The Sweet Truth About Glycine
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Make Your Collagen Work Better
This is Dr. James Nicolantonio. He’s a doctor of pharmacy, and a research scientist. He has a passion for evidence-based nutrition, and has written numerous books on the subject.
Controversy! Dr. DiNicolatonio’s work has included cardiovascular research, in which field he has made the case for increasing (rather than decreasing) the recommended amount of salt in our diet. This, of course, goes very much against the popular status quo.
We haven’t reviewed that research so we won’t comment on it here, but we thought it worth a mention as a point of interest. We’ll investigate his claims in that regard another time, though!
Today, however, we’ll be looking at his incisive, yet not controversial, work pertaining to collagen and glycine.
A quick recap on collagen
We’ve written about collagen before, and its importance for maintaining… Well, pretty much most of our body, really, buta deficiency in collagen can particularly weaken bones and joints.
On a more surface level, collagen’s also important for healthy elastic skin, and many people take it for that reason alone,
Since collagen is found only in animals, even collagen supplements are animal-based (often marine collagen or bovine collagen). However, if we don’t want to consume those, we can (like most animals) synthesize it ourselves from the relevant amino acids, which we can get from plants (and also laboratories, in some cases).
You can read our previous article about this, here:
We Are Such Stuff As Fish Are Made Of
What does he want us to know about collagen?
We’ll save time and space here: first, he’d like us to know the same as what we said in our article above
However, there is also more:
Let’s assume that your body has collagen to process. You either consumed it, or your body has synthesized it. We’ll skip describing the many steps of collagen synthesis, fascinating as that is, and get to the point:
When our body weaves together collagen fibrils out of the (triple-helical) collagen molecules…
- the cross-linking of the collagen requires lysyl oxidase
- the lysyl oxidase (which we make inside us) deanimates some other amino acids yielding aldehydes that allow the stable cross-links important for the high tensile strength of collagen, but to do that, it requires copper
- in order to use the copper it needs to be in its reduced cuprous form and that requires vitamin C
- but moving it around the body requires vitamin A
So in other words: if you are taking (or synthesizing) collagen, you also need copper and vitamins A and C.
However! Just to make things harder, if you take copper and vitamin C together, it’ll reduce the copper too soon in the wrong place.
Dr. DiNicolantonio therefore advises taking vitamin C after copper, with a 75 minutes gap between them.
What does he want us to know about glycine?
Glycine is one of the amino acids that makes up collagen. Specifically, it makes up every third amino acid in collagen, and even more specifically, it’s also the rate-limiting factor in the formation of glutathione, which is a potent endogenous (i.e., we make it inside us) antioxidant that works hard to fight inflammation inside the body.
What this means: if your joints are prone to inflammation, being glycine-deficient means a double-whammy of woe.
As well as being one of the amino acids most key to collagen production, glycine has another collagen-related role:
First, the problem: as we age, glycated collagen accumulates in the skin and cartilage (that’s bad; there is supposed to be collagen there, but not glycated).
More on glycation and what it is and why it is so bad:
Are You Eating Advanced Glycation End-Products? The Trouble Of The AGEs
Now, the solution: glycine suppresses advanced glycation end products, including the glycation of collagen.
See for example:
With these three important functions of glycine in mind…
Dr. DiNicolantonio therefore advises getting glycine at a dose of 100mg/kg/day. So, if you’re the same size as this rather medium-sized writer, that means 7.2g/day.
Where can I get it?
Glycine is found in many foods, including gelatin for those who eat that, eggs for the vegetarians, and spinach for vegans.
However, if you’d like to simply take it as a supplement, here’s an example product on Amazon
(the above product is not clear whether it’s animal-derived or not, so if that’s important to you, shop around. This writer got some locally that is certified vegan, but is in Europe rather than N. America, which won’t help most of our subscribers)
Note: pure glycine is a white crystalline powder that has the same sweetness as glucose. Indeed, that is how it got its name, from the Greek “γλυκύς”, pronounced /ɡly.kýs/, meaning “sweet”. Yes, same etymology as glucose.
So don’t worry that you’ve been conned if you order it and think “this is sugar!”; it just looks and tastes the same.
That does mean you should buy from a reputable source though, as a con would be very easy!
this does also mean that if you like a little sugar/sweetener in your tea or coffee, glycine can be used as a healthy substitute.
If you don’t like sweet tastes, then, condolences. This writer pours two espresso coffees (love this decaffeinated coffee that actually tastes good), puts the glycine in the first, and then uses the second to get rid of the sweet taste of the first. So that’s one way to do it.
Enjoy (if you can!)
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

This Week In Brain News

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
While reading this week’s health news, we’ve singled out three brain-related articles to feature here:
Bad breath now, bad brain later?
Researchers found links between oral microbiome populations, and changes in brain function with aging. The short version is indeed “bad breath now = bad brain later”, but more specifically:
- People who had large numbers of the bacteria groups Neisseria and Haemophilus had better memory, attention and ability to do complex tasks
- People who had higher levels of Porphyromonas had more memory problems later
- People with a lot of Prevotella tended to predict poorer brain health and was more common in people who carry the Alzheimer’s Disease risk gene, APOE4.
If you’ve never heard of half of those, don’t worry: mostly your oral microbiome can take care of itself, provide you consistently do the things that create a “good” oral microbiome. So, see our “related” link below:
Read in full: Mouth bacteria may hold insight into your future brain function
Related: Improve Your Oral Microbiome
Weeding out a major cause of cognitive decline
Cannabis may be great for relaxation, but regular use is not great for mental sharpness, and recent use (even if not regular, and even if currently sober) shows a similar dip in cognitive abilities, especially working memory. In other words, cannabis use for relaxation should be at most an occasional thing, rather than an everyday thing.
While the results of the study are probably not shocking, something that we found interesting was their classification system:
❝Heavy users are considered young adults who’ve used cannabis more than 1000 times over their lifetime. Whereas, using 10 to 999 times was considered a moderate user, and fewer than 10 times was considered a non-user.❞
Which—while being descriptive rather than prescriptive in nature—suggests that, to be on the healthy end of the bell curve, an occasional cannabis-user might want to consider “if you have 999 uses before you hit the “heavy user” category, project those 999 uses against your life expectancy, and moderate your use accordingly”. In other words, a person just now starting use, who expects to live another 40 years, would calculate: 999/40 = 24.9 uses per year, so call it 2 per month. A person who only expects to live another 20 years, would do the same math and arrive at 4 per month.
Disclaimer: the above is intended as an interesting reframe, and a way of looking at long-term cannabis use while being mindful of the risks. It is not intended as advice. This health-conscious writer personally has no intention of using at all, unless perhaps in some bad future scenario in which I have bad chronic pain, I might consider that pain relief effects may be worth the downsides. Or I might not; I hope not to be in the situation to find out!
Read in full: Largest study ever done on cannabis and brain function finds impact on working memory
Related: Cannabis Myths vs Reality
Mind-reading technology improves again
We’ve come quite a way from simple 1/0 reads, and basic cursor control! Now, researchers have created a brain decode that can translate a person’s thoughts into continuous text, without requiring the person to focus on words—in other words, it verbalizes the ideas directly. Most recently, the latest upgrade means that while previously, the device had to be trained on an individual brain for many hours, now the training/calibration process takes only an hour:
Read in full: Improved brain decoder holds promise for communication in people with aphasia
Related: Are Brain Chips Safe?
Take care!
Share This Post
-

Pistachios vs Pecans – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing pistachios to pecans, we picked the pistachios.
Why?
Firstly, the macronutrients: pistachios have twice as much protein and fiber. Pecans have more fat, though in both of these nuts the fats are healthy.
The category of vitamins is an easy win for pistachios, with a lot more of vitamins A, B1, B2, B3, B6, B9, C, and E. Especially the 8x vitamin A, 7x vitamin B6, 4x vitamin C, and 2x vitamin E, and as the percentages are good too, these aren’t small differences. Pecans, meanwhile, boast only a little more vitamin B5 (pantothenic acid, the one whose name means “it’s everywhere”, because that’s how easy it is to get it).
In terms of minerals, pistachios have more calcium, iron, phosphorus, potassium, and selenium, while pecans have more manganese and zinc. So, a fair win for pistachios on this one.
Adding up the three different kinds of win for pistachios means that *drumroll* pistachios win overall, and it’s not close.
As ever, do enjoy both though, because diversity is healthy!
Want to learn more?
You might like to read:
Take care!
Share This Post
-

How we can prepare for future public health emergencies
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The U.S. is experiencing an increasing number of disease outbreaks and extreme weather events. While state and national preparedness for public health emergencies has improved in some areas, dangerous gaps remain, says a recent report from Trust for America’s Health.
Titled, “Ready or Not 2024: Protecting the Public’s Health from Diseases, Disasters, and Bioterrorism,” the report identifies gaps in national and state preparedness for public health emergencies and provides recommendations for improvement.
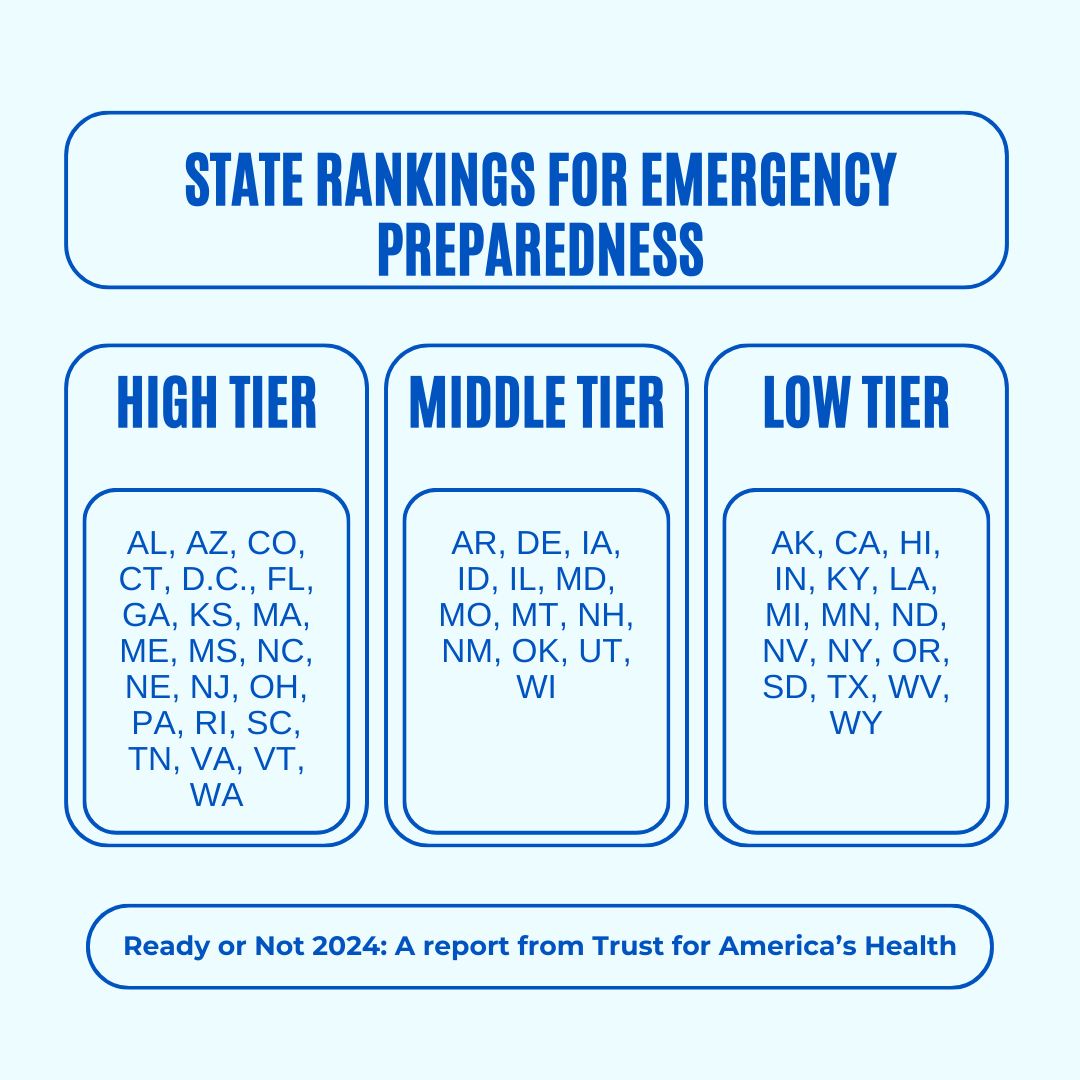
Using nine key indicators, the report categorizes all U.S. states and the District of Columbia into three readiness levels: high, medium, and low. The writers hope the report will help policymakers in under-performing states improve public health infrastructure.
Read on to learn more about what the research found and how we can individually prepare for future public health emergencies.
There’s work to be done

The report highlights areas with strong performance as well as those that need improvement.
Some areas with strong performance:
- State public health funding: Most states and the District of Columbia either maintained or increased their public health funding during the 2023 fiscal year.
- Health care labor force preparedness: Most states have started expanding the health care labor force for improved emergency response. As of 2023, 39 states participated in the Nurse Licensure Compact, which allows nurses to work in multiple member states without the need for additional state licenses.
Some areas that need improvement:
- Hospital safety scores: Only 25 percent of acute care hospitals earned the highest patient safety grade in fall 2023. These scores measure health care-associated infection rates, intensive care unit capacity, and other metrics. More high-scoring hospitals would improve preparedness for future public health emergencies.
- Access to paid time off: From March 2018 to March 2023, only 55 percent of U.S. workers used paid time off. Access to paid time off is important for reducing the spread of infectious diseases.
We can all do our part by staying up to date on vaccines
While the report focuses on policy changes that would improve emergency preparedness, Trust for America’s Health’s research identifies one way that we can individually prepare for future public health emergencies: staying up to date on vaccines.
The report found that during the 2022-2023 flu season, only 49 percent of those eligible for the flu vaccine received it. Public health experts are concerned that false claims about COVID-19 vaccines have resulted in overall vaccine hesitancy.
A decline in vaccination rates has led to an uptick in life-threatening, vaccine-preventable diseases, such as measles. Increasing vaccine uptake would prevent the spread of vaccine-preventable diseases and reduce strain on hospital systems during public health crises.
Make sure that you and your children have received all recommended vaccines to prevent severe illness, hospitalization, and death. Learn more about recommended vaccines for adults and children from the CDC.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Share This Post

Related Posts
-
Pomegranate vs Figs – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing pomegranate to figs, we picked the pomegranate.
Why?
In terms of macros, pomegranate has a lot more protein* and fiber, while the fig has more carbs. Thus, a win for pomegranate.
*Why such protein in a fruit? In both cases, it’s mostly from the seeds, which in both cases, we’re eating. However, pomegranates have a much greater seed-to-mass ratio than figs, and thus, a correspondingly higher amount of protein. Also some fats from the seeds, again more than figs, but the margin of difference is smaller, and not really enough to be of relevance.
In the category of vitamins, pomegranates lead with more of vitamins B1, B5, B9, C, E, K, and choline, while figs have more of vitamins A, B3, and B6. The largest margins of difference are in vitamins B9, E, and K, so all in pomegranate’s favor.
The minerals scene is closer to even; pomegranate has more copper, phosphorus, potassium, selenium, and zinc, while figs have more calcium, iron, magnesium, and manganese. Thus, a 5:4 lead for pomegranate, and the larger margins of difference are again for pomegranate.
In short, enjoy both, but pomegranates are the more nutritionally dense. Also, don’t throw away the peel! Dry it, and turn it into a powdered supplement—see our linked article below, for why:
Want to learn more?
You might like to read:
Pomegranate’s Health Gifts Are Mostly In Its Peel
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Power of Self-Care – by Dr. Sunil Kumar
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, what this book is mostly not about: bubble baths and scented candles. We say “mostly”, because stress management is an important aspect given worthy treatment in this book, but there is more emphasis on evidence-based interventions and thus Dr. Kumar is readier to prescribe nature walks and meditation, than product-based pampering sessions.
As is made clear in the subtitle “Transforming Heart Health with Lifestyle Medicine”, the focus is on heart health throughout, but as 10almonds readers know, “what’s good for your heart is good for your brain” is a truism that indeed holds true here too.
Dr. Kumar also gives nutritional tweaks to optimize heart health, and includes a selection of heart-healthy recipes, too. And exercise? Yes, customizable exercise plans, even. And a plan for getting sleep into order if perchance it has got a bit out of hand (most people get less sleep than necessary for maintenance of good health), and he even delves into “social prescribing”, that is to say, making sure that one’s social connectedness does not get neglected—without letting it, conversely, take over too much of one’s life (done badly, social connectedness can be a big source of unmanaged stress).
Perhaps the most value of this book comes from its 10-week self-care plan (again, with a focus on heart health), basically taking the reader by the hand for long enough that, after those 10 weeks, habits should be quite well-ingrained.
A strong idea throughout is that the things we take up should be sustainable, because well, a heart is for life, not just for a weekend retreat.
Bottom line: if you’d like to improve your heart health in a way that feels like self-care rather than an undue amount of work, then this is the book for you.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Brain Food – by Dr. Lisa Mosconi
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We know that we should eat for brain health, but often that knowledge doesn’t go a lot further than “we should eat some nuts… but also not the wrong nuts, which would be bad”.
However, as Dr. Lisa Mosconi lays out for us, there’s a lot more than that!
This book is as much a treatise of brain health in the context of nutrition, as it is a “eat this and avoid that” guide.
Which is good, because our brains don’t exist in isolation, and nor do the nutrients that we consume. Put it this way:
We have a tendecy to think of our diets as a set of slider-bars, “ok, that’s 104% of my daily intake of fiber, I need another 10g protein and that’ll be at 100%, I’ve had 80% of the vitamin C that I need, and…”
Whereas in reality: much of what we eat interacts positively or negatively with other things, and thus needs to be kept in balance. And not only that, but other peri-nutritional factors play a big part too! From obvious things like hydration, to less obvious things like maintaining good gut microbiota, our brains rely on us to do a lot of things for them.
This book is very easy-reading, though a weakness is it doesn’t tend to summarise key ideas much, give cheat-sheets, that sort of thing. We recommend reading this book with a notebook to the side, to jot down things you want to attend to in your own dietary habits.
Bottom line: this is an excellent overview of brain health in the context of nutrition, and is more comprehensive than most “eat this for good brain health and avoid that” books.
Click here to check out “Brain Food” on Amazon and treat your brain like it deserves!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: