Do we really need to burp babies? Here’s what the research says
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Parents are often advised to burp their babies after feeding them. Some people think burping after feeding is important to reduce or prevent discomfort crying, or to reduce how much a baby regurgitates milk after a feed.
It is true babies, like adults, swallow air when they eat. Burping releases this air from the top part of our digestive tracts. So when a baby cries after a feed, many assume it’s because the child needs to “be burped”. However, this is not necessarily true.
Why do babies cry or ‘spit up’ after a feed?
Babies cry for a whole host of reasons that have nothing to do with “trapped air”.
They cry when they are hungry, cold, hot, scared, tired, lonely, overwhelmed, needing adult help to calm, in discomfort or pain, or for no identifiable reason. In fact, we have a name for crying with no known cause; it’s called “colic”.
“Spitting up” – where a baby gently regurgitates a bit of milk after a feed – is common because the muscle at the top of a newborn baby’s stomach is not fully mature. This means what goes down can all too easily go back up.
Spitting up frequently happens when a baby’s stomach is very full, there is pressure on their tummy or they are picked up after lying down.
Spitting up after feeding decreases as babies get older. Three-quarters of babies one month old spit up after feeding at least once a day. Only half of babies still spit up at five months and almost all (96%) stop by their first birthdays.

Does burping help reduce crying or spitting up?
Despite parents being advised to burp their babies, there’s not much research evidence on the topic.
One study conducted in India encouraged caregivers of 35 newborns to burp their babies, while caregivers of 36 newborns were not given any information about burping.
For the next three months, mothers and caregivers recorded whether their baby would spit up after feeding and whether they showed signs of intense crying.
This study found burping did not reduce crying and actually increased spitting up.
When should I be concerned about spitting up or crying?
Most crying and spitting up is normal. However, these behaviours are not:
- refusing to feed
- vomiting so much milk weight gain is slow
- coughing or wheezing distress while feeding
- bloody vomit.
If your baby has any of these symptoms, see a doctor or child health nurse.
If your baby seems unbothered by vomiting and does not have any other symptoms it is a laundry problem rather than something that needs medical attention.
It is also normal for babies to cry and fuss quite a lot; two hours a day, for about the first six weeks is the average.
This has usually reduced to about one hour a day by the time they are three months of age.
Crying more than this doesn’t necessarily mean there is something wrong. The intense, inconsolable crying of colic is experienced by up to one-quarter of young babies but goes away with time on its own .
If your baby is crying more than average or if you are worried there might be something wrong, you should see your doctor or child health nurse.

Not everyone burps their baby
Burping babies seems to be traditional practice in some parts of the world and not in others.
For example, research in Indonesia found most breastfeeding mothers rarely or never burped their babies after feeding.
One factor that may influence whether a culture encourages burping babies may be related to another aspect of infant care: how much babies are carried.
Carrying a baby in a sling or baby carrier can reduce the amount of time babies cry.
Babies who are carried upright on their mother or another caregiver’s front undoubtedly find comfort in that closeness and movement.
Babies in slings are also being held firmly and upright, which would help any swallowed air to rise up and escape via a burp if needed.
Using slings can make caring for a baby easier. Studies (including randomised controlled trials) have also shown women have lower rates of post-natal depression and breastfeed for longer when they use a baby sling.
It is important baby carriers and slings are used safely, so make sure you’re up to date on the latest advice on how to do it.
So, should I burp my baby?
The bottom line is: it’s up to you.
Gently burping a baby is not harmful. If you feel burping is helpful to your baby, then keep doing what you’re doing.
If trying to burp your baby after every feed is stressing you or your baby out, then you don’t have to keep doing it.
Karleen Gribble, Adjunct Associate Professor, School of Nursing and Midwifery, Western Sydney University and Nina Jane Chad, Research Fellow, University of Sydney School of Public Health, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

‘It’s okay to poo at work’: new health campaign highlights a common source of anxiety

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For most people, the daily or near-daily ritual of having a bowel motion is not something we give a great deal of thought to. But for some people, the need to do a “number two” in a public toilet or at work can be beset with significant stress and anxiety.
In recognition of the discomfort people may feel around passing a bowel motion at work, the Queensland Department of Health recently launched a social media campaign with the message “It’s okay to poo at work”.
The campaign has gained significant traction on Instagram and Facebook. It has been praised by health and marketing experts for its humorous handling of a taboo topic.
A colourful Instagram post is accompanied by a caption warning of the health risks of “holding it in”, including haemorrhoids and other gastrointestinal problems. The caption also notes:
If you find it extremely difficult to poo around other people, you might have parcopresis.

Queensland Health/Instagram What is parcopresis?
Parcopresis, sometimes called “shy bowel”, occurs when people experience a difficulty or inability to poo in public toilets due to fear of perceived scrutiny by others.
People with parcopresis may find it difficult to go to the toilet in public places such as shopping centres, restaurants, at work or at school, or even at home when friends or family are around.
They may fear being judged by others about unpleasant smells or sounds when they have a bowel motion, or how long they take to go, for example.
Living with a gastrointestinal condition (at least four in ten Australians do) may contribute to parcopresis due to anxiety about the need to use a toilet frequently, and perceived judgment from others when doing so. Other factors, such as past negative experiences or accessibility challenges, may also play a role.
Some people may feel uncomfortable about using the toilet at work. Motortion Films/Shutterstock For sufferers, anxiety can present in the form of a faster heart rate, rapid breathing, sweating, muscle tension, blushing, nausea, trembling, or a combination of these symptoms. They may experience ongoing worry about situations where they may need to use a public toilet.
Living with parcopresis can affect multiple domains of life and quality of life overall. For example, sufferers may have difficulties relating to employment, relationships and social life. They might avoid travelling or attending certain events because of their symptoms.
How common is parcopresis?
We don’t really know how common parcopresis is, partly due to the difficulty of evaluating this behaviour. It’s not necessarily easy or appropriate to follow people around to track whether they use or avoid public toilets (and their reasons if they do). Also, observing individual bathroom activities may alter the person’s behaviour.
I conducted a study to try to better understand how common parcopresis is. The study involved 714 university students. I asked participants to respond to a series of vignettes, or scenarios.
In each vignette participants were advised they were at a local shopping centre and they needed to have a bowel motion. In the vignettes, the bathrooms (which had been recently cleaned) had configurations of either two or three toilet stalls. Each vignette differed by the configuration of stalls available.
The rate of avoidance was just over 14% overall. But participants were more likely to avoid using the toilet when the other stalls were occupied.
Around 10% avoided going when all toilets were available. This rose to around 25% when only the middle of three toilets was available. Men were significantly less likely to avoid going than women across all vignettes.
For those who avoided the toilet, many either said they would go home to poo, use an available disabled toilet, or come back when the bathroom was empty.
Parcopresis at work
In occupational settings, the rates of anxiety about using shared bathrooms may well be higher for a few reasons.
For example, people may feel more self-conscious about their bodily functions being heard or noticed by colleagues, compared to strangers in a public toilet.
People may also experience guilt, shame and fear about being judged by colleagues or supervisors if they need to make extended or frequent visits to the bathroom. This may particularly apply to people with a gastrointestinal condition.
Reducing restroom anxiety
Using a public toilet can understandably cause some anxiety or be unpleasant. But for a small minority of people it can be a real problem, causing severe distress and affecting their ability to engage in activities of daily living.
If doing a poo in a toilet at work or another public setting causes you anxiety, be kind to yourself. A number of strategies might help:
- identify and challenge negative thoughts about using public toilets and remind yourself that using the bathroom is normal, and that most people are not paying attention to others in the toilets
- try to manage stress through relaxation techniques such as deep breathing and progressive muscle relaxation, which involves tensing and relaxing different muscles around the body
- engaging in gradual exposure can be helpful, which means visiting public toilets at different times and locations, so you can develop greater confidence in using them
- use grounding or distraction techniques while going to the toilet. These might include listening to music, watching something on your phone, or focusing on your breathing.
If you feel parcopresis is having a significant impact on your life, talk to your GP or a psychologist who can help identify appropriate approaches to treatment. This might include cognitive behavioural therapy.
Simon Robert Knowles, Associate Professor and Clinical Psychologist, Swinburne University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Inverse Vaccines for Autoimmune Diseases
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Inverse Vaccines for Autoimmune Diseases

This is Dr. Jeffrey Hubbell. He’s a molecular engineer, with a focus on immunotherapy, immune response, autoimmune diseases, and growth factor variants.
He’s held 88 patents, and was the recipient of the Society for Biomaterials’ Founders Award for his “long-term, landmark contributions to the discipline of biomaterials”, amongst other awards and honours that would make our article too long if we included them all.
And, his latest research has been about developing…
Inverse Vaccines
You may be thinking: “you mean diseases; he’s engineering diseases?”
And no, it’s not that. Here’s how it works:
Normally in the case of vaccine, it’s something to tell the body “hey, if you see something that looks like this, you should kill it on sight” and the body goes “ok, preparing countermeasures according to these specifications; thanks for the heads-up”
In the case of an inverse vaccine, it’s the inverse. It’s something to tell the body “hey, this thing you seem to think is a threat, it’s actually not, and you should leave it alone”.
Why this matters for people with autoimmune diseases
Normally, autoimmune diseases are treated in one or more of the following ways:
- Dampen the entire immune system (bad for immunity against actual diseases, obviously, and is part of why many immunocompromised people have suffered and died disproportionately from COVID, for example)
- Give up and find a workaround (a good example of this is Type 1 Diabetes, and just giving up on the pancreas not being constantly at war with itself, and living on exogenous insulin instead)
Neither of those are great.
What inverse vaccines do is offer a way to flag the attacked-in-error items as acceptable things to have in the body. Those might be things that are in our body by default, as in the case of many autoimmune diseases, or they may even be external items that should be allowed but aren’t, as in the case of gluten, in the context of Celiac disease.
The latest research is not yet accessible for free, alas, but you can read the abstract here:
Or if you prefer a more accessible pop-science approach, here’s a great explanatory article:
“Inverse vaccine” shows potential to treat multiple sclerosis and other autoimmune diseases
Where can we get such inverse vaccines?
❝There are no clinically approved inverse vaccines yet, but we’re incredibly excited about moving this technology forward❞
~ Dr. Jeffrey Hubbell
But! Lest you be disappointed, you can get in line already, in the case of the Celiac disease inverse vaccine, if you’d like to be part of their clinical trial:
Click here to see if you are eligible to be part of their clinical trial
If you’re not up for that, or if your autoimmune disease is something else (most of the rest of their research is presently focusing on Multiple Sclerosis and Type 1 Diabetes), then:
- The phase 1 MS trial is currently active, estimated completion in summer 2024.
- They are in the process of submitting an investigational new drug (IND) application for Type 1 Diabetes
- This is the first step to starting clinical safety and efficacy trials
…so, watch this space!
Share This Post
-
The Japanese Health Initiative That Lowers Blood Sugars
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve talked before about Good (Or Bad) Health Starts With Your Blood, and how a lot of human disease begins with, or is exacerbated by, diabetes or even pre-diabetes, and that in the US, this is even more strongly true than in the rest of the world, what with the US being #1 for diabetes.
However! That does not mean if you’re not prediabetic, there is no threat. This is because it is usually insulin resistance, and not the high blood sugar content itself, that is the main driver of disease. It just so happens that blood sugars are a lot quicker and easier to test, and the correlation between them is high. On the other hand, insulin resistance will often go unnoticed for many years, because the pancreas just cranks out more and more extra insulin to compensate and keep the blood sugars balanced—until one day it can’t because the body is so resistant to insulin that the pancreas just can’t produce enough to get it to care adequately, and that’s when the blood sugars will finally rise (and get noticed).
We reviewed an excellent book about precisely this (very, very common) phenomenon: Why We Get Sick – by Dr. Benjamin Bikman
The good news is, there are things can be done to Improve Your Insulin Sensitivity.
And with regard to blood sugars themselves, an excellent list is: 10 Ways To Balance Blood Sugars
Number 8 in that list was:
After you eat, move
The glucose you eat will be used to replace lost muscle glycogen, before any left over is stored as fat… and, while it’s waiting to be stored as fat, just sitting in your bloodstream being high blood sugars. So, this whole thing will go a lot better if you are actively using muscle glycogen (by moving your body).
Inchauspé gives a metaphor: imagine a steam train worker, shoveling coal into the furnace. Meanwhile, other workers are bringing more coal. If the train is moving quickly, the coal can be shoveled into the furnace and burned and won’t build up so quickly. But if the train is moving slowly or not at all, that coal is just going to build up and build up, until the worker can shovel no more because of being neck-deep in coal.
Same with your blood sugars!
But that—sound advice as it is—remains a little vague, leaving us with questions such as:
- How much movement?
- For how long?
- And what’s the window of opportunity to enjoy this effect?
With those questions in mind…
Japan’s “Plus 10” Initiative
The government of Japan has a “plus 10” initiative, whose goal is to encourage everyone to add just 10 minutes of extra activity to each day. You might think that won’t make a big difference, but in fact it all adds up, for example: Cumulative Exercise vs Neurodegeneration ← which shows how it is cumulative exercise over time that matters the most in this regard, which means that “little and often” really does count for a lot.
We’ve also written before about How Useful Is “Exercise Snacking”, Really?, with some very specific protocols there for those who like to truly optimize everything.
Most recently, a Japanese research team investigated the effects of two different approaches to post-dinner exercise, on blood sugars:
- Walk for 10 minutes, immediately after eating
- Walk for 30 minutes, 30 minutes after eating
There was also a control condition (rest only, no walking).
They measured the effect of these conditions on blood glucose in three ways:
- 2‑hour blood glucose area under the curve (AUC)*
- mean average glucose
- peak glucose
*that’s a way of looking at the total impact of it over the course of the recording period
They additionally measured heart rate, perceived exertion, and gastrointestinal discomfort.
They found that both walking conditions significantly reduced 2‑hour blood glucose AUC and mean glucose versus control:
- 10-min walk: the AUC was 15,607 mg·min/dL (control was 16,605), and mean glucose = 127.9 mg/dL (control was 135.8mg/dL)
- 30-min walk: also effective, but no significant difference compared to the 10‑min walk immediately after eating.
However! Only the immediate 10‑min walk significantly lowered peak glucose (164.3 mg/dL, compared to the control condition’s 181.9 mg/dL).
Which means that the immediate 10-minute walk not only equals the delayed 30-minute walk in most ways, but also outright beats that in a third way. And that third way, the peak glucose? That’s where the insulin resistance starts, so this is critical.
As for the other things they measured: both walking conditions were rated as low perceived effort, with the 10‑min walk feeling the relatively easier of the two. No increase in gastrointestinal discomfort was reported for either walking condition.
You may be wondering about the pace of this walking:
❝The walking speed was self-selected by the participants to be comfortable. The participants were instructed to walk at their usual relaxed pace as in their daily life. The walking speed was set on a treadmill and was implemented at the same speed for the two walking conditions.❞
You can read the paper in full, here: Positive impact of a 10-min walk immediately after glucose intake on postprandial glucose levels
If walking isn’t your thing, or you don’t have a treadmill and the weather outside is frightful, then you might like:
No-Exercise Exercise! ← for a veritable buffet of exercise snacking ideas
Want to learn more?
Consider:
15 Easy Japanese Habits That Will Transform Your Health
Enjoy!
Share This Post




-

Cashew Nuts vs Coconut – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cashew nuts to coconut, we picked the cashews.
Why?
It can be argued this isn’t a fair comparison, as coconuts aren’t true nuts, but it’s at the very least a useful comparison, because they have very similar (often the same) culinary uses, so deciding between one or the other is something people will often do.
In terms of macros, cashews have 6x the protein and more than 2x the fiber, as well as slightly more fat (but the fats are healthy, as are those of coconut, by the way) and 2x the carbs. Depending on what you’re looking for, this head-to-head could come out differently, but we say it’s a win for cashews.
You may be wondering: if cashews have more of all those things, what are coconuts made of? And the answer is that coconuts have 8x the water (and yes, this is counting the coconut meat only, not including the milk inside). Of course, if you get dessicated coconut, then it won’t have that, but we’re comparing fresh to fresh.
In the category of vitamins, cashews have a lot more of vitamins B1, B2, B3, B5, B6, E, and K. Meanwhile, coconut has more vitamin C, but it’s not a lot. An easy win for cashews here.
When it comes to minerals, cashews have rather more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. On the other hand, coconut has more sodium. Another easy win for cashews.
Cashews also have the lower glycemic index.
All in all, cashews win the day.
Want to learn more?
You might like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Women take more antidepressants after divorce than men but that doesn’t mean they’re more depressed
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Research out today from Finland suggests women may find it harder to adjust to later-life divorce and break-ups than men.
The study used population data from 229,000 Finns aged 50 to 70 who had undergone divorce, relationship break-up or bereavement and tracked their use of antidepressants before and after their relationship ended.
They found antidepressant use increased in the four years leading to the relationship dissolution in both genders, with women experiencing a more significant increase.
But it’s too simplistic to say women experience poorer mental health or tend to be less happy after divorce than men.
Remind me, how common is divorce?
Just under 50,000 divorces are granted each year in Australia. This has slowly declined since the 1990s.
More couple are choosing to co-habitate, instead of marry, and the majority of couples live together prior to marriage. Divorce statistics don’t include separations of cohabiting couples, even though they are more likely than married couples to separate.
Those who divorce are doing so later in life, often after their children grow up. The median age of divorce increased from 45.9 in 2021 to 46.7 in 2022 for men and from 43.0 to 43.7 for women.
The trend of late divorces also reflects people deciding to marry later in life. The median duration from marriage to divorce in 2022 was around 12.8 years and has remained fairly constant over the past decade.
Why do couples get divorced?
Changes in social attitudes towards marriage and relationships mean divorce is now more accepted. People are opting not to be in unhappy marriages, even if there are children involved.
Instead, they’re turning the focus on marriage quality. This is particularly true for women who have established a career and are financially autonomous.
Similarly, my research shows it’s particularly important for people to feel their relationship expectations can be fulfilled long term. In addition to relationship quality, participants reported needing trust, open communication, safety and acceptance from their partners.
“Grey divorce” (divorce at age 50 and older) is becoming increasingly common in Western countries, particularly among high-income populations. While factors such as an empty nest, retirement, or poor health are commonly cited predictors of later-in-life divorce, research shows older couples divorce for the same reasons as younger couples.
What did the new study find?
The study tracked antidepressant use in Finns aged 50 to 70 for four years before their relationship breakdown and four years after.
They found antidepressant use increased in the four years leading to the relationship break-up in both genders. The proportion of women taking antidepressants in the lead up to divorce increased by 7%, compared with 5% for men. For de facto separation antidepressant use increased by 6% for women and 3.2% for men.
Within a year of the break-up, antidepressant use fell back to the level it was 12 months before the break-up. It subsequently remained at that level among the men.
But it was a different story for women. Their use tailed off only slightly immediately after the relationship breakdown but increased again from the first year onwards.
Women’s antidepressant use increased again.
sk/UnsplashThe researchers also looked at antidepressant use after re-partnering. There was a decline in the use of antidepressants for men and women after starting a new relationship. But this decline was short-lived for women.
But there’s more to the story
Although this data alone suggest women may find it harder to adjust to later-life divorce and break-ups than men, it’s important to note some nuances in the interpretation of this data.
For instance, data suggesting women experience depression more often than men is generally based on the rate of diagnoses and antidepressant use, which does not account for undiagnosed and unmedicated people.
Women are generally more likely to access medical services and thus receive treatment. This is also the case in Australia, where in 2020–2022, 21.6% of women saw a health professional for their mental health, compared with only 12.9% of men.
Why women might struggle more after separating
Nevertheless, relationship dissolution can have a significant impact on people’s mental health. This is particularly the case for women with young children and older women.
So what factors might explain why women might experience greater difficulties after divorce later in life?
Research investigating the financial consequences of grey divorce in men and women showed women experienced a 45% decline in their standard of living (measured by an income-to-needs ratio), whereas men’s dropped by just 21%. These declines persisted over time for men, and only reversed for women following re-partnering.
Another qualitative study investigating the lived experiences of heterosexual couples post-grey divorce identified financial worries as a common theme between female participants.
A female research participant (age 68) said:
[I am most worried about] the money, [and] what I’m going to do when the little bit of money I have runs out […] I have just enough money to live. And, that’s it, [and if] anything happens I’m up a creek. And Medicare is incredibly expensive […] My biggest expense is medicine.
Another factor was loneliness. One male research participant (age 54) described he preferred living with his ex-wife, despite not getting along with her, than being by himself:
It was still [good] knowing that [the] person was there, and now that’s gone.
Other major complications of later-life divorce are possible issues with inheritance rights and next-of-kin relationships for medical decision-making.
Separation can be positive
For some people, divorce or separation can lead to increased happiness and feeling more independent.
And the mental health impact and emotional distress of a relationship dissolution is something that can be counterattacked with resilience. Resilience to dramatic events built from life experience means older adults often do respond better to emotional distress and might be able to adjust better to divorce than their younger counterparts.

Raquel Peel, Adjunct Senior Lecturer, University of Southern Queensland and Senior Lecturer, RMIT University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Can We Drink To Good Health?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Can we drink to good health?
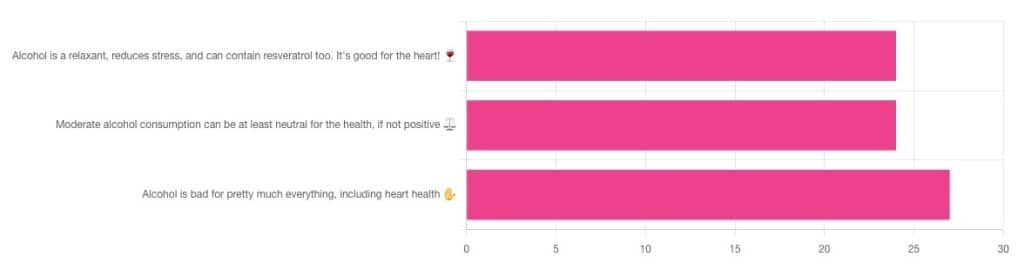
We asked you for your thoughts on alcohol and heart health, and we got quite an even spread of results!

If perchance that’s too tiny to read, the figures were:
- 32% voted for “Alcohol is a relaxant, reduces stress, and can contain resveratrol too. It’s good for the heart!”
- 32% voted for: “Moderate alcohol consumption can be at least neutral for the health, if not positive ⚖️”
- 36% voted for: “Alcohol is bad for pretty much everything, including heart health ✋”
One subscriber who voted for “Alcohol is a relaxant, reduces stress, and can contain resveratrol too. It’s good for the heart!” added the following thoughts:
❝While it isn’t necessary to consume alcohol, moderate amounts can be beneficial and contribute to well-being through social activity, celebrations, etc.❞
That’s an interesting point, and definitely many people do see alcohol that way! Of course, that does not mean that one will find no social activities, celebrations, etc, in parts of the world where alcohol consumption is uncommon. Indeed, in India, wedding parties where no alcohol is consumed can go on for days!
But, “we live in a society” and all that, and while we’re a health newsletter not a social issues newsletter, it’d be remiss of us to not acknowledge the importance of socialization for good mental health—and thus the rest of our health too.
So, if indeed all our friends and family drink alcohol, it can certainly make abstaining more of a challenge.
On that note, let’s take a moment to consider “The French Paradox” (an observation of a low prevalence of ischemic heart disease despite high intakes of saturated fat, a phenomenon accredited to the consumption of red wine).
As it happens, a comprehensive review in “Circulation”, a cardiovascular health journal, has suggested the French Paradox may not be so paradoxical after all.
Research suggests it has more to do with other lifestyle factors (and historic under-reporting of cardiovascular disease by French doctors), which would explain why Japan has lower rates of heart disease, despite drinking little wine, and more beer and spirits.
So, our subscriber’s note may not be completely without reason! It’s just about the party, not the alcohol.
One subscriber who voted for “Moderate alcohol consumption can be at least neutral for the health, if not positive ⚖️” wrote:
❝Keeping in mind, moderate means one glass of wine for women a day and two for men. Hard alcohol doesn’t have the same heart benefits as wine❞
That is indeed the guideline according to some health bodies!
In other places with different guiding advisory bodies, that’s been dropped down to one a day for everyone (the science may be universal, but how government institutions interpret that is not).
About that wine… Specifically, red wine, for its resveratrol content:
While there are polyphenols such as resveratrol in red wine that could boost heart health, there’s so little per glass that you may need 100–1000 glasses to get the dosage that provides benefits in mouse studies. If you’re not a mouse, you might even need more.
To this end, many people prefer resveratrol supplementation. ← link is to an example product, but there are plenty more so feel free to shop around
A subscriber who voted for “Alcohol is bad for pretty much everything, including heart health ✋” says:
❝New guidelines suggest 1 to 2 drinks a week are okay but the less the better.❞
If you haven’t heard these new guidelines, we’ll mention again: every government has its own official bodies and guidelines so perhaps your local guidelines differ, but for example here’s what that World Health Organization has to say (as of January this year):
WHO: No level of alcohol consumption is safe for our health
So, whom to believe? The governments who hopefully consider the welfare of their citizenry more important than the tax dollars from alcohol sales, or the World Health Organization?
It’s a tough one, but we’ll always err on the side of the science.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: