
What’s Your Ikigai?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Ikigai: A Closer Look
We’ve mentioned ikigai from time to time, usually when discussing the characteristics associated with Blue Zone centenarians, for example as number 5 of…
It’s about finding one’s “purpose”. Not merely a function, but what actually drives you in life. And, if Japanese studies can be extrapolated to the rest of the world, it has a significant and large impact on mortality (other factors being controlled for); not having a sense of ikigai is associated with an approximately 47%* increase in 7-year mortality risk in the categories of cardiovascular disease and external cause mortality:
Sense of life worth living (ikigai) and mortality in Japan: Ohsaki Study
*we did a lot of averaging and fuzzy math to get this figure; the link will show you the full stats though!
In case that huge (n=43,391) study didn’t convince you, here’s another comparably-sized (n=43,117) one that found similarly, albeit framing the numbers the other way around, i.e. a comparable decrease in mortality risk for having a sense of ikigai:
This study was even longer (12 years rather than 7), so the fact that it found pretty much the same results the 7-year study we cited just before is quite compelling evidence. Again, multivariate hazard ratios were adjusted for age, BMI, drinking and smoking status, physical activity, sleep duration, education, occupation, marital status, perceived mental stress, and medical history—so all these things were effectively controlled for statistically.
Three kinds of ikigai
There are three principal kinds of ikigai:
- Social ikigai: for example, a caring role in the family or community, volunteer work, teaching
- Asocial ikigai: for example, a solitary practice of self-discipline, spirituality, or study without any particular intent to teach others
- Antisocial ikigai: for example, a strong desire to outlive an enemy, or to harm a person or group that one hates
You may be thinking: wait, aren’t those last things bad?
And… Maybe! But ikigai is not a matter of morality or even about “warm fuzzy feelings”. The fact is, having a sense of purpose increases longevity regardless of moral implications or niceness.
Nevertheless, for obvious reasons there is a lot more focus on the first two categories (social and asocial), and of those, especially the first category (social), because on a social level, “we all do well when we all do well”.
We exemplified them above, but they can be defined:
- Social: working for the betterment of society
- Asocial: working for the betterment of oneself
Of course, for many people, the same ikigai may cover both of those—often somebody who excels at something for its own sake and/but shares it with others to enrich their lives also, for example a teacher, an artist, a scientist, etc.
For it to cover both, however, requires that both parts of it are genuinely part of their feeling of ikigai, and not merely unintended consequences.
For example, a piano teacher who loves music in general and the piano in particular, and would gladly spend every waking moment studying/practising/performing, but hates having to teach it, but needs to pay the bills so teaches it anyway, cannot be said to be living any kind of social ikigai there, just asocial. And in fact, if teaching the piano is causing them to not have the time or energy to pursue it for its own sake, they might not even be living any ikigai at all.
One other thing to watch out for
There is one last stumbling block, which is that while we can find ikigai, we can also lose it! Examples of this may include:
- A professional whose job is their ikigai, until they face mandatory retirement or are otherwise unable to continue their work (perhaps due to disability, for example)
- A parent whose full-time-parent role is their ikigai, until their children leave for school, university, life in general
- A married person whose “devoted spouse” role is their ikigai, until their partner dies
For this reason, people of any age can have a “crisis of identity” that’s actually more of a “crisis of purpose”.
There are two ways of handling this:
- Have a back-up ikigai ready! For example, if your profession is your ikigai, maybe you have a hobby waiting in the wings, that you can smoothly jump ship to upon retirement.
- Embrace the fluidity of life! Sometimes, things don’t happen the way we expect. Sometimes life’s surprises can trip us up; sometimes they can leave us a sobbing wreck. But so long as life continues, there is an opportunity to pick ourselves up and decide where to go from that point. Note that this is not fatalism, by the way, it doesn’t have to be “this bad thing happened so that we could find this good thing, so really it was a good thing all along”. Rather, it can equally readily be “well, we absolutely did not want that bad thing to happen, but since it did, now we shall take it this way from here”.
For more on developing/maintaining psychological resilience in the face of life’s less welcome adversities, see:
Psychological Resilience Training
…and:
Putting The Abs Into Absurdity ← do not underestimate the power of this one
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

ADHD… As An Adult?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
ADHD—not just for kids!
Consider the following:
- If a kid has consistent problems paying attention, it’s easy and common to say “Aha, ADHD!”
- If a young adult has consistent problems paying attention, it’s easy and common to say “Aha, a disinterested ne’er-do-well!”
- If an older adult has consistent problems paying attention, it’s easy and common to say “Aha, a senior moment!”
Yet, if we recognize that ADHD is fundamentally a brain difference in children (and we do; there are physiological characteristics that we can test), and we can recognize that as people get older our brains typically have less neuroplasticity (ability to change) than when we are younger rather than less, then… Surely, there are just as many adults with ADHD as kids!
After all, that rather goes with the linear nature of time and the progressive nature of getting older.
So why do kids get diagnoses so much more often than adults?
Parents—and schools—can find children’s ADHD challenging, and it’s their problem, so they look for an explanation, and ADHD isn’t too difficult to find as a diagnosis.
Meanwhile, adults with ADHD have usually developed coping mechanisms, have learned to mask and/or compensate for their symptoms, and we expect adults to manage their own problems, so nobody’s rushing to find an explanation on their behalf.
Additionally, the stigma of neurodivergence—especially something popularly associated with children—isn’t something that many adults will want for themselves.
But, if you have an ADHD brain, then recognizing that (even if just privately to yourself) can open the door to much better management of your symptoms… and your life.
So what does ADHD look like in adults?
ADHD involves a spread of symptoms, and not everyone will have them all, or have them in the same magnitude. However, very commonly most noticeable traits include:
- Lack of focus (ease of distraction)
- Conversely: high focus (on the wrong things)
- To illustrate: someone with ADHD might set out to quickly tidy the sock drawer, and end up Marie Kondo-ing their entire wardrobe… when they were supposed to doing something else
- Conversely: high focus (on the wrong things)
- Poor time management (especially: tendency to procrastinate)
- Forgetfulness (of various kinds—for example, forgetting information, and forgetting to do things)
Want To Take A Quick Test? Click Here ← this one is reputable, and free. No sign in required; the test is right there.
Wait, where’s the hyperactivity in this Attention Deficit Hyperactivity Disorder?
It’s often not there. ADHD is simply badly-named. This stems from how a lot of mental health issues are considered by society in terms of how much they affect (and are observable by) other people. Since ADHD was originally noticed in children (in fact being originally called “Hyperkinetic Reaction of Childhood”), it ended up being something like:
“Oh, your brain has an inconvenient relationship with dopamine and you are driven to try to correct that by shifting attention from boring things to stimulating things? You might have trouble-sitting-still disorder”
Hmm, this sounds like me (or my loved one); what to do now at the age of __?
Some things to consider:
- If you don’t want medication (there are pros and cons, beyond the scope of today’s article), you might consider an official diagnosis not worth pursuing. That’s fine if so, because…
- More important than whether or not you meet certain diagnostic criteria, is whether or not the strategies recommended for it might help you.
- Whether or not you talk to other people about it is entirely up to you. Maybe it’s a stigma you’d rather avoid… Or maybe it’ll help those around you to better understand and support you.
- Either way, you might want to learn more about ADHD in adults. Today’s article was about recognizing it—we’ll write more about managing it another time!
In the meantime… We recommended a great book about this a couple of weeks ago; you might want to check it out:
Click here to see our review of “The Silent Struggle: Taking Charge of ADHD in Adults”!
Note: the review is at the bottom of that page. You’ll need to scroll past the video (which is also about ADHD) without getting distracted by it and forgetting you were there to see about the book. So:
- Click the above link
- Scroll straight to the review!
Share This Post
-

‘I can’t quite shut it off’: Prevalence of insomnia a growing concern for women
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
 Tasha Werner, 43, gets up at 3:30 a.m. twice a week for her part-time job at a fitness centre in Calgary. After a five-hour shift, she is back home by 9 a.m. to homeschool her two children, aged 9 and 12. The hardest part of her position – stay-at-home mom, homeschool teacher and part-time worker – is the downtime “lost from my life,” says Werner.
Tasha Werner, 43, gets up at 3:30 a.m. twice a week for her part-time job at a fitness centre in Calgary. After a five-hour shift, she is back home by 9 a.m. to homeschool her two children, aged 9 and 12. The hardest part of her position – stay-at-home mom, homeschool teacher and part-time worker – is the downtime “lost from my life,” says Werner.A study by Howard M. Kravitz, a psychiatrist in Chicago, showed that up to 60 per cent of women experience sleep disorders due to hormonal changes linked to menopause. But there is an increasing prevalence of insomnia symptoms in women that may be attributed, in part, to societal changes.
“We live in a world that didn’t exist a generation ago. Now everyone is trying to figure it out,” says Michael Grandner, director of the Sleep and Health Research Program at the University of Arizona.
While women are no longer expected to stay at home, many who are employed outside the home also have the primary responsibility for family matters. And women aged 40 to 60 commonly fall within the “sandwich generation,” caring for both children and parents.
As women juggle their responsibilities, these duties can take a toll, both emotionally and practically.
Both Werner and her husband were raised in traditional homes; their mothers stayed at home to oversee childcare, cooking, grocery shopping and household duties. Initially, Werner and her husband followed a similar path, mirroring their parents’ lives as homemakers. “I think we just fell into what we were used to,” says Werner.
However, a notable shift in their family dynamics occurred once she started working outside the home.
Her children’s physical needs and illnesses have had major consequences on her sleep. If one of the children is sick with the flu, that’s “a week of not a lot of sleep during the night,” she says, “because that’s my job.” Many nights, she finds herself waking up between 1 a.m. and 3 a.m., worrying about how the kids are doing academically or behaviourally.
“We face a specific set of anxieties and a different set of pressures than men,” says Emma Kobil, who has been a therapist in Denver, Colo., for 15 years and is now an insomnia coach. There is so much pressure to be everything as a woman – to be an amazing homemaker and worker while maintaining a hot-rocking body and having a cool personality, to “be the cool mom but also the CEO, to follow your dreams and be the boss b****,” says Kobil.
And there’s an appeal to that concept. Daughters grow up viewing their moms as superwomen juggling responsibilities. But what isn’t always obvious are the challenges women face while managing their lives and the health issues they may encounter.
A study revealed that women are 41 per cent more at risk of insomnia than men.
A thorough study revealed that women are 41 per cent more at risk of insomnia than men. Beyond menopausal hormonal shifts, societal pressures, maternal concerns and the challenge of balancing multiple roles contribute to women’s increased susceptibility to insomnia.
Cyndi Aarrestad, 57, lives on a farm in Saskatchewan with her husband, Denis. Now an empty nester, Aarrestad fills her time working on the farm, keeping house, volunteering at her church and managing her small woodworking business. And she struggles with sleep.
Despite implementing some remedies, including stretching, drinking calming teas and rubbing her feet before bed, Aarrestad says achieving restful sleep has remained elusive for the past decade.
Two primary factors contribute to her sleep challenges — her inability to quiet her mind and hormonal hot flashes due to menopause. Faced with family and outside commitments, Aarrestad finds it challenging to escape night time’s mental chatter. “It’s a mom thing for me … I can’t quite shut it off.” Even as her children transitioned to young adulthood and moved out, the worries persisted, highlighting the lasting concerns moms have about their kids’ jobs, relationships and overall well-being.
Therapist Kobil says that every woman she’s ever worked with experiences this pressure to do everything, to be perfect. These women feel like they’re not measuring up. They’re encouraged to take on other people’s burdens; to be the confidante and the saviour in many ways; to sacrifice themselves. Sleep disruptions simply reflect the consequences of this pressure.
“They’re trying to fit 20 hours in a 24-hour day, and it doesn’t work,” says Grandner, the sleep specialist.
Grandner says that consistently sleeping six hours or less as an adult makes one 55 per cent more likely to become obese, 20 per cent more likely to develop high blood pressure, and 30 per cent more likely to develop Type 2 diabetes if you didn’t have it already. This lack of sleep makes you more likely to catch the flu. It makes vaccines less effective, and it increases your likelihood of developing depression and anxiety.
When is the time to change? Yesterday. Grandner warns that the sleep sacrifices made at a young age impact health later. But it’s never too late to make changes, he says, and “you do the best with what you’ve got.”
Kobil suggests a practical approach for women struggling with sleep. She emphasizes understanding that sleeplessness isn’t a threat and encourages a shift in mindset about being awake. Instead of fighting sleeplessness, she advises treating oneself kindly, recognizing the difficulty.
Kobil recommends creating a simple playbook with comforting activities for awake moments during the night. Just as you would comfort a child who’s afraid, she suggests being gentle with yourself, gradually changing the perception of wakefulness into a positive experience.
This article is republished from HealthyDebate under a Creative Commons license. Read the original article.
Share This Post
-

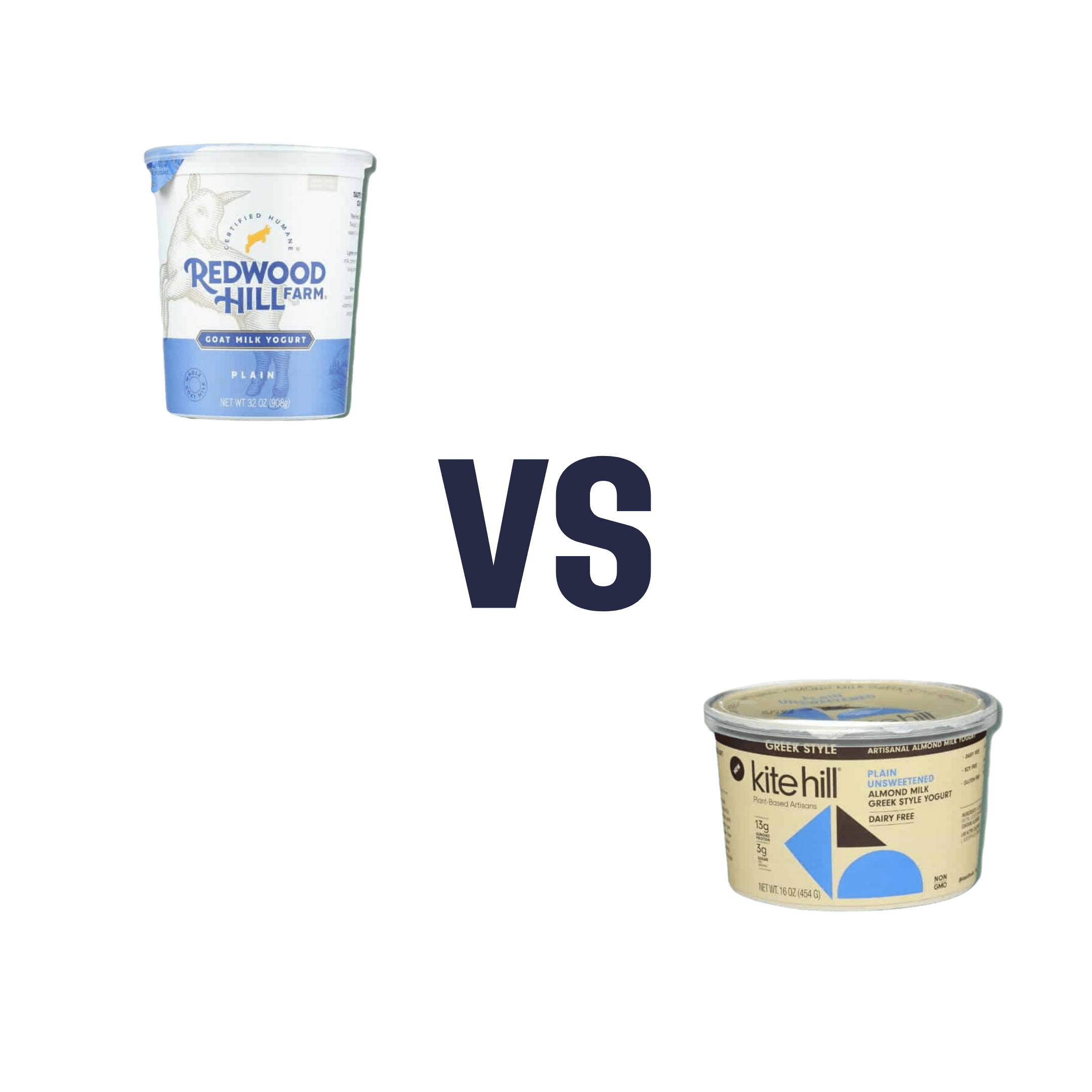
Goat Milk Greek Yogurt vs Almond Milk Greek Yogurt – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing goat milk yogurt to almond milk yogurt, we picked the almond milk yogurt.
Why?
Surprised? Honestly, we were too!
Much as we love almonds, we were fully expecting to write about how they’re very close in nutritional value, but the dairy yogurt has more probiotics, but no, as it turns out when we looked into them, they’re quite comparable in that regard.
It’s easy to assume “goat milk yogurt is more natural and therefore healthier”, but in both cases, it was a case of taking a fermentable milk, and fermenting it (an ancient process). “But almond milk is a newfangled thing”, well, new-ish…

So what was the deciding factor?
In this case, the almond milk yogurt has about twice the protein per (same size) serving, compared to the goat milk; all the other macros are about the same, and the micronutrients are similar. Like many plant-based milks and yogurts, this one is fortified with calcium and vitamin D, so that wasn’t an issue either.
In short: the only meaningful difference was the protein, and the almond came out on top.
However!
The almond came out on top only because it is strained; this can be done (or not) with any kind of yogurt, be it from an animal or a plant.
In other words: if it had been different brands, the goat milk yogurt could have come out on top!
The take-away idea here is: always read labels, because as you’ve just seen, even we can get surprised sometimes!
seriously if you only remember one thing from this today, make it the above
Other thing worth mentioning: yogurts, and dairy products in general, are often made with common allergens (e.g. dairy, nuts, soy, etc). So if you are allergic or intolerant, obviously don’t choose the one to which you are allergic or intolerant.
That said… If you are lactose-intolerant, but not allergic, goat’s milk does have less lactose than cow’s milk. But of course, you know your limits better than we can in this regard.
Want to try some?
Amazon is not coming up with the goods for this one (or anything even similar, at time of writing), so we recommend trying your local supermarket (and reading labels, because products vary widely!)
What you’re looking for (be it animal- or plant-based):
- Live culture probiotic bacteria
- No added sugar
- Minimal additives in general
- Lastly, check out the amounts for protein, calcium, vitamin D, etc.
Enjoy!
Share This Post

Related Posts
-

Nanotechnology vs Alcohol Damage!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One Thing That Does Pair Well With Alcohol…
Alcohol is not a healthy thing to consume. That shouldn’t be a controversial statement, but there is a popular belief that it can be good for the heart:
Red Wine & The Heart: Can We Drink To Good Health?
The above is an interesting and well-balanced article that examines the arguments for health benefits (including indirectly, e.g. social aspects).
Ultimately, though, as the World Health Organization puts it:
WHO: No level of alcohol consumption is safe for our health
There is some good news:
We can somewhat reduce the harm done by alcohol by altering our habits slightly:
How To Make Drinking Less Harmful
…and we can also, of course, reduce our alcohol consumption (ideally to zero, but any reduction is an improvement already):
And, saving the best news (in this section, anyway) for last, it is almost always possible to undo the harm done specifically to one’s liver:
Nanotechnology to the rescue?
Remember when we had a main feature about how colloidal gold basically does nothing by itself (and that that’s precisely why gold is used in medicine, when it is used)?
Now it has an extra bit of nothing to do, for our benefit (if we drink alcohol, anyway), as part of a gel that detoxifies alcohol before it can get to our liver:
Gold is one of the “ingredients” in a gel containing a nanotechnology lattice of protein fibrils coated with iron (and the gold is there as an inert catalyst, which is chemistry’s way of saying it doesn’t react in any way but it does cheer the actual reagents on). There’s more chemistry going on than we have room to discuss in our little newsletter, so if you like the full details, you can read about that here:
Single-site iron-anchored amyloid hydrogels as catalytic platforms for alcohol detoxification
The short and oversimplified explanation is that instead of alcohol being absorbed from the gut and transported via the bloodstream to the liver, where it is metabolized (poisoning the liver as it goes, and poisoning the rest of the body too, including the brain), the alcohol is degraded while it is still in the gastrointestinal tract, converted by the gel’s lattice into acetic acid (which is at worst harmless, and actually in moderation a good thing to have).
Even shorter and even more oversimplified: the gel turns the alcohol into vinegar in the stomach and gut, before it can get absorbed into the blood.
But…
Of course there’s a “but”…
There are some limitations:
It doesn’t get it all (tests so far found it only gets about half of the alcohol), and so far it’s only been tested on mice, so it’s not on the market yet—while the researchers are sufficiently confident about it that a patent application has now been made, though, so it’ll probably show up on the market in the near future.
You can read a pop-science article about it (with diagrams!) here:
New gel breaks down alcohol in the body
Want to read more…
…about how to protect your organs (including your brain) from alcohol completely?
We’ve reviewed quite a number of books about quitting alcohol, so it’s hard to narrow it down to a single favorite, but after some deliberation, we’ll finish today with recommending:
Quit Drinking – by Rebecca Dolton ← you can read our review here
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Best Mobility Exercises For Each Joint
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Stiff joints and tight muscles limit movement, performance, and daily activities. They also increase the risk of injury, and increase recovery time if the injury happens. So, it’s pretty important to take care of that!
Here’s how
Key to joint health involves understanding mobility, flexibility, and stability:
- Mobility: active joint movement through a range of motion.
- Flexibility: muscle lengthening passively through a range of motion.
- Stability: body’s ability to return to position after disturbance.
Different body parts have different needs when it comes to prioritizing mobility, flexibility, and stability exercises. So, with that in mind, here’s what to do for your…
- Wrists: flexibility and stability (e.g., wrist circles, loaded flexions/extensions).
- Elbows: Stability is key; exercises like wrist and shoulder movements benefit elbows indirectly.
- Shoulders: mobility and stability; exercises include prone arm circles, passive hangs, active prone raises, easy bridges, and stick-supported movements.
- Spine: mobility and stability; recommended exercises include cat-cow and quadruped reach.
- Hips: mobility and flexibility through deep squat hip rotations; beginners can use hands for support.
- Knees: stability; exercises include elevated pistols, Bulgarian split squats, lunges, and single-leg balancing.
- Ankles: flexibility and stability; exercises include lunges, prying goblet squats, and deep squats with support if necessary.
For more on all of these, plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Building & Maintaining Mobility
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Going for a bushwalk? 3 handy foods to have in your backpack (including muesli bars)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This time of year, many of us love to get out and spend time in nature. This may include hiking through Australia’s many beautiful national parks.
Walking in nature is a wonderful activity, supporting both physical and mental health. But there can be risks and it’s important to be prepared.
You may have read the news about hiker, Hadi Nazari, who was recently found alive after spending 13 days lost in Kosciuszko National Park.
He reportedly survived for almost two weeks in the Snowy Mountains region of New South Wales by drinking fresh water from creeks, and eating foraged berries and two muesli bars.
So next time you’re heading out for a day of hiking, what foods should you pack?
Here are my three top foods to carry on a bushwalk that are dense in nutrients and energy, lightweight and available from the local grocery store.
Leah-Anne Thompson/Shutterstock 1. Muesli bars
Nazari reportedly ate two muesli bars he found in a mountain hut. Whoever left the muesli bars there made a great choice.
Muesli bars come individually wrapped, which helps them last longer and makes them easy to transport.
They are also a good source of energy. Muesli bars typically contain about 1,500–1,900 kilojoules per 100 grams. The average energy content for a 35g bar is about 614kJ.
This may be a fraction of what you’d usually need in a day. However, the energy from muesli bars is released at a slow to moderate pace, which will help keep you going for longer.
Muesli bars are also packed with nutrients. They contain all three macronutrients (carbohydrate, protein and fat) that our body needs to function. They’re a good source of carbohydrates, in particular, which are a key energy source. An average Australian muesli bar contains 14g of whole grains, which provide carbohydrates and dietary fibre for long-lasting energy.
Muesli bars that contain nuts are typically higher in fat (19.9g per 100g) and protein (9.4g per 100g) than those without.
Fat and protein are helpful for slowing down the release of energy from foods and the protein will help keep you feeling full for longer.
There are many different types of muesli bars to choose from. I recommend looking for those with whole grains, higher dietary fibre and higher protein content.
2. Nuts
Nuts are nature’s savoury snack and are also a great source of energy. Cashews, pistachios and peanuts contain about 2,300-2,400kJ per 100g while Brazil nuts, pecans and macadamias contain about 2,700-3,000kJ per 100g. So a 30g serving of nuts will provide about 700-900kJ depending on the type of nut.
Just like muesli bars, the energy from nuts is released slowly. So even a relatively small quantity will keep you powering on.
Nuts are also full of nutrients, such as protein, fat and fibre, which will help to stave off hunger and keep you moving for longer.
When choosing which nuts to pack, almost any type of nut is going to be great.
Peanuts are often the best value for money, or go for something like walnuts that are high in omega-3 fatty acids, or a nut mix.
Whichever nut you choose, go for the unsalted natural or roasted varieties. Salted nuts will make you thirsty.
Nut bars are also a great option and have the added benefit of coming in pre-packed serves (although nuts can also be easily packed into re-usable containers).
If you’re allergic to nuts, roasted chickpeas are another option. Just try to avoid those with added salt.
Nuts are nature’s savoury snack and are also a great source of energy. Eakrat/Shutterstock 3. Dried fruit
If nuts are nature’s savoury snack, fruit is nature’s candy. Fresh fruits (such as grapes, frozen in advance) are wonderfully refreshing and perfect as an everyday snack, although can add a bit of weight to your hiking pack.
So if you’re looking to reduce the weight you’re carrying, go for dried fruit. It’s lighter and will withstand various conditions better than fresh fruit, so is less likely to spoil or bruise on the journey.
There are lots of varieties of dried fruits, such as sultanas, dried mango, dried apricots and dried apple slices.
These are good sources of sugar for energy, fibre for fullness and healthy digestion, and contain lots of vitamins and minerals. So choose one (or a combination) that works for you.
Don’t forget water
Next time you head out hiking for the day, you’re all set with these easily available, lightweight, energy- and nutrient-dense snacks.
This is not the time to be overly concerned about limiting your sugar or fat intake. Hiking, particularly in rough terrain, places demands on your body and energy needs. For instance, an adult hiking in rough terrain can burn upwards of about 2,000kJ per hour.
And of course, don’t forget to take plenty of water.
Having access to even limited food, and plenty of fresh water, will not only make your hike more pleasurable, it can save your life.
Margaret Murray, Senior Lecturer, Nutrition, Swinburne University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:




