The Surprising Link Between Type 2 Diabetes & Alzheimer’s
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Surprising Link Between Type 2 Diabetes & Alzheimer’s
This is Dr. Rhonda Patrick. She’s a biomedical scientist with expertise in the areas of aging, cancer, and nutrition. In the past five years she has expanded her research of aging to focus more on Alzheimer’s and Parkinson’s, as she has a genetic predisposition to both.
What does that genetic predisposition look like? People who (like her) have the APOE-ε4 allele have a twofold increased risk of Alzheimer’s disease—and if you have two copies (i.e., one from each of two parents), the risk can be up to tenfold. Globally, 13.7% of people have at least one copy of this allele.
So while getting Alzheimer’s or not is not, per se, hereditary… The predisposition to it can be passed on.
What’s on her mind?
Dr. Patrick has noted that, while we don’t know for sure the causes of Alzheimer’s disease, and can make educated guesses only from correlations, the majority of current science seems to be focusing on just one: amyloid plaques in the brain.
This is a worthy area of research, but ignores the fact that there are many potential Alzheimer’s disease mechanisms to explore, including (to count only mainstream scientific ideas):
- The amyloid hypothesis
- The tau hypothesis
- The inflammatory hypothesis
- The cholinergic hypothesis
- The cholesterol hypothesis
- The Reelin hypothesis
- The large gene instability hypothesis
…as well as other strongly correlated factors such as glucose hypometabolism, insulin signalling, and oxidative stress.
If you lost your keys and were looking for them, and knew at least half a dozen places they might be, how often would you check the same place without paying any attention to the others?
To this end, she notes about those latter-mentioned correlated factors:
❝50–80% of people with Alzheimer’s disease have type 2 diabetes; there is definitely something going on❞
There’s another “smoking gun” for this too, because dysfunction in the blood vessels and capillaries that line the blood-brain barrier seem to be a very early event that is common between all types of dementia (including Alzheimer’s) and between type 2 diabetes and APOE-ε4.
Research is ongoing, and Dr. Patrick is at the forefront of that. However, there’s a practical take-away here meanwhile…
What can we do about it?
Dr. Patrick hypothesizes that if we can reduce the risk of type 2 diabetes, we may reduce the risk of Alzheimer’s with it.
Obviously, avoiding diabetes if possible is a good thing to do anyway, but if we’re aware of an added risk factor for Alzheimer’s, it becomes yet more important.
Of course, all the usual advices apply here, including a Mediterranean diet and regular moderate exercise.
Three other things Dr. Patrick specifically recommends (to reduce both type 2 diabetes risk and to reduce Alzheimer’s risk) include:
(links are to her blog, with lots of relevant science for each)
You can also hear more from Dr. Patrick personally, as a guest on Dr. Peter Attia’s podcast recently. She discusses these topics in much greater detail than we have room for in our newsletter:
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Our family is always glued to separate devices. How can we connect again?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Saturday afternoon and the kids are all connected to separate devices. So are the parents. Sounds familiar?
Many families want to set ground rules to help them reduce their screen time – and have time to connect with each other, without devices.
But it can be difficult to know where to start and how to make a plan that suits your family.
First, look at your own screen time
Before telling children to “hop off the tech”, it’s important parents understand how much they are using screens themselves.
Globally, the average person spends an average of six hours and 58 minutes on screens each day. This has increased by 13%, or 49 minutes, since 2013.
Parents who report high screen time use tend to see this filtering down to the children in their family too. Two-thirds of primary school-aged children in Australia have their own mobile screen-based device.
Australia’s screen time guidelines recommended children aged five to 17 years have no more than two hours of sedentary screen time (excluding homework) each day. For those aged two to five years, it’s no more than one hour a day. And the guidelines recommend no screen time at all for children under two.
Yet the majority of children, across age groups, exceed these maximums. A new Australian study released this week found the average three-year-old is exposed to two hours and 52 minutes of screen time a day.
Some screen time is OK, too much increases risks
Technology has profoundly impacted children’s lives, offering both opportunities and challenges.
On one hand, it provides access to educational resources, can develop creativity, facilitates communication with peers and family members, and allows students to seek out new information.
On the other hand, excessive screen use can result in too much time being sedentary, delays in developmental milestones, disrupted sleep and daytime drowsiness.

Disrupted sleep can leave children tired the next day.
Yulia Raneva/ShutterstockToo much screen time can affect social skills, as it replaces time spent in face-to-face social interactions. This is where children learn verbal and non-verbal communication, develop empathy, learn patience and how to take turns.
Many families also worry about how to maintain a positive relationship with their children when so much of their time is spent glued to screens.
What about when we’re all on devices?
When families are all using devices simultaneously, it results in less face-to-face interactions, reducing communication and resulting in a shift in family dynamics.
The increased use of wireless technology enables families to easily tune out from each other by putting in earphones, reducing the opportunity for conversation. Family members wearing earphones during shared activities or meals creates a physical barrier and encourages people to retreat into their own digital worlds.
Wearing earphones for long periods may also reduce connection to, and closeness with, family members. Research from video gaming, for instance, found excessing gaming increases feelings of isolation, loneliness and the displacement of real-world social interactions, alongside weakened relationships with peers and family members.
How can I set screen time limits?
Start by sitting down as a family and discussing what limits you all feel would be appropriate when using TVs, phones and gaming – and when is an appropriate time to use them.
Have set rules around family time – for example, no devices at the dinner table – so you can connect through face-to-face interactions.
One rule might be no devices at the dinner table.
Monkey Business Images/ShutterstockConsider locking your phone or devices away at certain periods throughout the week, such as after 9pm (or within an hour of bedtime for younger children) and seek out opportunities to balance your days with physical activities, such kicking a footy at the park or going on a family bush walk.
Parents can model healthy behaviour by regulating and setting limits on their own screen time. This might mean limiting your social media scrolling to 15 or 30 minutes a day and keeping your phone in the next room when you’re not using it.
When establishing appropriate boundaries and ensuring children’s safety, it is crucial for parents and guardians to engage in open communication about technology use. This includes teaching critical thinking skills to navigate online content safely and employing parental control tools and privacy settings.
Parents can foster a supportive and trusting relationship with children from an early age so children feel comfortable discussing their online experiences and sharing their fears or concerns.
For resources to help you develop your own family’s screen time plan, visit the Raising Children Network.

Elise Waghorn, Lecturer, School of Education, RMIT University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Healthy Homemade Flatbreads
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our recipes sometimes call for the use of flatbreads, or suggest serving with flatbreads. But we want you to be able to have healthy homemade ones! So here’s a very quick and easy recipe. You’ll probably need to order some of the ingredients in, but it’s worth it, and then if you keep a stock of the ingredients, you can whip these up in minutes anytime you want them.
You will need
- 1 cup garbanzo bean flour, plus more for dusting
- 1 cup quinoa flour
- 2 tbsp ground/milled flaxseed
- 1 tbsp baking powder
- 1 tbsp extra virgin olive oil, plus more for the pan
- ½ tsp MSG, or 1 tsp low-sodium salt, with MSG being the healthier and preferable option
- ½ tsp onion powder
- ½ tsp garlic powder
- ½ tsp dried cumin
- ½ tsp dried thyme
Method
(we suggest you read everything at least once before doing anything)
1) Mix the flaxseed with ⅓ cup of water and set aside for at least 5 minutes.
2) Combine the rest of the ingredients in a big bowl, plus the flax mixtures we just made, and an extra ½ cup of water. Knead this into a dough, adding a touch more water if it becomes necessary, but be sparing with it.
3) Divide the dough into 6 equal portions, shaping each into a ball. Dust a clean surface with the extra garbanzo bean flour, and roll each dough ball into in a thin 6″ circle.
4) Heat a skillet and add some olive oil for frying; when hot enough, place a dough disk in the pan and cook for a few minutes on each side until golden brown. Repeat with the other 5.
5) Serve! If you’re looking for a perfect accompaniment to these, try our Hero Homemade Hummus
Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
Take care!
Share This Post
-

Come Together – by Dr. Emily Nagoski
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
From Dr. Emily Nagoski, author of the bestseller “Come As You Are” (which we reviewed very favorably before) we now present: Come Together.
What it is not about: simultaneous orgasms. The title is just a play on words.
What it is about: improving sexual wellbeing, particularly in long-term relationships where one or more partner(s) may be experiencing low desire.
Hence: come together, in the closeness sense.
A lot of books (or advice articles) out there take the Cosmo approach of “spicing things up”, and that can help for a night perhaps, but relying on novelty is not a sustainable approach.
Instead, what Dr. Nagoski outlines here is a method for focusing on shared comfort and pleasure over desire, creating the right state of mind that’s more conducive to sexuality, and reducing things that put the brakes on sexuality.
She also covers things whereby sexuality can often be obliged to change (for example, with age and/or disability), but that with the right attitude, change can sometimes just be growth in a different way, as you explore the new circumstances together, and continue to find shared pleasure in the ways that best suit your changing circumstances,
Bottom line: if you and/or your partner(s) would like to foster and maintain intimacy and pleasure, then this is a top-tier book for you.
Click here to check out Come Together, and, well, come together!
Share This Post



Related Posts
-

State of Slim – by Dr. James Hill & Dr. Holly Wyatt
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The premise of this book is “people in Colorado are on average the slimmest in the US”, and sets about establishing why, and then doing what Coloradans are doing. As per the subtitle (drop 20 pounds in 8 weeks), this is a weight loss book and does assume that you want to lose weight—specifically, to lose fat. So if that’s not your goal, you can skip this one already.
The authors explain, as many diet and not-diet-but-diet-adjacent book authors do, that this is not a diet—and then do refer to it as the Colorado Diet throughout. So… Is it a diet?
The answer is a clear “yes, but”—and the caveat is “yes, but also some associated lifestyle practices”.
The diet component is basically a very low-carb diet to start with (with the day’s ration of carbs being a small amount of oats and whatever you can get from some non-starchy vegetables such as greens, tomatoes, etc), and then reintroducing more carbohydrate centric foods one by one, stopping after whole grains. If you are vegan or vegetarian, you can also skip this one already, because this advises eating six animal protein centric meals per day.
The non-diet components are very general healthy-living advices mixed in with popular “diet culture” advices, such as practice mindful eating, don’t eat after 8pm, exercise more, use small plates, enjoy yourself, pre-portion your snacks, don’t drink your calories, get 8 hours sleep, weigh all your food, etc.
Bottom line: this is a very mixed bag, even to the point of being a little chaotic. It gives sometimes contradictory advice, and/but this results in a very “something for everyone” cafeteria approach to dieting. The best recommendation we can give for this book is “it has very many ideas for you to try and see if they work for you”.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Longevity for the Lazy – by Dr. Richard Malish
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There are some people who devote all their resources to longevity, which can become a full-time occupation, not to mention a very expensive endeavor. This book’s for those who want to get the best possible “bang for buck” by doing the things that have the most favorable cost:worth ratio.
Dr. Malish covers what can be done easily for personal longevity, as well as what technological advances can be enjoyed that those before us didn’t have as options. He also discusses the diseases that are most likely to kill us, and how to avoid those.
He preaches a proactive approach, but one that is simple and consistent and based in good science, and good statistics. Indeed, while he’s served 20 years as an army doctor and a cardiologist, he now works as a healthcare policy consultant, so he is well-placed to advise.
The style of the book is halfway between regular pop-science and a textbook; you can either read it cover-to-cover, or skim first though the key points, highlight boxes, summaries, and the like. He also provides a time-phased task list, for those who like things to be laid out like that.
Bottom line: this is a very good, methodical guide to living longer without making it a full-time occupation.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What are ‘collarium’ sunbeds? Here’s why you should stay away
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Reports have recently emerged that solariums, or sunbeds – largely banned in Australia because they increase the risk of skin cancer – are being rebranded as “collarium” sunbeds (“coll” being short for collagen).
Commercial tanning and beauty salons in Queensland, New South Wales and Victoria are marketing collariums, with manufacturers and operators claiming they provide a longer lasting tan and stimulate collagen production, among other purported benefits.
A collarium sunbed emits both UV radiation and a mix of visible wavelength colours to produce a pink or red light. Like an old-school sunbed, the user lies in it for ten to 20 minute sessions to quickly develop a tan.
But as several experts have argued, the providers’ claims about safety and effectiveness don’t stack up.
Why were sunbeds banned?
Commercial sunbeds have been illegal across Australia since 2016 (except for in the Northern Territory) under state-based radiation safety laws. It’s still legal to sell and own a sunbed for private use.
Their dangers were highlighted by young Australians including Clare Oliver who developed melanoma after using sunbeds. Oliver featured in the No Tan Is Worth Dying For campaign and died from her melanoma at age 26 in 2007.
Sunbeds lead to tanning by emitting UV radiation – as much as six times the amount of UV we’re exposed to from the summer sun. When the skin detects enough DNA damage, it boosts the production of melanin, the brown pigment that gives you the tanned look, to try to filter some UV out before it hits the DNA. This is only partially successful, providing the equivalent of two to four SPF.
Essentially, if your body is producing a tan, it has detected a significant amount of DNA damage in your skin.
Research shows people who have used sunbeds at least once have a 41% increased risk of developing melanoma, while ten or more sunbed sessions led to a 100% increased risk.
In 2008, Australian researchers estimated that each year, sunbeds caused 281 cases of melanoma, 2,572 cases of squamous cell carcinoma (another common type of skin cancer), and $3 million in heath-care costs, mostly to Medicare.
How are collarium sunbeds supposed to be different?
Australian sellers of collarium sunbeds imply they are safe, but their machine descriptions note the use of UV radiation, particularly UVA.
UVA is one part of the spectrum of UV radiation. It penetrates deeper into the skin than UVB. While UVB promotes cancer-causing mutations by discharging energy straight into the DNA strand, UVA sets off damage by creating reactive oxygen species, which are unstable compounds that react easily with many types of cell structures and molecules. These damage cell membranes, protein structures and DNA.
Evidence shows all types of sunbeds increase the risk of melanoma, including those that use only UVA.
Some manufacturers and clinics suggest the machine’s light spectrum increases UV compatibility, but it’s not clear what this means. Adding red or pink light to the mix won’t negate the harm from the UV. If you’re getting a tan, you have a significant amount of DNA damage.
Collagen claims
One particularly odd claim about collarium sunbeds is that they stimulate collagen.
Collagen is the main supportive tissue in our skin. It provides elasticity and strength, and a youthful appearance. Collagen is constantly synthesised and broken down, and when the balance between production and recycling is lost, the skin loses strength and develops wrinkles. The collagen bundles become thin and fragmented. This is a natural part of ageing, but is accelerated by UV exposure.
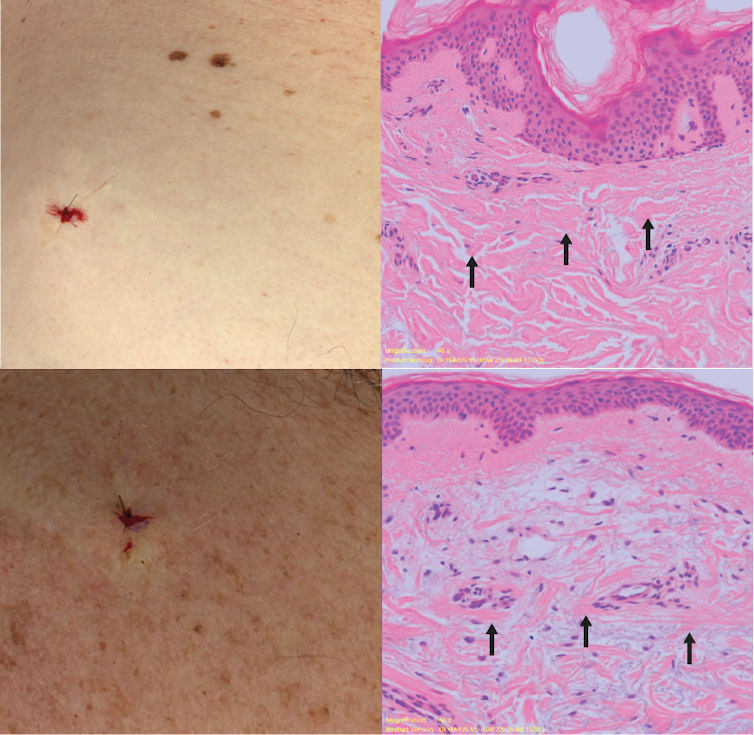
Sun-protected skin (top) has thick bands of pink collagen (arrows) in the dermis, as seen on microscopic examination. Chronically sun-damaged skin (bottom) has much thinner collagen bands.
Katie Lee/UQThe reactive oxygen species generated by UVA light damage existing collagen structures and kick off a molecular chain of events that downgrades collagen-producing enzymes and increases collagen-destroying enzymes. Over time, a build-up of degraded collagen fragments in the skin promotes even more destruction.
While there is growing evidence red light therapy alone could be useful in wound healing and skin rejuvenation, the UV radiation in collarium sunbeds is likely to undo any benefit from the red light.
What about phototherapy?
There are medical treatments that use controlled UV radiation doses to treat chronic inflammatory skin diseases like psoriasis.
The anti-collagen effects of UVA can also be used to treat thickened scars and keloids. Side-effects of UV phototherapy include tanning, itchiness, dryness, cold sore virus reactivation and, notably, premature skin ageing.
These treatments use the minimum exposure necessary to treat the condition, and are usually restricted to the affected body part to minimise risks of future cancer. They are administered under medical supervision and are not recommended for people already at high risk of skin cancer, such as people with atypical moles.
So what happens now?
It looks like many collariums are just sunbeds rebranded with red light. Queensland Health is currently investigating whether these salons are breaching the state’s Radiation Safety Act, and operators could face large fines.
As the 2024 Australians of the Year – melanoma treatment pioneers Georgina Long and Richard Scolyer – highlighted in their acceptance speech, “there is nothing healthy about a tan”, and we need to stop glamorising tanning.
However, if you’re desperate for the tanned look, there is a safer and easy way to get one – out of a bottle or by visiting a salon for a spray tan.
Katie Lee, PhD Candidate, Dermatology Research Centre, The University of Queensland and Anne Cust, Professor of Cancer Epidemiology, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: