Canned Tuna vs Canned Sardines – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing canned tuna to canned sardines, we picked the sardines.
Why?
This comparison is unfair, but practical—because both are sold next to each other in the supermarket and often used for similar things.
It’s unfair because in a can of tuna, there is tuna meat, whereas in a can of sardines, there is sardine meat, skin, and bones.
Consequently, sardines outperform tuna in almost everything, because a lot of nutrients are in the skin and bones.
To be completely unambiguous:
Sardines have more vitamins and minerals by far (special shout-out to calcium, of which sardines contain 6000% more), and more choline (which is sometimes reckoned as a vitamin, sometimes not).
Tuna does have marginally more protein, and less fat. If you are trying to limit your cholesterol intake, then that could be an argument for choosing tuna over sardines.
All in all: the sardines are more nutrient dense by far, are good sources of vitamins and minerals that tuna contains less of (and in many cases only trace amounts of), and for most people this will more than offset the difference in cholesterol, especially if having not more than one can per day.
About that skin and bones…
That’s where the real benefit for your joints lies, by the way!
See: We Are Such Stuff As Fish Are Made Of
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Will there soon be a cure for HIV?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Human immunodeficiency virus, or HIV, is a chronic health condition that can be fatal without treatment. People with HIV can live healthy lives by taking antiretroviral therapy (ART), but this medication must be taken daily in order to work, and treatment can be costly. Fortunately, researchers believe a cure is possible.
In July, a seventh person was reportedly cured of HIV following a 2015 stem cell transplant for acute myeloid leukemia. The patient stopped taking ART in 2018 and has remained in remission from HIV.
Read on to learn more about HIV, the promise of stem cell transplants, and what other potential cures are on the horizon.
What is HIV?
HIV infects and destroys the immune system’s cells, making people more susceptible to infections. If left untreated, HIV will severely impair the immune system and progress to acquired immunodeficiency syndrome (AIDS). People living with untreated AIDS typically die within three years.
People with HIV can take ART to help their immune systems recover and to reduce their viral load to an undetectable level, which slows the progression of the disease and prevents them passing the virus to others.
How can stem cell transplants cure HIV?
Several people have been cured of HIV after receiving stem cell transplants to treat leukemia or lymphoma. Stem cells are produced by the spongy tissue located in the center of some bones, and they can turn into new blood cells.
A mutation on the CCR5 gene prevents HIV from infecting new cells and creates resistance to the virus, which is why some HIV-positive people have received stem cells from donors carrying this mutation. (One person was reportedly cured of HIV after receiving stem cells without the CCR5 mutation, but further research is needed to understand how this occurred.)
Despite this promising news, experts warn that stem cell transplants can be fatal, so it’s unlikely this treatment will be available to treat people with HIV unless a stem cell transplant is needed to treat cancer. People with HIV are at an increased risk for blood cancers, such as Hodgkin lymphoma and non-Hodgkin lymphoma, which stem cell transplants can treat.
Additionally, finding compatible donors with the CCR5 mutation who share genetic heritage with patients of color can be challenging, as donors with the mutation are typically white.
What are other potential cures for HIV?
In some rare cases, people who started ART shortly after infection and later stopped treatment have maintained undetectable levels of HIV in their bodies. There have also been some people whose bodies have been able to maintain low viral loads without any ART at all.
Researchers are studying these cases in their search for a cure.
Other treatment options researchers are exploring include:
- Gene therapy: In addition to stem cell transplants, gene therapy for HIV involves removing genes from HIV particles in patients’ bodies to prevent the virus from infecting other cells.
- Immunotherapy: This treatment is typically used in cancer patients to teach their immune systems how to fight off cancer. Research has shown that giving some HIV patients antibodies that target the virus helps them reach undetectable levels of HIV without ART.
- mRNA technology: mRNA, a type of genetic material that helps produce proteins, has been used in vaccines to teach cells how to fight off viruses. Researchers are seeking a way to send mRNA to immune system cells that contain HIV.
When will there be a cure for HIV?
The United Nations and several countries have pledged to end HIV and AIDS by 2030, and a 2023 UNAIDS report affirmed that reaching this goal is possible. However, strategies to meet this goal include HIV prevention and improving access to existing treatment alongside the search for a cure, so we still don’t know when a cure might be available.
How can I find out if I have HIV?
You can get tested for HIV from your primary care provider or at your local health center. You can also purchase an at-home HIV test from a drugstore or online. If your at-home test result is positive, follow up with your health care provider to confirm the diagnosis and get treatment.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Share This Post
-
Blackberries vs Blueberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing blackberries to blueberries, we picked the blackberries.
Why?
They’re both great! But the humble blackberry stands out (and is an example of the rule-of-thumb “foods that are darker are often more nutrient-dense”).
In terms of macros, blackberries have 2x the fiber and for what it’s worth (which isn’t much because the numbers are tiny) 2x the protein, while blueberries have 2x the carbs. An easy first-round win for blackberries.
When it comes to vitamins, blackberries have notably more of vitamins A, B3, B5, B9, C, and E, while blueberries have a little more of vitamins B1, B2, and B6. Another clear win for blackberries.
In the category of minerals, blackberries have a lot more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while blueberries are not higher in any minerals, so that’s a total win for blackberries in this round!
In other considerations, blueberries are famous for their antioxidants, but blackberries actually equal them. The polyphenol content varies from one fruit to another, but they are both loaded with an abundance (thousands) of antioxidants, especially anthocyanins. So this round’s most reasonably a tie.
Adding up the sections makes for a clear overall win for blackberries, but by all means do enjoy either or both, as diversity is best!
PS: this writer has managed to get both to grow in her garden, and she lives at the edge of an ancient bog, which really limits what can be grown here. This is probably no use to you, dear reader (you are too far for me to share my blackberries and blueberries with you), but I’m proud of it :p However! If we want to make it useful, then: do consider it an exhortation to grow what you can, wherever you may be!
Want to learn more?
You might like:
21 Most Beneficial Polyphenols & What Foods Have Them
Enjoy!
Share This Post
-
Cabbage vs Spinach – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cabbage to spinach, we picked the spinach.
Why?
Why, oh why indeed? ← lamentations of this cabbage-loving writer
But more seriously:
In terms of macros, these are very similar: mostly water, small amounts of carbs and protein, and enough fiber to hold them together. The only notable point of distinction here is that cabbage higher in soluble fiber, while spinach has more insoluble fiber, however these are both important, just different, and ultimately balanced in any case, so we’ll call this round a tie.
In the category of vitamins, cabbage has more of vitamins B5 and C, while spinach has more of vitamins A, B1, B2, B3, B6, B7, B9, E, K, and choline; a clear win for spinach.
When it comes to minerals, cabbage is not higher in any minerals, and spinach has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. Another easy win for spinach.
With regard to phytochemicals, spinach has a much higher polyphenol content (mostly flavonols), and on the flipside, spinach has a much higher oxalate content (that’s not a problem for most people, but bad if you have certain kidney issues). So this category could be swung any which way depending on the state of your kidneys. For simplicity, we’ll record this round as a tie, but its constituent parts are worth bearing in mind.
Adding up the sections makes for an overall win for spinach, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
What Do The Different Kinds Of Fiber Do? 30 Foods That Rank Highest
Enjoy!
Share This Post

Related Posts
-

Rainbow Roasted Potato Salad
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This salad has potatoes in it, but it’s not a potato salad as most people know it. The potatoes are roasted, but in a non-oily-dressing, that nevertheless leaves them with an amazing texture—healthy and delicious; the best of both worlds. And the rest? We’ve got colorful vegetables, we’ve got protein, we’ve got seasonings full of healthy spices, and more.
You will need
- 1½ lbs new potatoes (or any waxy potatoes; sweet potato is also a great option; don’t peel them, whichever you choose) cut into 1″ chunks
- 1 can / 1 cup cooked cannellini beans (or your preferred salad beans)
- 1 carrot, grated
- 2 celery stalks, finely chopped
- 3 spring onions, finely chopped
- ½ small red onion, finely sliced
- 2 tbsp white wine vinegar
- 1 tbsp balsamic vinegar
- 1 tbsp lemon juice
- 1 tbsp nutritional yeast
- 1 tsp garlic powder
- 1 tsp black pepper
- ½ tsp red chili powder
- We didn’t forget salt; it’s just that with the natural sodium content of the potatoes plus the savory flavor-enhancing properties of the nutritional yeast, it’s really not needed here. Add if you feel strongly about it, opting for low-sodium salt, or MSG (which has even less sodium).
- To serve: 1 cup basil pesto (we’ll do a recipe one of these days; meanwhile, store-bought is fine, or you can use the chermoula we made the other day, ignoring the rest of that day’s recipe and just making the chermoula component)
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven as hot as it goes!
2) Combine the potatoes, white wine vinegar, nutritional yeast, garlic powder, black pepper, and red chili powder, mixing thoroughly (but gently!) to coat.
3) Spread the potatoes on a baking tray, and roast in the middle of the oven (for best evenness of cooking); because of the small size of the potato chunks, this should only take about 25 minutes (±5mins depending on your oven); it’s good to turn them halfway through, or at least jiggle them if you don’t want to do all that turning.
4) Allow to cool while still on the baking tray (this allows the steam to escape immediately, rather than the steam steaming the other potatoes, as it would if you put them in a bowl).
5) Now put them in a serving bowl, and mix in the beans, vegetables, balsamic vinegar, and lemon juice, mixing thoroughly but gently
6) Add generous lashings of the pesto to serve; it should be gently mixed a little too, so that it’s not all on top.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- White Potato vs Sweet Potato – Which is Healthier?
- Eat More (Of This) For Lower Blood Pressure
- Our Top 5 Spices: How Much Is Enough For Benefits?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Recent outbreaks highlight the risks of bacterial meningitis and the need to vaccinate
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Outbreaks of bacterial meningococcal disease in England and recent cases in students in New Zealand have raised awareness of this serious and life-threatening disease.
The disease is caused by the bacterium Neisseria meningitidis and presents as meningitis or blood poisoning (septicaemia).
Meningitis is an inflammation of the membranes that cover the brain and spinal cord (meninges), while septicaemia affects the whole body through the presence of bacteria in the blood stream.
Both can be also be caused by other infectious agents, but bacterial meningococcal disease is the most severe form.
Infants, children and young adults are at higher risk. While the disease is largely preventable through vaccination, only one vaccine is currently on the national immunisation schedule in Aotearoa New Zealand.
As part of ongoing research to explain the recent cases, we compared the meningococcal strains involved in both countries and explored the significance of people who carry the bacterium but don’t develop symptoms or disease.
There are several strains of Neisseria meningitidis and most belong to six groups (named A, B, C, W, X and Y). All have an extraordinary ability to swap genetic material between them and switch genes on and off through a process known as phase variation.
This can change the surface of the bacterium, enabling it to escape the body’s immune system.
The strains responsible for both the UK and recent Dunedin cases belong to Group B meningococci. However, the similarity ends there. The UK outbreak strain is known as ST485, while the Dunedin cases were caused by different strains. They differ from the UK strain as well as from each other, suggesting more than one chain of transmission was involved.
The Bexsero vaccine is used to protect people against bacterial meningitis caused by group B strains. It was designed to recognise components in the outer membrane and on the surface of the bacteria.
The strain that caused the UK outbreak is likely covered by the Bexero vaccine because it matches exactly one of the protein antigen sequences used in the vaccine.
But genomic sequencing of the bacteria responsible for one of the Dunedin cases is still pending, while the other case did not yield a bacterial culture.
Students and staff queue to receive antibiotics at the UK University of Kent after an outbreak of meningitis caused the deaths of two people. Carl Court/Getty Images The importance of genome sequencing
Although meningococcal disease can appear as scattered and apparently unrelated cases, these can occasionally build into larger outbreaks.
Strain typing and genome sequencing can help to determine if an apparent outbreak is due to the emergence of a particular strain or a cluster of cases that are genetically unrelated.
Both scenarios can occur if cases share a common risk factor, such as increased close contact and mixing in educational settings such as schools and universities.
Past genomic surveillance in New Zealand has shown the emergence of outbreak strains and helped identify likely resistance to antibiotics. For example, a W group strain variant caused rising numbers of meningococcal disease between 2016 and 2019 in New Zealand and an outbreak in Northland in 2018.
Genome sequencing showed this strain was different from the W strain causing disease in Europe at the time, and the specific 2015 variant also has increased resistance to penicillin.
Healthy people can be carriers
Despite its ability to cause severe disease, the bacterium causing meningococcal disease is often found in people’s throat, without causing symptoms.
About 5% to 30% of the global population are carriers, and most don’t experience any symptoms or disease. We don’t yet fully understand the factors that determine whether disease develops.
Genome sequencing has shown that some highly virulent strains which are associated with outbreaks are rarely identified in samples from healthy carriers. But as yet, attempts to find genomic explanations for differences in bacteria found in outbreaks and healthy carriers remain inconclusive.
The likelihood whether people carry the bacterium is age dependent. It is low in younger children and older people, but high in teenagers and young adults.
The high carriage rate in young adults makes university students a high-risk group for developing the disease. Crowded living conditions also contribute to the high carriage rate, exacerbating the risk.
In New Zealand, both the Bexsero (against group B) and MenQuadfi (against ACWY) vaccines are available to young people moving into boarding school or university halls the first time. In contrast, only one vaccine (against ACWY) is currently funded for university students in England.
Both vaccines are needed to have maximum protection. Conjugate ACWY vaccines may reduce carriage and therefore transmission. Bexsero does not reduce carriage but protects against development of the disease.
Impact of COVID measures on transmission
Lockdowns and border controls introduced during the COVID pandemic reduced transmission of the SARS-CoV2 virus. But they also had a major effect on other diseases, including influenza and other respiratory viruses.
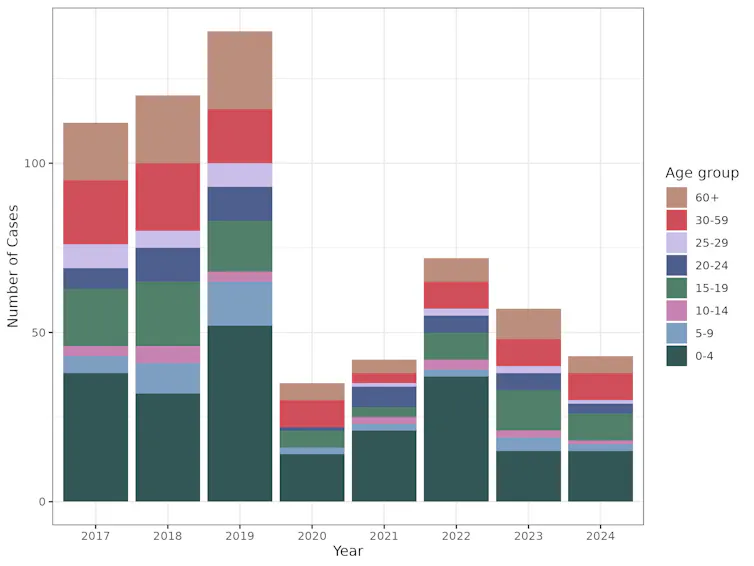
Cases of meningococcal disease were also dramatically reduced during the COVID response, most likely due to reduced contact between individuals and because fewer infected people entered the country.
This graph shows the drop in cases of meningococcal disease, across all age groups, during the period of COVID lockdowns. Data extracted from the PHF Science notifiable disease dashboard for meningococcal disease, CC BY-SA The rebound in cases following relaxation of these strict measures was expected.
This highlights how important it is to be aware of the risks associated with large gatherings, particularly of young people, and the need to vaccinate with the Bexsero vaccine as part of the immunisation schedule as well as MenQuadfi for high-risk groups.
Una Ren, Senior Scientist in Genomics, New Zealand Institute for Public Health and Forensic Science; Nigel French, Distinguished Professor of Infectious Disease Epidemiology and Public Health, Te Kunenga ki Pūrehuroa – Massey University, and Sarah Hannah, Doctoral Candidate in Epidemiology, Te Kunenga ki Pūrehuroa – Massey University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

‘Disease X’: What it is (and isn’t)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What you need to know
- In January 2024, the World Economic Forum hosted an event called Preparing for Disease X to discuss strategies to improve international pandemic response.
- Disease X is a term used in epidemiology to refer to potential disease threats. It is not a real disease or a global conspiracy.
- Preparation to prevent and respond to future pandemics is a necessary part of global health to keep us all safer.
During the World Economic Forum’s 54th annual meeting in Davos, Switzerland, global health experts discussed ways to strengthen health care systems in preparation for future pandemics. Conspiracy theories quickly began circulating posts about the event and the fictional disease at its center, so-called Disease X.
What is Disease X?
In 2018, the World Health Organization added Disease X to its list of Blueprint Priority Diseases that are public health risks. But, unlike the other diseases on the list, Disease X doesn’t exist. The term represents a hypothetical human disease capable of causing a pandemic. Although experts don’t know what the next Disease X will be, they can make educated guesses about where and how it may emerge—and how we can prepare for it.
Why are we hearing about Disease X now?
COVID-19 has been the deadliest infectious disease outbreak of the 21st century. It’s also an example of a Disease X: a previously unknown pathogen that spreads rapidly around the world, claiming millions of lives.
When the WEF hosted a panel of experts to discuss Disease X, it was the first exposure that many people had to a concept that global health experts have been discussing since 2018.
Even before the routine pandemic preparedness event took place, online conspiracy theorists began circulating false claims that those discussing and preparing for Disease X had sinister motives, underscoring how widespread distrust of global health entities has become in the wake of the COVID-19 pandemic.
Why does Disease X matter?
Epidemiologists use concepts like Disease X to plan for future outbreaks and avoid the mistakes of past outbreaks. The COVID-19 pandemic and the recent non-endemic outbreak of mpox highlight the importance of global coordination to efficiently prevent and respond to disease outbreaks.
Pandemics are inevitable, but the scale of their destruction doesn’t have to be. Major disease outbreaks are likely to become more frequent due to the impacts of climate change. Preparing for a pandemic now helps ensure that the world is better equipped to handle the next one.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: