your memory for that time in your life.
A lot of what we learned in school was wrong—especially what we learned about learning. Traditional (vertical) learning is harder to retain, whereas horizontal learning (connecting topics through shared characteristics) creates stronger, interconnected memories. In short, your memories should tell contextual stories, not be isolated points of data.
Embarking on a new course of study? Yes? (If not, then why not? Pick something!)
It may be difficult at first, but experts memorize things more quickly due to built-up intuition in their field. For example a chess master can glance at a chess board for about 5 seconds and memorize the position—but only if the position is one that could reasonably arise in a game; if the pieces are just placed at random, then their memorization ability plummets to that of the average person, because their expertise has been nullified.
What this means in practical terms: building a “skeleton” framework before learning can enhance memorization through logical connections. For this reason, if embarking on a serious course of study, getting a good initial overview when you start is critical, so that you have a context for the rest of what you learn to go into. For example, let’s say you want to learn a language; if you first quickly do a very basic bare-bones course, such as from Duolingo or similar, then even though you’ll have a very small vocabulary and a modest grasp of grammar and make many mistakes and have a lot of holes in your knowledge, you now have somewhere to “fit” every new word or idea you learn. Same goes for other fields of study; for example, a doctor can be told about a new drug and remember everything about it immediately, because they understand the systems it interacts with, understand how it does what it does, and can compare it mentally to similar drugs, and they thus have a “place” in that overall system for the drug information to reside. But for someone who knows nothing about medicine, it’s just a lot of big words with no meaning. So: framework first, details later.
For more on all this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
How To Boost Your Memory Immediately (Without Supplements)
Take care!
Share This Post
-
3 Standing Abs Exercises You’ll Actually Feel Tomorrow
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to ab exercises, not everyone loves spending time on the floor. So, what else is there?
On your feet
The three exercises she recommends are:
- Kettlebell “around the world”: hold a light kettlebell and pass it around your waist in a circular motion, switching hands in front and back. Perform in both directions to improve core stability, coordination, and balance.
- Overhead carry with knee raise: hold one or two dumbbells overhead and alternate raising your knees. Keep your pelvis slightly forward to engage your core, not your hip flexors. Do it stationary, or walking to build extra core and shoulder stability.
- Dumbbell “wood chopper”: swing a dumbbell diagonally across your body using hip rotation. This rotational movement engages the obliques and improves spine flexibility, balance, and total-body coordination.
For more on each of these plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Is A Visible Six-Pack Obtainable Regardless Of Genetic Predisposition?
Take care!
Share This Post
-

Heal Your Nervous System – by Dr. Linnea Passaler
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This book focuses on the oft-overlooked connection between nervous system dysregulation (i.e. sympathetic nervous system dominance, keeping the brain in “may have to fight for my life at any moment” mode) and the many symptoms—mental and physical—that can arise as a result.
While there is a lot of theory explained in here, there’s practicality too, providing the reader with tools to assess our own levels of nervous system dysregulation and what factors affect that.
In particular in that category, a lot of value is delivered in terms of practical guidance on avoiding common pitfalls in the healing journey. Dr. Passaler discusses the four biggest mistakes people make when attempting to heal, and gives clear strategies to sidestep each of them, with exercises to do and habits to implement.
Another thing that sets this book apart from many of its genre is her emphasis on the importance of sequencing healing practices in the right order. By offering a structured approach, the book helps us implement healing practices without getting overwhelmed or hitting the proverbial brick wall and getting frustrated, which makes a big difference.
The style is easy-to-understand pop-science, albeit with a reassuring 20 pages of references at the back.
Bottom line: if you feel like “peace of mind” is something that’s always just out of reach, this book can help you to get where you need to be, physically as well as mentally.
Click here to check out Heal Your Nervous System, and get things into much better order!
Share This Post


Related Posts
-

Eggs: Nutritional Powerhouse or Heart-Health Timebomb?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Eggs: All Things In Moderation?

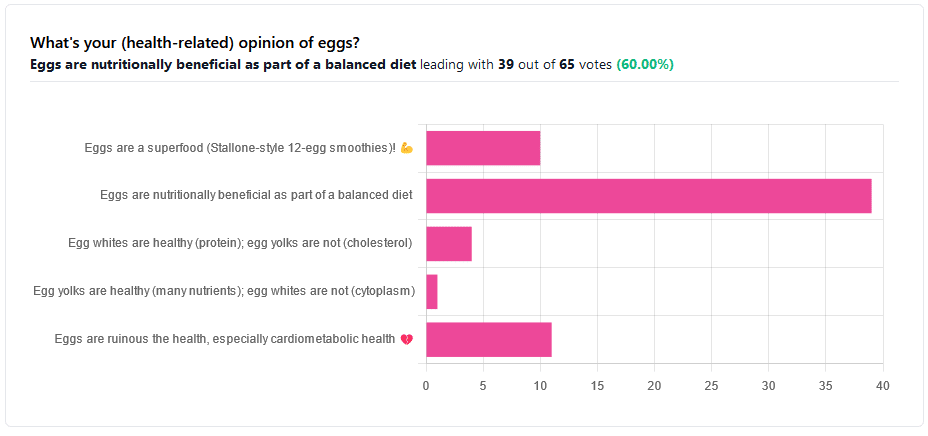
We asked you for your (health-related) opinion on eggs. We specified that, for the sake of simplicity, let’s say that they are from happy healthy backyard hens who enjoy a good diet.
Apparently this one wasn’t as controversial as it might have been! We (for myth-busting purposes) try to pick something polarizing and sometimes even contentious for our Friday editions, and pick apart what science lies underneath public perceptions.
However, more than half (in fact, 60%) of the subscribers who voted in the poll voted for “Eggs are nutritionally beneficial as part of a balanced diet”, which very moderate statement is indeed pretty much the global scientific consensus.
Still, we’ve a main feature to write, so let’s look at the science, and what the other 40% had in mind:
Eggs are ruinous to health, especially cardiometabolic health: True or False?
False, per best current science, anyway!
Scientific consensus has changed over the years. We learned about cholesterol, then we learned about different types of cholesterol, and now we’ve even learned about in some instances even elevated levels of “bad” cholesterol aren’t necessarily a cause of cardiometabolic disorders so much as a symptom—especially in women.
Not to derail this main feature about eggs (rather than just cholesterol), but for those who missed it, this is actually really interesting: basically, research (pertaining to the use of statins) has found that in women, higher LDL levels aren’t anywhere near the same kind of risk factor as they are for men, and thus may mean that statins (whose main job is reducing LDL) may be much less helpful for women than for men, and more likely to cause unwanted serious side effects in women.
Check out our previous main feature about this: Statins: His & Hers?
But, for back on topic, several large studies (totalling 177,000 people in long-term studies in 50 countries) found:
❝Results from the three cohorts and from the updated meta-analysis show that moderate egg consumption (up to one egg per day) is not associated with cardiovascular disease risk overall, and is associated with potentially lower cardiovascular disease risk in Asian populations.❞
Egg whites are healthy (protein); egg yolks are not (cholesterol): True or False?
True and False, respectively. That is to say, egg whites are healthy (protein), and egg yolks are also healthy (many nutrients).
We talked a bit already about cholesterol, so we’ll not rehash that here. As to the rest:
Eggs are one of the most nutritionally dense foods around. After all, they have everything required to allow a cluster of cells to become a whole baby chick. That’s a lot of body-building!
They’re even more nutritionally heavy-hitters if you get omega-3 enriched eggs, which means the hens were fed extra omega-3, usually in the form of flax seeds.
Also, free-range is better healthwise than others. Do bear in mind that unless they really are from your backyard, or a neighbor’s, chances are that the reality is not what the advertising depicts, though. There are industry minimum standards to be able to advertise as “free-range”, and those standards are a) quite low b) often ignored, because an occasional fine is cheaper than maintaining good conditions.
So if you can look after your own hens, or get them from somewhere that you can see for yourself how they are looked after, so much the better!
Check out the differences side-by-side, though:
Pastured vs Omega-3 vs “Conventional” Eggs: What’s the Difference?
Stallone-style 12-egg smoothies are healthy: True or False?
False, at least if taken with any regularity. One can indeed have too much of a good thing.
So, what’s the “right amount” to eat?
It may vary depending on individual factors (including age and ethnicity), but a good average, according to science, is to keep it to 3 eggs or fewer per day. There are a lot of studies, but we only have so much room here, so we’ll pick one. Its findings are representative of (and in keeping with) the many other studies we looked at, so this seems uncontroversial scientifically:
❝Intake of 1 egg/d was sufficient to increase HDL function and large-LDL particle concentration; however, intake of 2-3 eggs/d supported greater improvements in HDL function as well as increased plasma carotenoids. Overall, intake of ≤3 eggs/d favored a less atherogenic LDL particle profile, improved HDL function, and increased plasma antioxidants in young, healthy adults.❞
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Dandelion Greens vs Collard Greens – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing dandelion greens to collard greens, we picked the dandelion greens.
Why?
Collard greens are great—they even beat kale in one of our previous “This or That” articles!—but dandelion greens simply pack more of a nutritional punch:
In terms of macros, dandelions have slightly more carbs (+3g/100g) for the same protein and fiber, and/but the glycemic index is equal (zero), so those carbs aren’t anything to worry about. Nobody is getting metabolic disease by getting their carbs from dandelion leaves. In short, we’re calling it a tie on macros, though it could nominally swing either way if you have an opinion (one way or the other) about the extra 3g of carbs.
In the category of vitamins, things are more exciting: dandelion greens have more of vitamins A, B1, B2, B3, B6, B7, B9, C, E, and K, while collard greens have more vitamin B5. An easy and clear win for dandelions.
Looking at the minerals tells a similar story; dandelion greens have much more calcium, copper, iron, magnesium, phosphorus, potassium, and zinc, while collard greens have slightly more manganese. Another overwhelming win for dandelions.
One more category, polyphenols. We’d be here until next week if we listed all the polyphenols that dandelion greens have, but suffice it to say, dandelion greens have a total of 385.55mg/100g polyphenols, while collard greens have a total of 0.08mg/100g polyphenols. Grabbing a calculator, we see that this means dandelions have more than 4819x the polyphenol content that collard greens do.
So, “eat leafy greens” is great advice, but they are definitely not all created equal!
Let us take this moment to exhort: if you have any space at home where you can grow dandelions, grow them!
Not only are they great for pollinators, but also they beat the collard greens that beat kale. And you can have as much as you want, for free, right there.
Want to learn more?
You might like to read:
Collard Greens vs Kale – Which is Healthier?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Plant Power Doctor
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A Prescription For GLOVES

This is Dr. Gemma Newman. She’s a GP (General Practitioner, British equivalent to what is called a family doctor in America), and she realized that she was treating a lot of patients while nobody was actually getting better.
So, she set out to help people actually get better… But how?
The biggest thing
The single biggest thing she recommends is a whole foods plant-based diet, as that’s a starting point for a lot of other things.
Click here for an assortment of short videos by her and other health professionals on this topic!
Specifically, she advocates to “love foods that love you back”, and make critical choices when deciding between ingredients.
Click here to see her recipes and tips (this writer is going to try out some of these!)
What’s this about GLOVES?
We recently reviewed her book “Get Well, Stay Well: The Six Healing Health Habits You Need To Know”, and now we’re going to talk about those six things in more words than we had room for previously.
They are six things that she says we should all try to get every day. It’s a lot simpler than a lot of checklists, and very worthwhile:
Gratitude
May seem like a wishy-washy one to start with, but there’s a lot of evidence for this making a big difference to health, largely on account of how it lowers stress and anxiety. See also:
How To Get Your Brain On A More Positive Track (Without Toxic Positivity)
Love
This is about social connections, mostly. We are evolved to be a social species, and while some of us want/need more or less social interaction than others, generally speaking we thrive best in a community, with all the social support that comes with that. See also:
How To Beat Loneliness & Isolation
Outside
This is about fresh air and it’s about moving and it’s about seeing some green plants (and if available, blue sky), marvelling at the wonder of nature and benefiting in many ways. See also:
Vegetables
We spoke earlier about the whole foods plant-based diet for which she advocates, so this is that. While reducing/skipping meat etc is absolutely a thing, the focus here is on diversity of vegetables; it is best to make a game of seeing how many different ones you can include in a week (not just the same three!). See also:
Three Critical Kitchen Prescriptions
Exercise
At least 150 minutes moderate exercise per week, and some kind of resistance work. It can be calisthenics or something; it doesn’t have to be lifting weights if that’s not your thing! See also:
Resistance Is Useful! (Especially As We Get Older)
Sleep
Quality and quantity. Yes, 7–9 hours, yes, regardless of age. Unless you’re a child or a bodybuilder, in which case make it nearer 12. But for most of us, 7–9. See also:
Why You Probably Need More Sleep
Want to know more?
As well as the book we mentioned earlier, you might also like:
The Plant Power Doctor – by Dr. Gemma Newman
While the other book we mentioned is available for pre-order for Americans (it’s already released for the rest of the world), this one is available to all right now, so that’s a bonus too.
If books aren’t your thing (or even if they are), you might like her award-winning podcast:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: