CBD Oil’s Many Benefits
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
CBD Oil: What Does The Science Say?
First, a quick legal (and practical) note:
CBD and THC are both derived from the hemp or cannabis plant, but only the latter has euphoriant psychoactive effects, i.e., will get you high. We’re writing here about CBD derived from hemp and not containing THC (thus, will not get you high).
Laws and regulations differ far too much from place to place for us to try to advise here, so please check your own local laws and regulations. And also, while you’re at it, with your doctor and/or pharmacist.
As ever, this newsletter is for purposes of education and enjoyment, and does not constitute any kind of legal (or medical) advice.
With that in mind, onwards to today’s research review…
CBD for Pain Relief
CBD has been popularly touted as a pain relief panacea, and there are a lot of pop-science articles out there “debunking” this, but…
The science seems to back it up. We couldn’t find studies refuting the claim (of CBD as a viable pain relief option). We did, however, find research showing it was good against:
Note that that latter (itself a research review, not a single study, hence covering a lot of bases) describes it matter-of-factly, with no caveats or weasel-words, as:
“CBD, a non-euphoriant, anti-inflammatory analgesic with CB1 receptor antagonist and endocannabinoid modulating effects”
As a quick note: all of the above is about the topical use of CBD oil, not any kind of ingestion
CBD for Anxiety/Depression
There’s a well-cited study with what honestly we think was a bit of a small sample size, but compelling results within that:
A study published in the Brazilian Journal of Psychiatry tested the anxiety levels of 57 men in a simulated public speaking test.
Compared to placebo…
- Those who received 300mg of CBD experienced significantly reduced anxiety during the test.
- Those who received either 150mg or 600mg of CBD experienced more anxiety during the test than the 300mg group
- This means there’s a sweet spot to the dosage
There was also a clinical study that found CBD to have anti-depressant effects.
The methodology was a lot more robust, but the subjects were mice. We can’t have everything in one study, apparently! There is probably a paucity of human volunteers to have their brain slices looked at after tests, though.
Anyway, what makes this study interesting is that it measured quite an assortment of biological markers in the brain, and found that the CBD had a similar physiological effect to the antidepressant imipramine.
CBD for Treating Opioid Addiction
There are a lot of studies for this, both animal and human, but we’d like to put the spotlight on a human study (with the participation of heroin users) that found:
❝Within one week, CBD significantly reduced cravings, anxiety, resting heart rate, and salivary cortisol levels. No serious adverse effects were found.❞
This is groundbreaking because the very thing about heroin is that it’s so addictive and the body rapidly needs more and more of it. You might think “duh”, but most people don’t realize this part:
Heroin is attractive because it offers (and delivers) an immediate guaranteed “downer”, instant relaxation… with none of the bad side effects of, for example, alcohol. No nausea, no hangover, nothing.
The problem is that the body gets tolerant to heroin very quickly, meaning your doses need to get bigger and more frequent to have the same effect.
Before you know it, what seemed like an affordable “self-medication for a stressful life” is very much out of control! Many doctors have personally found this out the hard way.
So, it’s ruinous:
- first to your financial health, as the costs rapidly spiral
- then to your physical health, as you either suffer from withdrawal or eventually overdose
Consequently, heroin is an incredibly easy drug to get hooked onto, and incredibly difficult to get back off.
So CBD offering relief is really a game-changer.
And more…
CBD has been well-studied and found to be effective for a lot of things, more than we could hope to cover in a single edition here.
Some further reading that may interest you includes:
- CBD against Diabetes in mice / in vitro / in humans
- CBD against neurological diseases (in general, in humans)
- CBD against arthritis in mice / in humans
- CBD specifically against the pain of rheumatoid arthritis / of osteoarthritis
Let us know if there’s any of these (or other) conditions you’d like us to look more into the CBD-related research for, because there’s a lot! You can always hit reply to any of our emails, or use the feedback widget at the bottom
Read (and shop, if you want and it’s permitted where you are):
10 Best CBD Oils of 2023, According to the Forbes Health Advisory Board
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How does the hair-loss drug finasteride work? Can it affect my mental health?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For many men the gradual thinning of hair is about more than just their appearance. Finasteride, a drug widely prescribed for the treatment of male pattern baldness has been used effectively for many years for this deeply personal problem.
Yet, behind its use are growing concerns about its link to the development of depression, anxiety, and even suicidal thoughts.
There is now critical discussion among both users and health-care professionals about the potential hazards associated with its continued use.
So how does the drug work? And what does the evidence say about the risk of developing a mental health problem?

agrobacter/Getty How does finasteride work?
Finasteride is used to treat androgenetic alopecia, also known as male pattern baldness. It works to regrow hair and prevent the further loss of hair.
One of the key causes of pattern baldness is the production of a hormone called dihydrotestosterone which the body makes from testosterone. When it binds to the follicles of hairs, it initiates a process called hair follicle miniaturisation. This is where the growth cycle of the hair becomes progressively shorter, resulting in thinner and weaker hair.
Finasteride works by blocking the enzyme that converts testosterone to dihydrotestosterone. By blocking the enzyme, dihydrotestosterone concentrations can be reduced by around 60–70% for the majority of men.
Finasteride was first approved in the late 1990s as a prescription-only medicine and is taken as a daily 1 milligram oral tablet. Medications available at a higher 5 mg daily dose are not used for baldness, but as a treatment for non-cancerous prostate enlargement.
This medication is not indicated for women, even though they can also have this type of hair loss.
How can it impact your mental health?
Changes in mental health are not listed as an established side effect in Australian guidance given to health-care professionals.
Based on clinical trials, the most common effects include:
- decreased libido
- erectile dysfunction
- reduced semen production.
The guidance also describes an increased risk of prostate cancer and a potential risk for breast cancer. Yes, men can get breast cancer too.
While initial clinical trials conducted to obtain approval for the drug didn’t demonstrate mental health concerns, monitoring of patients using the drug has since indicated a potential increased risk of depression and suicidal thoughts. But as this is based on patients self-reporting symptoms, according to the guidance there is no definitive link.
However, in May 2025, the European Medicines Agency safety committee stated suicidal thoughts was a confirmed side effect of finasteride. The European Union also advises patients that finasteride can cause a depressed mood and depression.
Similarly, in a warning about compounded finasteride, the United States Food and Drug Administration stated in April 2025 that topical formulations of the drug has similar side effects to the oral version. These include depression, anxiety and suicidal thoughts.
What should you do if it is affecting your mental health?
If you notice changes in your mental health while taking the drug, try not to handle significant mood changes by yourself. If you’re feeling unusually low, anxious or emotionally unstable, check in with a doctor so they can help you figure out whether finasteride is contributing to your mood and what support you may need.
If the symptoms are mild, they may suggest pausing finasteride to see whether things improve, or continuing with additional mental health support. If your symptoms are more severe, stopping the medication and getting prompt medical review may be appropriate.
If you are taking finasteride and are worried about its side effects, it is safe to stop immediately. Most side effects ease once the medication is out of your system, although a small number of people have reported symptoms that persist.
If you do decide to stop, this will mean that your hormone levels will gradually return to baseline and the hair growth seen with the drug will be lost over time.
If finasteride is not the right fit for you, there is another evidence-based alternative.
Topical minoxidil is a first-line treatment that can be used on its own or with other treatments and is available from pharmacies over the counter. It only works while it’s being used and may irritate the scalp, but its effectiveness is well-established and widely recommended.
While depression and anxiety are associated with minoxidil, the incidence is much lower because of their topical application.
There is also a medication called dutasteride. However, as it works in a similar way to finasteride, it may also increase your risk of developing mental health problems. So it is best to avoid dutasteride if finasteride is not suitable for you.
If this story has raised any issues for you, please contact one of the services below:
- Lifeline: 13 11 14 or lifeline.org.au
- Suicide Call Back Service (ages 15+): 1300 659 467 or suicidecallbackservice.org.au
Nial Wheate, Professor, School of Natural Sciences, Macquarie University and Jasmine Lee, Pharmacist and PhD Candidate, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

What’s the difference between vegan and vegetarian?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
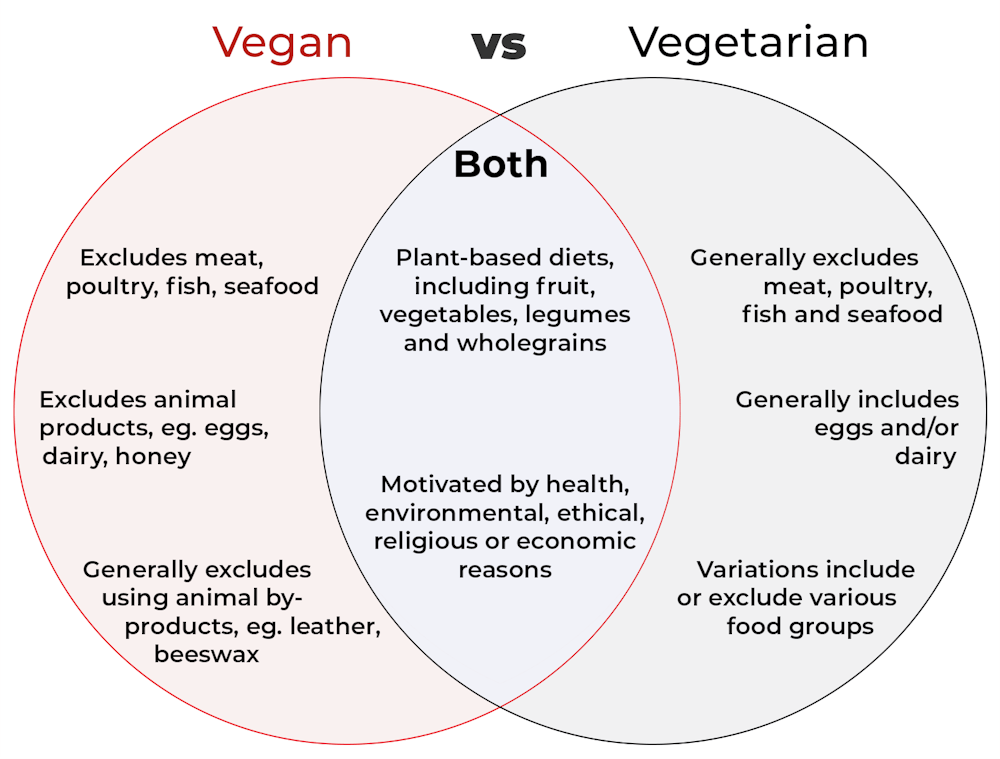
Vegan and vegetarian diets are plant-based diets. Both include plant foods, such as fruits, vegetables, legumes and whole grains.
But there are important differences, and knowing what you can and can’t eat when it comes to a vegan and vegetarian diet can be confusing.
So, what’s the main difference?
Creative Cat Studio/Shutterstock What’s a vegan diet?
A vegan diet is an entirely plant-based diet. It doesn’t include any meat and animal products. So, no meat, poultry, fish, seafood, eggs, dairy or honey.
What’s a vegetarian diet?
A vegetarian diet is a plant-based diet that generally excludes meat, poultry, fish and seafood, but can include animal products. So, unlike a vegan diet, a vegetarian diet can include eggs, dairy and honey.
But you may be wondering why you’ve heard of vegetarians who eat fish, vegetarians who don’t eat eggs, vegetarians who don’t eat dairy, and even vegetarians who eat some meat. Well, it’s because there are variations on a vegetarian diet:
- a lacto-ovo vegetarian diet excludes meat, poultry, fish and seafood, but includes eggs, dairy and honey
- an ovo-vegetarian diet excludes meat, poultry, fish, seafood and dairy, but includes eggs and honey
- a lacto-vegetarian diet excludes meat, poultry, fish, seafood and eggs, but includes dairy and honey
- a pescatarian diet excludes meat and poultry, but includes eggs, dairy, honey, fish and seafood
- a flexitarian, or semi-vegetarian diet, includes eggs, dairy and honey and may include small amounts of meat, poultry, fish and seafood.
Are these diets healthy?
A 2023 review looked at the health effects of vegetarian and vegan diets from two types of study.
Observational studies followed people over the years to see how their diets were linked to their health. In these studies, eating a vegetarian diet was associated with a lower risk of developing cardiovascular disease (such as heart disease or a stroke), diabetes, hypertension (high blood pressure), dementia and cancer.
For example, in a study of 44,561 participants, the risk of heart disease was 32% lower in vegetarians than non-vegetarians after an average follow-up of nearly 12 years.
Further evidence came from randomised controlled trials. These instruct study participants to eat a specific diet for a specific period of time and monitor their health throughout. These studies showed eating a vegetarian or vegan diet led to reductions in weight, blood pressure, and levels of unhealthy cholesterol.
For example, one analysis combined data from seven randomised controlled trials. This so-called meta-analysis included data from 311 participants. It showed eating a vegetarian diet was associated with a systolic blood pressure (the first number in your blood pressure reading) an average 5 mmHg lower compared with non-vegetarian diets.
It seems vegetarian diets are more likely to be healthier, across a number of measures.
For example, a 2022 meta-analysis combined the results of several observational studies. It concluded a vegetarian diet, rather than vegan diet, was recommended to prevent heart disease.
There is also evidence vegans are more likely to have bone fractures than vegetarians. This could be partly due to a lower body-mass index and a lower intake of nutrients such as calcium, vitamin D and protein.
But it can be about more than just food
Many vegans, where possible, do not use products that directly or indirectly involve using animals.
So vegans would not wear leather, wool or silk clothing, for example. And they would not use soaps or candles made from beeswax, or use products tested on animals.
The motivation for following a vegan or vegetarian diet can vary from person to person. Common motivations include health, environmental, ethical, religious or economic reasons.
And for many people who follow a vegan or vegetarian diet, this forms a central part of their identity.
More than a diet: veganism can form part of someone’s identity. Shutterstock So, should I adopt a vegan or vegetarian diet?
If you are thinking about a vegan or vegetarian diet, here are some things to consider:
- eating more plant foods does not automatically mean you are eating a healthier diet. Hot chips, biscuits and soft drinks can all be vegan or vegetarian foods. And many plant-based alternatives, such as plant-based sausages, can be high in added salt
- meeting the nutrient intake targets for vitamin B12, iron, calcium, and iodine requires more careful planning while on a vegan or vegetarian diet. This is because meat, seafood and animal products are good sources of these vitamins and minerals
- eating a plant-based diet doesn’t necessarily mean excluding all meat and animal products. A healthy flexitarian diet prioritises eating more whole plant-foods, such as vegetables and beans, and less processed meat, such as bacon and sausages
- the Australian Dietary Guidelines recommend eating a wide variety of foods from the five food groups (fruit, vegetables, cereals, lean meat and/or their alternatives and reduced-fat dairy products and/or their alternatives). So if you are eating animal products, choose lean, reduced-fat meats and dairy products and limit processed meats.
Katherine Livingstone, NHMRC Emerging Leadership Fellow and Senior Research Fellow at the Institute for Physical Activity and Nutrition, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

The Longevity Diet – by Dr. Valter Longo
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Another book with “The New Science” in its subtitle, so, is this one a new science?
Yes and no; some findings are new, many are not, what really sets this book apart from many of its genre though is that rather than focusing on fighting aging, it focuses on retaining youth. While this may seem like one and the same thing, there is a substantive difference beyond the ideological, which is: while anti-aging research focuses on what causes people to suffer age-related decline and fights each of those things, Dr. Longo’s research focuses on what is predominant in youthful bodies, cells, DNA, and looks to have more of that. Looking in a slightly different place means finding slightly different things, and knowledge is power indeed.
Dr. Longo bases his research and focus on his “5 pillars of longevity”. We’ll not keep them a mystery; they are:
- Juventology research
- Epidemiology
- Clinical studies
- Centenarian studies
- Study of complex systems
The first there (juventology research) may sound like needless jargon, but it is the counterpoint of the field of gerontology, and is otherwise something that didn’t have an established name.
You may wonder why “clinical studies” gets a separate item when the others already include studies; this is because many studies when it comes to aging and related topics are population-based studies, cohort studies, observational studies, or (as is often the case) multiple of the above at once.
Of course, all this discussion of academia is not itself practical information for the reader (unless we happen to work in the field), but it is interesting and does give confidence in the conclusions upon which the practical parts of the book are based.
And what are they? As the title suggests, it’s about diet, and specifically, it’s about Dr. Longo’s “fast-mimicking diet”, which boasts the benefits of intermittent fasting without intermittent fasting. This hinges, of course, on avoiding metabolic overload, which can be achieved with a fairly simple diet governed by the principles outlined in this book, based on the research referenced.
In the category of subjective criticism, there is quite a bit of fluff, much of it self-indulgently autobiographical and very complimentary, but its presence does not take anything away from the excellent content contained in the book.
Bottom line: if you’d like a fresh perspective on regaining/retaining youthfulness, then this is a great book to read.
Click here to check out The Longevity Diet, and stay younger!
Share This Post




-
Is period syncing real? Two reproductive health experts explain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Have you ever heard two or more women say they’re on the same cycle?
This is a common claim among women who live together, for example in a family or as housemates.
This idea that people menstruate, or have their period, at the same time is known as “menstrual synchrony”. If their menstrual periods happen to regularly align, they might describe themselves as being “in sync”.
But is menstrual synchrony possible, according to science? Let’s unpack the evidence.
www.kaboompics.com/Pexels The ‘menstrual synchrony’ myth
The term “menstrual synchrony” is difficult to define.
In popular culture, it’s generally thought to be the result of various unknown factors which cause two or more people to have their period at the same time. So it is supposedly due to biology, not coincidence.
Scientists also struggle to define menstrual synchrony. According to one 2023 study, it is when people’s menstrual periods start at roughly the same time, not necessarily on the same day.
But as we’ll see, research suggests being on the exact same menstrual cycle as someone else is scientifically very unlikely.
Where did this idea come from?
A psychologist named Martha McClintock likely popularised the concept of menstrual synchrony. In a 1971 study published in the journal Nature, McClintock studied 135 women aged between 17 and 22 who all lived together in a college dormitory.
Her main finding was the menstrual cycles of women who shared a room or spent lots of time together aligned over time. But this was not the case among those who lived in the same building or spent more time with men, both of which are factors that influence mating behaviour in animals.
Despite being published in a reputable and widely-read journal, today there are as many studies refuting McClintock’s 1971 study as there are supporting it. Critics mainly point to the flawed assumptions and calculations McClintock made as part of the study.
For example, when the boarders first moved in, McClintock recorded the date when each person’s period started. Several months later, she again noted the boarders’ menstrual start date. However, she did not record the length of each person’s cycle over the course of the study. That makes it hard to know whether the boarders’ periods synced purely by chance.
McClintock’s study also assumed each boarder had a standard 28-day menstrual cycle. Before the 2000s, this was widely accepted as scientific fact. But multiple landmark studies which used apps to track pregnancy and contraception show the length of a menstrual cycle can vary. We now know it commonly lasts between 28 and 35 days.
One 2017 study examined the menstrual cycles of pairs of close friends or housemates. It found three-quarters of the pairs saw the timing of their periods become less, not more, aligned. But this study was not peer-reviewed, so we must interpret it with caution.
So, why is this myth still around?
Here are three reasons.
It makes some evolutionary sense
In one 2008 study, researchers suggested menstrual synchrony could lead to greater genetic diversity among groups of primates. They argued that if multiple females are capable of reproducing at the same time, it’s less likely that one alpha male will father all offspring. In theory, this would increase the group’s long-term survival through natural selection. This is the idea that beneficial genetic mutations are passed onto the next generation through reproduction.
It’s a common misconception
Many people believe menstrual synchrony is real. This could be because they’ve noticed their period starting around the same time as a friend, housemate or family member. But they may hold onto this myth because of confirmation bias. This is the idea that people look for evidence that affirms their existing beliefs, even if they don’t do it deliberately. So confirmation bias means we’re less likely to notice the times our periods are not in sync, or to simply dismiss that possibility.
It may help women connect
One American study found 90% of women surveyed believed in menstrual synchrony. Many described it as a “magical” concept which made them feel more connected to other women. Some also said it helped them cope with the challenges of menstruation. Another study found 70% of participants said they had experienced period syncing firsthand, with most viewing menstrual synchrony as a real and positive experience.
So the evidence suggests period syncing is not scientifically supported. But it still persists in popular culture. And for some women, it may make menstruation that bit more tolerable.
Emmalee Ford, Adjunct Lecturer, Sexual and Reproductive Health, University of Sydney and Tessa Copp, NHMRC Emerging Leader Research Fellow in Reproductive Health, School of Public Health, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
How Stress Affects Your Body
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Sharon Bergquist gives us a tour:
Stress, from the inside out
Stress is a natural physical and emotional response to challenges or being overwhelmed. It can be beneficial in short-term situations (e.g. escape from a tiger) but is harmful when prolonged or frequent (e.g. escape the rat-race).
Immediate physiological response: cortisol, adrenaline (epinephrine), and norepinephrine are released by the adrenal glands.
The effects this has (non-exhaustive list; we’re just citing what’s in the video here):
- Cortisol impairs blood vessel function, promoting atherosclerosis.
- Adrenaline increases heart rate and blood pressure, leading to hypertension.
- Stress disrupts the brain-gut connection, causing:
- Digestive issues like irritable bowel syndrome and heartburn.
- Changes in gut bacteria composition, potentially affecting overall health.
- Cortisol increases appetite and cravings for energy-dense “comfort foods”.
- This in turn promotes visceral fat storage, which raises the risk of heart disease and insulin resistance.
- Immune-specific effects:
- Stress hormones initially aid in healing and immune defense.
- Chronic stress weakens immune function (by over-working it constantly), increasing susceptibility to infections and slowing recovery.
- Other systemic effects:
- Chronic stress shortens telomeres, which protect chromosomes. Shortened telomeres accelerate cellular aging.
- Chronic stress can also cause acne, hair loss, sexual dysfunction, headaches, muscle tension, fatigue, irritability, and difficulty concentrating.
So, how to manage this? The video says that viewing stressful situations as controllable challenges, rather than insurmountable threats, leads to better short-term performance and long-term health.
Which would be wonderful, except that usually things are stressful precisely because they are not entirely within the field of our control, and the usual advice is to tend to what we can control, and accept what we can’t.
However… That paradigm still leaves out the very big set of “this might be somewhat within our control or it might not; we really don’t know yet; we can probably impact it but what if we don’t do enough, or take the wrong approach and do the wrong thing? And also we have 17 competing stressors, which ones should we prioritize tending to first, and…” and so on.
To that end, we suggest checking out the “Want to learn more?” link we drop below the video today, as it is about managing stress realistically, in a world that, if we’re honest about it, can sometimes be frankly unmanageable.
Meanwhile, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Heart Health vs Systemic Stress ← this is good in and of itself, and also links to other stress-related resources of ours
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Fiber Fueled – by Dr. Will Bulsiewicz
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We generally know that for gut health we should eat fiber, but what of the balances of different sorts of fiber?
That’s one of the main things that make this book stand out—fostering diversity in our microbiome by fostering diversity in our diet. Specifically, diversity of fiber-containing foods.
The book is part “science made easy for the lay reader”, and part recipe book. The recipes come with shopping lists and a meal planner, though we would recommend to use those as a guide rather than to try to adhere perfectly to them.
In particular, this reviewer would encourage much more generous use of healthful seasonings… and less reliance on there being leftovers several days later (tasty food gets gone quickly in this house!)
As for the science, the feel of this is more like reading a science-based observational documentary with explanations, than of reading a science textbook. Studies are mentioned in passing, but not dissected in any detail, and the focus is more on getting the key learnings across.
Bottom line: if you’d like to boost not just the amount, but also the diversity, of fiber in your diet, and reap the gut-health rewards, this book is a great guide for that!
Click here to get your copy of “Fiber Fueled” from Amazon today!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: