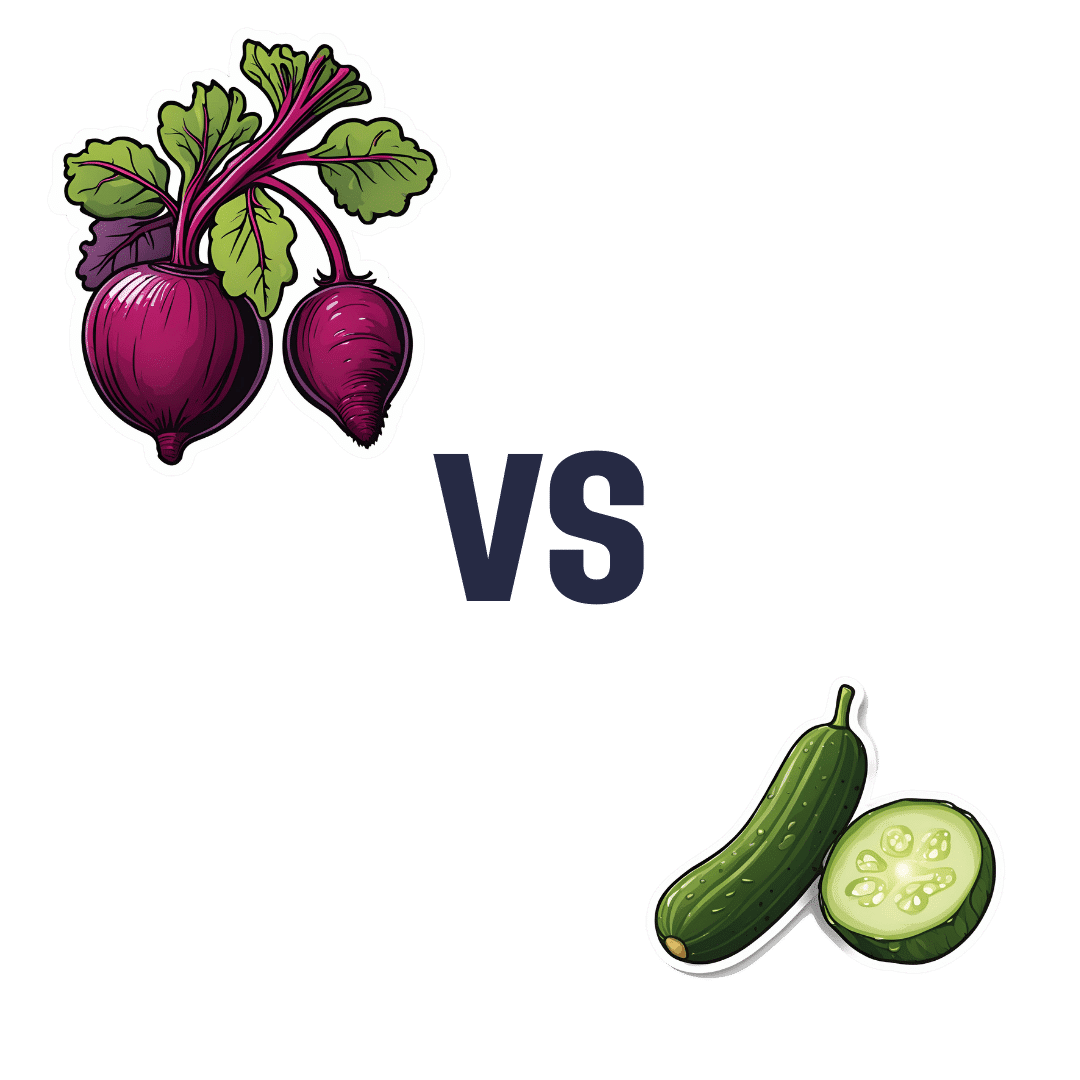
Beetroot vs Cucumber – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing beetroot to cucumber, we picked the beetroot.
Why?
While they’re both mostly-water vegetables that can go in salads, soups, and sauces, they have some notable differences:
In terms of macros, beetroot has nearly 3x the carbs and/but also nearly 6x the fiber, so we say beetroot wins this category.
On the vitamins front, beetroot has more of vitamins B1, B2, B3, B6, B7, B9, C, and E, while cucumber has more of vitamins A, B5, and K. In short, a clear win for beetroot.
In the category of minerals, beetroot has more copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while cucumber is not richer in any minerals.
When it comes to beneficial phytochemicals, both have good things to offer, though we say beetroot has more. Notably, cucumber extract beats glucosamine and chondroitin for reducing joint inflammation, at 1/135th of the dose. On the other hand, beetroot’s phytochemical benefits are so numerous we’ll not list them here, and just recommend checking out the link below!
In short, a win in all categories for beetroot, but cucumbers are great too, so by all means enjoy either or both!
Want to learn more?
You might like to read:
Beetroot For More Than Just Your Blood Pressure
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Paracetamol pack sizes and availability are changing. Here’s what you need to know

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Changes are coming into effect from February 1 about how paracetamol is sold in Australia.
This mainly affects pack sizes of paracetamol sold outside pharmacies and how paracetamol is accessed in pharmacies.
The changes, announced by Australia’s drug regulator, are in line with moves internationally to reduce the harms of liver toxicity and the risk of overdose.
However, there are no new safety concerns when paracetamol is used as directed. And children’s products are not affected.

Bowonpat Sakaew/Shutterstock What is paracetamol?
Paracetamol is commonly sold under brand names such as Panadol, Dymadon and Panamax. It’s used to treat mild pain and fever for short periods or can be prescribed for chronic (long-term) pain.
Millions of packs of this cheap and accessible medicine are sold in Australia every year.
Small packs (up to 20 tablets) have been available from supermarkets and other retailers such as petrol stations. Larger packs (up to 100 tablets) are only available from pharmacies.
Paracetamol is relatively safe when used as directed. However, at higher-than-recommended doses, it can cause liver toxicity. In severe cases and when left untreated, this can be lethal.
Why are the rules changing?
In 2022, we wrote about how the Therapeutic Goods Administration (TGA) was considering changes to paracetamol access because of an increase in people going to hospital with paracetamol poisoning.
An expert review it commissioned found there were about 40–50 deaths every year from paracetamol poisoning between 2007 and 2020. Between 2009–10 and 2016–17, hospital admissions for this increased (from 8,617 to 11,697), before reducing in 2019–20 (8,723). Most admissions were due to intentional self-poisonings, and about half of these were among people aged ten to 24.
After the report, the TGA consulted with the public to work out how to prevent paracetamol poisonings.
Options included reducing pack sizes, limiting how many packs could be bought at once, moving larger packs behind the pharmacy counter and restricting access by age.
Responses were mixed. Although responses supported the need to prevent poisonings, there were concerns about how changes might affect:
- people with chronic pain, especially those in regional areas, where it may be harder to access pharmacies and, therefore, larger packs
- people on limited incomes, if certain products were made prescription-only.
Although deaths from paracetamol poisoning are tragic and preventable, they are rare considering how much paracetamol Australians use. There is less than one death due to poisoning for every million packs sold.
Because of this, it was important the TGA addressed concerns about poisonings while making sure Australians still had easy access to this essential medicine.
If you buy large packs of paracetamol for chronic pain, you’ll need to go to the pharmacy counter. StratfordProductions/Shutterstock So what’s changing?
The key changes being introduced relate to new rules about the pack sizes that can be sold outside pharmacies, and the location of products sold in pharmacies.
From February 1, packs sold in supermarkets and places other than pharmacies will reduce from a maximum 20 tablets to 16 tablets per pack. These changes bring Australia in line with other countries. These include the United Kingdom, which restricted supermarket packs to 16 tablets in 1998, and saw reductions in poisonings.
In all jurisdictions except Queensland and Western Australia, packs sold in pharmacies larger than 50 tablets will move behind the pharmacy counter and can only be sold under pharmacist supervision. In Queensland and WA, products containing more than 16 tablets will only be available from behind the pharmacy counter and sold under pharmacist supervision.
In all jurisdictions, any packs containing more than 50 tablets will need to be sold in blister packs, rather than bottles.
Several paracetamol products are not affected by these changes. These include children’s products, slow-release formulations (for example, “osteo” products), and products already behind the pharmacy counter or only available via prescription.
What else do I need to know?
These changes have been introduced to reduce the risk of poisonings from people exceeding recommended doses. The overall safety profile of paracetamol has not changed.
Paracetamol is still available from all current locations and there are no plans to make it prescription-only or remove it from supermarkets altogether. Many companies have already been updating their packaging to ensure there are no gaps in supply.
The reduction in pack sizes of paracetamol available in supermarkets means a pack of 16 tablets will now last two days instead of two-and-a-half days if taken at the maximum dose (two tablets, four times a day). Anyone in pain that does not improve after short-term use should speak to their pharmacist or GP.
For people who use paracetamol regularly for chronic pain, it is more cost-effective to continue buying larger packs from pharmacies. As larger packs (50+ tablets) need to be kept out of sight, you will need to ask at the pharmacy counter. Pharmacists know that for many people it’s appropriate to use paracetamol daily for chronic pain.
Natasa Gisev, Clinical pharmacist and Scientia Associate Professor at the National Drug and Alcohol Research Centre, UNSW Sydney and Ria Hopkins, Postdoctoral Research Fellow, National Drug and Alcohol Research Centre, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

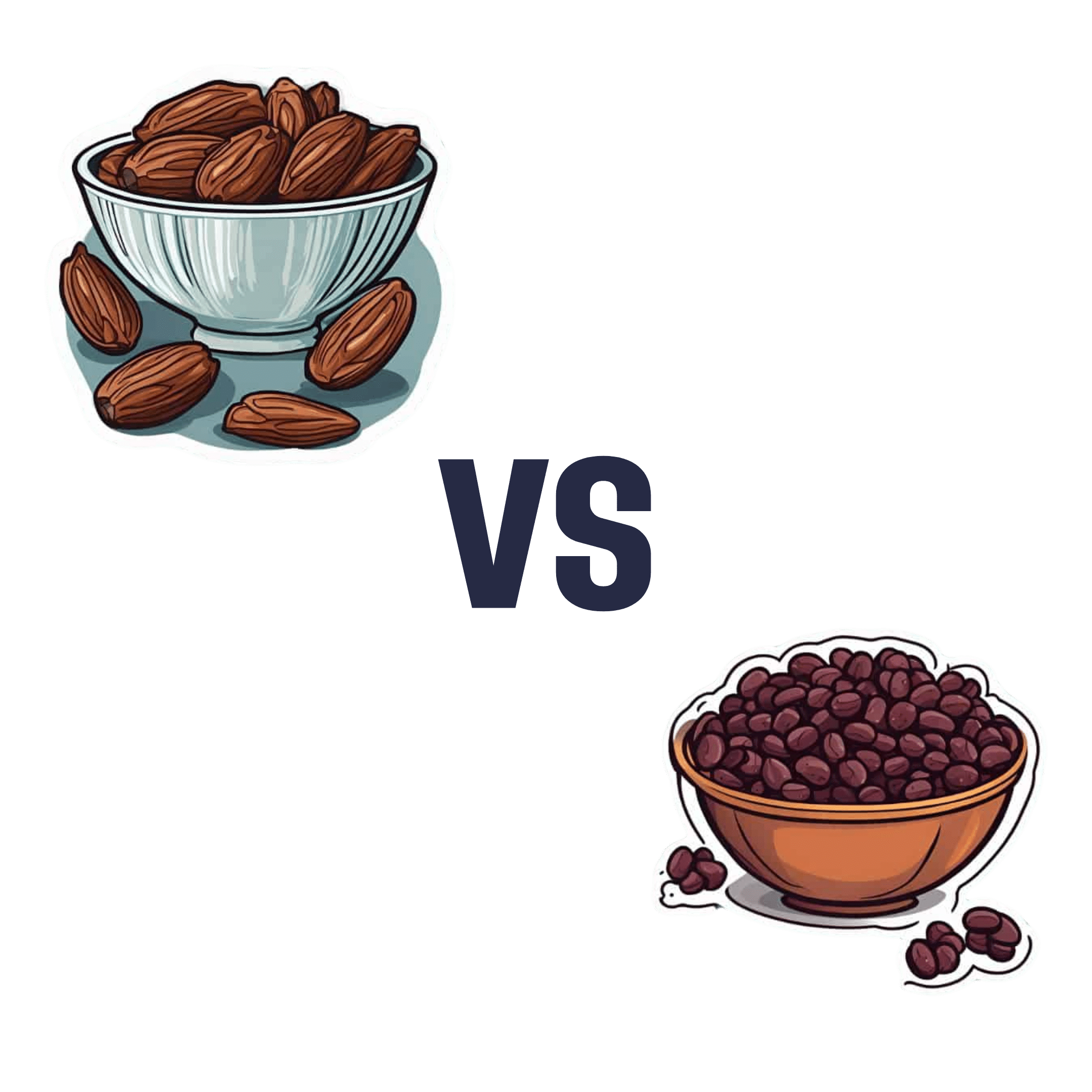
Dates vs Raisins – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing dates to raisins, we picked the dates.
Why?
There are benefits for each fruit, but we say dates come out on top. See what you think:
In terms of macros, while they’re both dried fruits, dates contain more water (unless you leave them sitting open for a while), which will tend to mathematically lower the relative percentages of other components because they’re being held against water weight too. However, even though this is the case (i.e. dates are being mathematically disadvantaged), dates contain more than twice the fiber that raisins do (8g/100g compared to raisins’ 3.7g/100g).
While we’re talking macros, dates are also lower in total carbs, as well as obviously net carbs, and have a much lower glycemic index than raisins (dates have a glycemic index of 42, considered low, while raisins have a glycemic index of 64, considered medium; their respective glycemic loads are even more telling: 13 for raisins and just 2 for dates!).
About those carbs… For dates, it’s an approximately equal mix of sucrose, glucose, and fructose, while for raisins it’s 49% glucose and 49% fructose. Because sucrose is the only disaccharide here, this (as well as the fiber difference) is one of the reasons for the different glycemic indices and glycemic loads, since glucose and fructose are more quickly absorbed.
That’s more than we usually write about macros, but in this case, both fruits are ones especially often hit with the “aren’t they full of sugar though?” question, so it was important to cover the critical distinctions between the two, because they really are very different.
Summary of macros: dates win easily in every aspect we looked at
In the category of vitamins, raisins get a tally in their favor. Raisins are higher in vitamins B1, B2, C, E, K, and choline, while dates are higher in vitamins A, B3, B5, and B9, giving raisins a 6:4 lead here. In dates’ defense, the difference in vitamin K is marginal, and it’d make it a 5:4 lead if we considered that within the margin of error (because all these figures are of course based on averages), and the vitamins that dates are higher in, the margins are much wider indeed, meaning that both fruits have approximately the same overall levels of vitamins when looked at in total, but still, we’ll call this category a nominal win for raisins.
When it comes to minerals, dates have more magnesium, selenium, and zinc, while raisins have more copper, iron, phosphorus, and potassium. Nominally that’s a 4:3 lead for raisins, but if we consider that raisins also contain more sodium, it’s more like a tie here. If we have to pick one though, this is a very slight win for raisins.
Adding up the sections, we have one huge win for dates (macros) with two very marginal wins for raisins—hence, we say that dates win out.
Still, of course enjoy both; diversity is good for the health.
Want to learn more?
You might like to read:
Which Sugars Are Healthier, And Which Are Just The Same?
Take care!
Share This Post
-
Can you die from long COVID? The answer is not so simple
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Nearly five years into the pandemic, COVID is feeling less central to our daily lives.
But the virus, SARS-CoV-2, is still around, and for many people the effects of an infection can be long-lasting. When symptoms persist for more than three months after the initial COVID infection, this is generally referred to as long COVID.
In September, Grammy-winning Brazilian musician Sérgio Mendes died aged 83 after reportedly having long COVID.
Australian data show 196 deaths were due to the long-term effects of COVID from the beginning of the pandemic up to the end of July 2023.
In the United States, the Centers for Disease Control and Prevention reported 3,544 long-COVID-related deaths from the start of the pandemic up to the end of June 2022.
The symptoms of long COVID – such as fatigue, shortness of breath and “brain fog” – can be debilitating. But can you die from long COVID? The answer is not so simple.
Jan Krava/Shutterstock How could long COVID lead to death?
There’s still a lot we don’t understand about what causes long COVID. A popular theory is that “zombie” virus fragments may linger in the body and cause inflammation even after the virus has gone, resulting in long-term health problems. Recent research suggests a reservoir of SARS-CoV-2 proteins in the blood might explain why some people experience ongoing symptoms.
We know a serious COVID infection can damage multiple organs. For example, severe COVID can lead to permanent lung dysfunction, persistent heart inflammation, neurological damage and long-term kidney disease.
These issues can in some cases lead to death, either immediately or months or years down the track. But is death beyond the acute phase of infection from one of these causes the direct result of COVID, long COVID, or something else? Whether long COVID can directly cause death continues to be a topic of debate.
Of the 3,544 deaths related to long COVID in the US up to June 2022, the most commonly recorded underlying cause was COVID itself (67.5%). This could mean they died as a result of one of the long-term effects of a COVID infection, such as those mentioned above.
COVID infection was followed by heart disease (8.6%), cancer (2.9%), Alzheimer’s disease (2.7%), lung disease (2.5%), diabetes (2%) and stroke (1.8%). Adults aged 75–84 had the highest rate of death related to long COVID (28.8%).
These findings suggest many of these people died “with” long COVID, rather than from the condition. In other words, long COVID may not be a direct driver of death, but rather a contributor, likely exacerbating existing conditions.
The symptoms of long COVID can be debilitating. Lysenko Andrii/Shutterstock ‘Cause of death’ is difficult to define
Long COVID is a relatively recent phenomenon, so mortality data for people with this condition are limited.
However, we can draw some insights from the experiences of people with post-viral conditions that have been studied for longer, such as myalgic encephalomyelitis or chronic fatigue syndrome (ME/CFS).
Like long COVID, ME/CFS is a complex condition which can have significant and varied effects on a person’s physical fitness, nutritional status, social engagement, mental health and quality of life.
Some research indicates people with ME/CFS are at increased risk of dying from causes including heart conditions, infections and suicide, that may be triggered or compounded by the debilitating nature of the syndrome.
So what is the emerging data on long COVID telling us about the potential increased risk of death?
Research from 2023 has suggested adults in the US with long COVID were at greater risk of developing heart disease, stroke, lung disease and asthma.
Research has also found long COVID is associated with a higher risk of suicidal ideation (thinking about or planning suicide). This may reflect common symptoms and consequences of long COVID such as sleep problems, fatigue, chronic pain and emotional distress.
But long COVID is more likely to occur in people who have existing health conditions. This makes it challenging to accurately determine how much long COVID contributes to a person’s death.
Research has long revealed reliability issues in cause-of-death reporting, particularly for people with chronic illness.
Determining the exact cause of someone’s death is not always easy. Pixabay/Pexels So what can we conclude?
Ultimately, long COVID is a chronic condition that can significantly affect quality of life, mental wellbeing and overall health.
While long COVID is not usually immediately or directly life-threatening, it’s possible it could exacerbate existing conditions, and play a role in a person’s death in this way.
Importantly, many people with long COVID around the world lack access to appropriate support. We need to develop models of care for the optimal management of people with long COVID with a focus on multidisciplinary care.
Dr Natalie Jovanovski, Vice Chancellor’s Senior Research Fellow in the School of Health and Biomedical Sciences at RMIT University, contributed to this article.
Rose (Shiqi) Luo, Postdoctoral Research Fellow, School of Health and Biomedical Sciences, RMIT University; Catherine Itsiopoulos, Professor and Dean, School of Health and Biomedical Sciences, RMIT University; Kate Anderson, Vice Chancellor’s Senior Research Fellow, RMIT University; Magdalena Plebanski, Professor of Immunology, RMIT University, and Zhen Zheng, Associate Professor, STEM | Health and Biomedical Sciences, RMIT University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post





Related Posts
-
How To Stop Ingrown Hair & Razor Bumps From Waxing & Shaving
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Simi Adedeji shares her expertise:
Staying smooth
Ingrown hairs (pseudofolliculitis) are inflamed hair follicles caused by hairs growing back into the skin—common in coarse, curly hair areas such as the underarms, pubic region, legs, and face.
It can be caused by shaving, waxing, plucking, tweezing, and more—in fact, almost anything aside from “trim it or leave it be”. This is because most methods cause irritation by cutting or pulling hair in ways that make it more likely to re-enter the skin.
Normally, it’s just a case of rash or itchy red bumps appearing a few days after hair removal. However, it can also get more pronounced, in cases of bacterial infection (true folliculitis), hyperpigmentation, or scarring (keloid or hypertrophic).
There are two main kinds of ingrown hair to be aware of:
- extra-follicular penetration: occurs after shaving—sharply cut hairs re-enter the skin beside the follicle, causing inflammation.
- trans-follicular penetration: occurs after plucking, waxing, or tweezing—trapped hair grows through the follicle wall into the skin, creating lumps.
Treatment options include:
- Hydrocortisone: reduces inflammation and redness.
- Benzoyl peroxide: antibacterial effect for inflamed areas.
- Chemical exfoliants: help stop hair from getting trapped
How to stop it from happening in the future:
- First, reset things and let it all calm down—stop shaving, waxing, or plucking for about a month—when hairs grow 10 mm or more, irritation usually resolves.
- Next, consider alternatives, such as depilatory creams, which dissolve hair, leaving a blunt or feathered tip that can still ingrow, but is less likely to than the other methods we talked about above. However, this comes with the tradeoff that the cream itself may irritate the skin.
- Then, consider long-term hair removal methods, such as laser or IPL, if you have dark hair on light skin—this is because laser/IPL superheats melanin in the hair to destroy the follicle, which means it won’t work on light hair (no melanin to superheat), and can harm dark skin (superheats the wrong melanin)—or electrolysis otherwise, which doesn’t depend on pigment. Removing the hair permanently means stopping ingrown hairs permanently, because a hair can’t ingrow if it’s not growing back at all.
If you are going to shave or wax, though, then:
- Shaving tips: shave after a warm bath or shower (or pre-soak the area with a warm towel); use shaving cream or a gentle cleanser for slip; avoid stretching your skin; use a bland, fragrance-free moisturizer afterwards; wait 3–4 days before applying glycolic acid.
- Waxing tips: wax before showering and avoid moisturizers beforehand; taking acetaminophen and antihistamines 30–45 minutes before can reduce pain and inflammation, respectively. Ibuprofen will also reduce both things (pain and inflammation).
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Skin Care Down There (Incl. Butt Acne, Hyperpigmentation, & More)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Fix Your Squat: 3 Squat Myths That Need To Die
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This also explains why these myths appeared in the first place:
Let’s get down to it
Trying to copy one “perfect” squat form for every body type can cause more harm than good (people have different builds, postures, mobility, and injury histories).
The result is often people giving wrong advice, much like an albatross might say to a penguin “flight is easy, just flap your wings like this”, or a penguin might say to an albatross “it’s perfectly safe to swim under this ice, just your breath for 15 minutes”.
Consequently, good form should focus on engaging the right muscles and moving safely, not just mimicking how a squat looks on someone else.
Furthermore, forcing a “textbook” squat that’s not right for you can make your body seek mobility from the wrong joints or overuse small stabilizing muscles, increasing compensation injury risk.
In particular, three myths are very prevalent:
- “Your knees mustn’t go past your toes”: this cue originated to help people sit back instead of bending only at the knees, but knees can and often should go past toes, for example when doing a deep and/or pistol squat. The real key is to keep your heels down and properly load your glutes while maintaining good hip and ankle mobility.
- “You must stay perfectly upright”: forcing a straight torso if your build or mobility doesn’t allow for it can cause back pain. A forward lean can be perfectly fine—especially for people with long femurs or shorter torsos—as long as your glutes and core are working properly.
- “There’s one correct squat depth”: there’s no universal rule about how low to go—it depends on your structure, injury history, and control. aim to move through the largest range of motion you can safely manage. Both deep and parallel squats have value depending on your goals. Also, even those who can squat deep can still benefit from using partial squats to target weak points, while others may stop at parallel to protect their knees or maintain control.
For more on each of these plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Squat Variations for Painful Knees (No More Pain!)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Who will look after us in our final years? A pay rise alone won’t solve aged-care workforce shortages
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Aged-care workers will receive a significant pay increase after the Fair Work Commission ruled they deserved substantial wage rises of up to 28%. The federal government has committed to the increases, but is yet to announce when they will start.
But while wage rises for aged-care workers are welcome, this measure alone will not fix all workforce problems in the sector. The number of people over 80 is expected to triple over the next 40 years, driving an increase in the number of aged care workers needed.
How did we get here?
The Royal Commission into Aged Care Quality and Safety, which delivered its final report in March 2021, identified a litany of tragic failures in the regulation and delivery of aged care.
The former Liberal government was dragged reluctantly to accept that a total revamp of the aged-care system was needed. But its weak response left the heavy lifting to the incoming Labor government.
The current government’s response started well, with a significant injection of funding and a promising regulatory response. But it too has failed to pursue a visionary response to the problems identified by the Royal Commission.
Action was needed on four fronts:
- ensuring enough staff to provide care
- building a functioning regulatory system to encourage good care and weed out bad providers
- designing and introducing a fair payment system to distribute funds to providers and
- implementing a financing system to pay for it all and achieve intergenerational equity.
A government taskforce which proposed a timid response to the fourth challenge – an equitable financing system – was released at the start of last week.
Consultation closed on a very poorly designed new regulatory regime the week before.
But the big news came at end of the week when the Fair Work Commission handed down a further determination on what aged-care workers should be paid, confirming and going beyond a previous interim determination.
What did the Fair Work Commission find?
Essentially, the commission determined that work in industries with a high proportion of women workers has been traditionally undervalued in wage-setting. This had consequences for both care workers in the aged-care industry (nurses and Certificate III-qualified personal-care workers) and indirect care workers (cleaners, food services assistants).
Aged-care staff will now get significant pay increases – 18–28% increase for personal care workers employed under the Aged Care Award, inclusive of the increase awarded in the interim decision.
The commission determined aged care work was undervalued.
Shutterstock/Toa55Indirect care workers were awarded a general increase of 3%. Laundry hands, cleaners and food services assistants will receive a further 3.96% on the grounds they “interact with residents significantly more regularly than other indirect care employees”.
The final increases for registered and enrolled nurses will be determined in the next few months.
How has the sector responded?
There has been no push-back from employer groups or conservative politicians. This suggests the uplift is accepted as fair by all concerned.
The interim increases of up to 15% probably facilitated this acceptance, with the recognition of the community that care workers should be paid more than fast food workers.
There was no criticism from aged-care providers either. This is probably because they are facing difficulty in recruiting staff at current wage rates. And because government payments to providers reflect the actual cost of aged care, increased payments will automatically flow to providers.
When the increases will flow has yet to be determined. The government is due to give its recommendations for staging implementation by mid-April.
Is the workforce problem fixed?
An increase in wages is necessary, but alone is not sufficient to solve workforce shortages.
The health- and social-care workforce is predicted to grow faster than any other sector over the next decade. The “care economy” will grow from around 8% to around 15% of GDP over the next 40 years.
This means a greater proportion of school-leavers will need to be attracted to the aged-care sector. Aged care will also need to attract and retrain workers displaced from industries in decline and attract suitably skilled migrants and refugees with appropriate language skills.
Aged care will need to attract workers from other sectors.
nastya_ph/ShutterstockThe caps on university and college enrolments imposed by the previous government, coupled with weak student demand for places in key professions (such as nursing), has meant workforce shortages will continue for a few more years, despite the allure of increased wages.
A significant increase in intakes into university and vocational education college courses preparing students for health and social care is still required. Better pay will help to increase student demand, but funding to expand place numbers will ensure there are enough qualified staff for the aged-care system of the future.

Stephen Duckett, Honorary Enterprise Professor, School of Population and Global Health, and Department of General Practice and Primary Care, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: