Caffeine: Cognitive Enhancer Or Brain-Wrecker?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Two Sides Of Caffeine
We asked you for your health-related opinions on caffeine itself, not necessarily the coffee, tea, energy drinks, etc that might contain it.
We have, by the way previously written about the health effects of coffee and tea specifically:
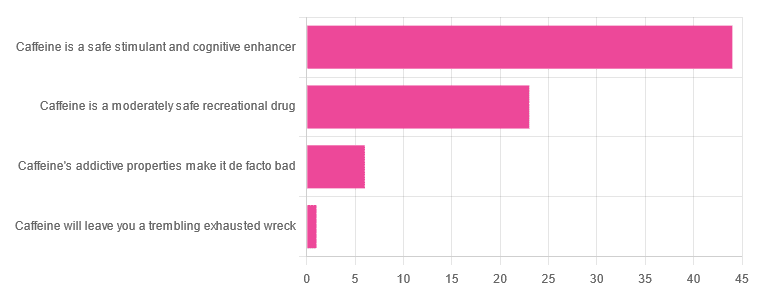
As for our question about caffeine itself, though, we got the above-depicted, below-described, set of results:
- About 59% said “caffeine is a safe stimulant and cognitive enhancer”
- About 31% said “caffeine is a moderately safe recreational drug”
- About 8% said “caffeine’s addictive properties make it de facto bad”
- One (1) person said “caffeine will leave you a trembling exhausted wreck”
But what does the science say?
Caffeine is addictive: True or False?
True, though one will find occasional academics quibbling the definition. Most of the studies into the mechanisms of caffeine addiction have been conducted on rats, but human studies exist too and caffeine is generally considered addictive for humans, for example:
See also:
Notwithstanding its addictive status, caffeine is otherwise safe: True or False?
True-ish, for most people. Some people with heart conditions or a hypersensitivity to caffeine may find it is not safe for them at all, and for the rest of us, the dose makes the poison. For example:
❝Can too much caffeine kill you? Although quite rare, caffeine can be fatal in cases of overdose; such circumstances are generally not applicable to healthy individuals who typically consume caffeine via beverages such as tea or coffee.❞
this paper, by the way, also includes a good example of academics quibbling the definition of addiction!
Caffeine is a cognitive enhancer: True or False?
True, but only in the case of occasional use. If you are using it all the time, your physiology will normalize it and you will require caffeine in order to function at your normal level. To attain higher than that, once addicted to caffeine, would now require something else.
Read more: Caffeine: benefits and drawbacks for technical performance
Caffeine will leave you a trembling exhausted wreck: True or False?
True or False depending on usage:
- The famously moderate 3–5 cups per day will not, for most people, cause any such problems.
- Using/abusing it to make up for lost sleep (or some other source of fatigue, such as physical exhaustion from exertion), however, is much more likely to run into problems.
In the latter case, caffeine really is the “payday loan” of energy! It’ll give you an adrenal boost now (in return, you must suffer the adrenal dumping later, along with lost energy expended in the adrenaline surge), and also, the tiredness that you thought was gone, was just caffeine’s adenosine-blocking activities temporarily preventing you from being able to perceive the tiredness. So you’ll have to pay that back later, with interest, because of the extra time/exertion too.
Want to make caffeine a little more gentle on your system?
Taking l-theanine alongside caffeine can ameliorate some of caffeine’s less wonderful effects—and as a bonus, l-theanine has some nifty benefits of its own, too:
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Are You Eating AGEs?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Trouble of the AGEs
Advanced Glycation End-Products (AGEs) are the result of the chemical process of glycation, which can occur in your body in response to certain foods you ate, or you can consume them directly, if you eat animal products that contained them (because we’re not special and other animals glycate too, especially mammals such as pigs, cows, and sheep).
As a double-whammy, if you cook animal products (especially without water, such as by roasting or frying), extra AGEs will form during cooking.
When proteinous and/or fatty food turns yellow/golden/brown during cooking, that’s generally glycation.
If there’s starch present, some or all of that yellow/golden/brown stuff will be a Maillard Reaction Product (MRP), such as acrylamide. That’s not exactly a health food, but it’s nowhere near being even in the same ballpark of badness.
In short, during cooking:
- Proteinous/fatty food turns yellow/golden/brown = probably an AGE
- Starchy food turns yellow/golden/brown = probably a MRP
The AGEs are far worse.
What’s so bad about AGEs?
Let’s do a quick tour of some studies:
- The role of advanced glycation end-products in retinal ageing and disease
- Advanced glycation end-products and their circulating receptors predict cardiovascular disease mortality in older women
- Elevated serum advanced glycation end-products in obese indicate risk for the metabolic syndrome: a link between healthy and unhealthy obesity?
- Increased levels of serum advanced glycation end-products in women with polycystic ovary syndrome
- Advanced glycation end-products and their involvement in liver disease
- Effects of advanced glycation end-products on renal fibrosis and oxidative stress
- Role of advanced glycation end-products and oxidative stress in vascular complications in diabetes
- Cancer malignancy is enhanced by advanced glycation end-products
- Advanced glycation end-products in the pathogenesis of Alzheimer’s disease
We could keep going, but you probably get the picture!
What should we do about it?
There are three main ways to reduce serum AGE levels:
Reduce or eliminate consumption of animal products
Especially mammalian animal products, such as from pigs, cows, and sheep, especially their meat. Processed versions are even worse! So, steak is bad, but bacon and sausages are literally top-tier bad.
Cook wet
Dry cooking (which includes frying, and especially includes deep fat frying, which is worse than shallow frying which is worse than air frying) produces far more AGEs than cooking with methods that involve water (boiling, steaming, slow-cooking, etc).
As a bonus, adding acidic ingredients (e.g. vinegar, lemon juice, tomato juice) can halve the amount of AGEs produced.
Consume antioxidants
Our body does have some ability to deal with AGEs, but that ability has its limits, and our body can be easily overwhelmed if we consume foods that are bad for it. So hopefully you’ll tend towards a plant-based diet, but whether you do or don’t:
You can give your body a hand by consuming antioxidant foods and drinks (such as berries, tea/coffee, and chocolate), and/or taking supplements.
Want to know more about the science of this?
Check out…
Advanced Glycation End-Products in Foods and a Practical Guide to Their Reduction in the Diet
Share This Post
-

Herbs For Evidence-Based Health & Healing
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Herbs have been used since prehistoric times to treat injuries and illnesses, but which ones actually work, as opposed to being “old wives’ tales”?
Even today, in pharmacies herbals products may come with a disclaimer “based on traditional use only”, which, in scientific terms, means it likely performs no better than placebo.
This is a “Saturday Life Hacks” edition, not a “Research Review Monday”, so we won’t be doing any deep-dives today, and will instead keep things short and snappy. We’ll also spotlight one main benefit, rather than trying to cover all bases, as we often have room to do on a Monday!
Basil
Helps boost immunity:
Chamomile
Significantly reduces symptoms of osteoarthritis:
(This one challenged your writer’s resolve as it does so many things, it was hard to pick just one. So, she went with one that’s less known that “settling the stomach” and “relieving PMS” and “relaxation” and so forth)
Echinacea
Significantly reduces the risk of catching a cold (but won’t help once you’ve caught it):
Echinacea for preventing and treating the common cold
Elderberry
Significantly hastens recovery from upper respiratory viral infections:
Evening Primrose
Fights neuropathy, along with many other benefits:
An updated review on pharmacological activities and phytochemical constituents of evening primrose
Fennel
Antinflammatory, along with many other benefits:
Ginkgo biloba
Antioxidant effects provide anti-aging benefits:
Advances in the Studies of Ginkgo Biloba Leaves Extract on Aging-Related Diseases
Ginseng
Combats fatigue:
Ginseng as a Treatment for Fatigue: A Systematic Review
Lavender
Enjoyed for its sedative effects, which is really does have:
Evidence for Sedative Effects of the Essential Oil of Lavender after Inhalation
Sage
Helps fight HIV type 1 and Herpes simplex type 2 (and probably other viruses, but that’s what we have the science for right now):
Aqueous extracts from peppermint, sage and lemon balm leaves display potent anti-HIV-1 activity
Valerian
Inconclusive data; “traditional use only” for restful sleep.
Can’t have everything!
Share This Post
-

Better With Age – by Dr. Alan Castel
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This one isn’t about the biology of aging, so much as (as the subtitle promises) the psychology of it.
Dr. Castel first covers the grounds of what “successful aging” is, and the benefits that can be expected from doing it right. Spoiler, it’s not just “reduced decline”, there are numerous things that actually get better, too.
We also learn how our memory works differently—it can be worse, of course, but it can also be just different, in a way that tends to tie in with vastness of the accumulated knowledge over the years, allowing for easiest access to the things the brain thinks are most important—ranging from expertise in a certain field, to life-experience “wisdom”.
There’s a lot of advice that’s mostly not going to be anything new to regular readers of 10almonds, in terms of staying sharp with an active lifestyle and a well-nourished brain.
The style is very soft pop-science; there are citations dotted throughout, but mostly this is more of a “curl up with a book” book, not a textbook.
In the category of subjective criticism, it can be a little repetitive (but for those who like repetition for ease of learning, you will love this), and his name-dropping habit gets quite eyeroll-worthy quite quickly.
Bottom line: if you’d like to learn about the very many ways in which “over the hill” is simply defeatist pessimism, then this book can help you to ensure you do better.
Click here to check out Better With Age, and get better with age!
Share This Post

Related Posts
-

What will aged care look like for the next generation? More of the same but higher out-of-pocket costs
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Aged care financing is a vexed problem for the Australian government. It is already underfunded for the quality the community expects, and costs will increase dramatically. There are also significant concerns about the complexity of the system.
In 2021–22 the federal government spent A$25 billion on aged services for around 1.2 million people aged 65 and over. Around 60% went to residential care (190,000 people) and one-third to home care (one million people).
The final report from the government’s Aged Care Taskforce, which has been reviewing funding options, estimates the number of people who will need services is likely to grow to more than two million over the next 20 years. Costs are therefore likely to more than double.
The taskforce has considered what aged care services are reasonable and necessary and made recommendations to the government about how they can be paid for. This includes getting aged care users to pay for more of their care.
But rather than recommending an alternative financing arrangement that will safeguard Australians’ aged care services into the future, the taskforce largely recommends tidying up existing arrangements and keeping the status quo.
No Medicare-style levy
The taskforce rejected the aged care royal commission’s recommendation to introduce a levy to meet aged care cost increases. A 1% levy, similar to the Medicare levy, could have raised around $8 billion a year.
The taskforce failed to consider the mix of taxation, personal contributions and social insurance which are commonly used to fund aged care systems internationally. The Japanese system, for example, is financed by long-term insurance paid by those aged 40 and over, plus general taxation and a small copayment.
Instead, the taskforce puts forward a simple, pragmatic argument that older people are becoming wealthier through superannuation, there is a cost of living crisis for younger people and therefore older people should be required to pay more of their aged care costs.
Separating care from other services
In deciding what older people should pay more for, the taskforce divided services into care, everyday living and accommodation.
The taskforce thought the most important services were clinical services (including nursing and allied health) and these should be the main responsibility of government funding. Personal care, including showering and dressing were seen as a middle tier that is likely to attract some co-payment, despite these services often being necessary to maintain independence.
The task force recommended the costs for everyday living (such as food and utilities) and accommodation expenses (such as rent) should increasingly be a personal responsibility.

Aged care users will pay more of their share for cooking and cleaning.
Lizelle Lotter/ShutterstockMaking the system fairer
The taskforce thought it was unfair people in residential care were making substantial contributions for their everyday living expenses (about 25%) and those receiving home care weren’t (about 5%). This is, in part, because home care has always had a muddled set of rules about user co-payments.
But the taskforce provided no analysis of accommodation costs (such as utilities and maintenance) people meet at home compared with residential care.
To address the inefficiencies of upfront daily fees for packages, the taskforce recommends means testing co-payments for home care packages and basing them on the actual level of service users receive for everyday support (for food, cleaning, and so on) and to a lesser extent for support to maintain independence.
It is unclear whether clinical and personal care costs and user contributions will be treated the same for residential and home care.
Making residential aged care sustainable
The taskforce was concerned residential care operators were losing $4 per resident day on “hotel” (accommodation services) and everyday living costs.
The taskforce recommends means tested user contributions for room services and everyday living costs be increased.
It also recommends that wealthier older people be given more choice by allowing them to pay more (per resident day) for better amenities. This would allow providers to fully meet the cost of these services.
Effectively, this means daily living charges for residents are too low and inflexible and that fees would go up, although the taskforce was clear that low-income residents should be protected.
Moving from buying to renting rooms
Currently older people who need residential care have a choice of making a refundable up-front payment for their room or to pay rent to offset the loans providers take out to build facilities. Providers raise capital to build aged care facilities through equity or loan financing.
However, the taskforce did not consider the overall efficiency of the private capital market for financing aged care or alternative solutions.
Instead, it recommended capital contributions be streamlined and simplified by phasing out up-front payments and focusing on rental contributions. This echoes the royal commission, which found rent to be a more efficient and less risky method of financing capital for aged care in private capital markets.
It’s likely that in a decade or so, once the new home care arrangements are in place, there will be proportionally fewer older people in residential aged care. Those who do go are likely to be more disabled and have greater care needs. And those with more money will pay more for their accommodation and everyday living arrangements. But they may have more choice too.
Although the federal government has ruled out an aged care levy and changes to assets test on the family home, it has yet to respond to the majority of the recommendations. But given the aged care minister chaired the taskforce, it’s likely to provide a good indication of current thinking.

Hal Swerissen, Emeritus Professor, La Trobe University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Could ADHD drugs reduce the risk of early death? Unpacking the findings from a new Swedish study
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Attention-deficit hyperactivity disorder (ADHD) can have a considerable impact on the day-to-day functioning and overall wellbeing of people affected. It causes a variety of symptoms including difficulty focusing, impulsivity and hyperactivity.
For many, a diagnosis of ADHD, whether in childhood or adulthood, is life changing. It means finally having an explanation for these challenges, and opens up the opportunity for treatment, including medication.
Although ADHD medications can cause side effects, they generally improve symptoms for people with the disorder, and thereby can significantly boost quality of life.
Now a new study has found being treated for ADHD with medication reduces the risk of early death for people with the disorder. But what can we make of these findings?
A large study from Sweden
The study, published this week in JAMA (the prestigious journal of the American Medical Association), was a large cohort study of 148,578 people diagnosed with ADHD in Sweden. It included both adults and children.
In a cohort study, a group of people who share a common characteristic (in this case a diagnosis of ADHD) are followed over time to see how many develop a particular health outcome of interest (in this case the outcome was death).
For this study the researchers calculated the mortality rate over a two-year follow up period for those whose ADHD was treated with medication (a group of around 84,000 people) alongside those whose ADHD was not treated with medication (around 64,000 people). The team then determined if there were any differences between the two groups.
What did the results show?
The study found people who were diagnosed and treated for ADHD had a 19% reduced risk of death from any cause over the two years they were tracked, compared with those who were diagnosed but not treated.
In understanding this result, it’s important – and interesting – to look at the causes of death. The authors separately analysed deaths due to natural causes (physical medical conditions) and deaths due to unnatural causes (for example, unintentional injuries, suicide, or accidental poisonings).
The key result is that while no significant difference was seen between the two groups when examining natural causes of death, the authors found a significant difference for deaths due to unnatural causes.
So what’s going on?
Previous studies have suggested ADHD is associated with an increased risk of premature death from unnatural causes, such as injury and poisoning.
On a related note, earlier studies have also suggested taking ADHD medicines may reduce premature deaths. So while this is not the first study to suggest this association, the authors note previous studies addressing this link have generated mixed results and have had significant limitations.
In this new study, the authors suggest the reduction in deaths from unnatural causes could be because taking medication alleviates some of the ADHD symptoms responsible for poor outcomes – for example, improving impulse control and decision-making. They note this could reduce fatal accidents.
The authors cite a number of studies that support this hypothesis, including research showing ADHD medications may prevent the onset of mood, anxiety and substance use disorders, and lower the risk of accidents and criminality. All this could reasonably be expected to lower the rate of unnatural deaths.
Strengths and limitations
Scandinavian countries have well-maintained national registries that collect information on various aspects of citizens’ lives, including their health. This allows researchers to conduct excellent population-based studies.
Along with its robust study design and high-quality data, another strength of this study is its size. The large number of participants – almost 150,000 – gives us confidence the findings were not due to chance.
The fact this study examined both children and adults is another strength. Previous research relating to ADHD has often focused primarily on children.
One of the important limitations of this study acknowledged by the authors is that it was observational. Observational studies are where the researchers observe and analyse naturally occurring phenomena without intervening in the lives of the study participants (unlike randomised controlled trials).
The limitation in all observational research is the issue of confounding. This means we cannot be completely sure the differences between the two groups observed were not either partially or entirely due to some other factor apart from taking medication.
Specifically, it’s possible lifestyle factors or other ADHD treatments such as psychological counselling or social support may have influenced the mortality rates in the groups studied.
Another possible limitation is the relatively short follow-up period. What the results would show if participants were followed up for longer is an interesting question, and could be addressed in future research.
What are the implications?
Despite some limitations, this study adds to the evidence that diagnosis and treatment for ADHD can make a profound difference to people’s lives. As well as alleviating symptoms of the disorder, this study supports the idea ADHD medication reduces the risk of premature death.
Ultimately, this highlights the importance of diagnosing ADHD early so the appropriate treatment can be given. It also contributes to the body of evidence indicating the need to improve access to mental health care and support more broadly.
Hassan Vally, Associate Professor, Epidemiology, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

‘Sleep tourism’ promises the trip of your dreams. Beyond the hype plus 5 tips for a holiday at home
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Imagine arriving at your hotel after a long flight and being greeted by your own personal sleep butler. They present you with a pillow menu and invite you to a sleep meditation session later that day.
You unpack in a room kitted with an AI-powered smart bed, blackout shades, blue light-blocking glasses and weighted blankets.
Holidays are traditionally for activities or sightseeing – eating Parisian pastry under the Eiffel tower, ice skating at New York City’s Rockefeller Centre, lying by the pool in Bali or sipping limoncello in Sicily. But “sleep tourism” offers vacations for the sole purpose of getting good sleep.
The emerging trend extends out of the global wellness tourism industry – reportedly worth more than US$800 billion globally (A$1.2 trillion) and expected to boom.
Luxurious sleep retreats and sleep suites at hotels are popping up all over the world for tourists to get some much-needed rest, relaxation and recovery. But do you really need to leave home for some shuteye?
RossHelen/Shutterstock Not getting enough
The rise of sleep tourism may be a sign of just how chronically sleep deprived we all are.
In Australia more than one-third of adults are not achieving the recommended 7–9 hours of sleep per night, and the estimated cost of this inadequate sleep is A$45 billion each year.
Inadequate sleep is linked to long-term health problems including poor mental health, heart disease, metabolic disease and deaths from any cause.
Can a fancy hotel give you a better sleep?
Many of the sleep services available in the sleep tourism industry aim to optimise the bedroom for sleep. This is a core component of sleep hygiene – a series of healthy sleep practices that facilitate good sleep including sleeping in a comfortable bedroom with a good mattress and pillow, sleeping in a quiet environment and relaxing before bed.
The more people follow sleep hygiene practices, the better their sleep quality and quantity.
When we are staying in a hotel we are also likely away from any stressors we encounter in everyday life (such as work pressure or caring responsibilities). And we’re away from potential nighttime disruptions to sleep we might experience at home (the construction work next door, restless pets, unsettled children). So regardless of the sleep features hotels offer, it is likely we will experience improved sleep when we are away.
Being away from home also means being away from domestic disruptions. Makistock/Shutterstock What the science says about catching up on sleep
In the short-term, we can catch up on sleep. This can happen, for example, after a short night of sleep when our brain accumulates “sleep pressure”. This term describes how strong the biological drive for sleep is. More sleep pressure makes it easier to sleep the next night and to sleep for longer.
But while a longer sleep the next night can relieve the sleep pressure, it does not reverse the effects of the short sleep on our brain and body. Every night’s sleep is important for our body to recover and for our brain to process the events of that day. Spending a holiday “catching up” on sleep could help you feel more rested, but it is not a substitute for prioritising regular healthy sleep at home.
All good things, including holidays, must come to an end. Unfortunately the perks of sleep tourism may end too.
Our bodies do not like variability in the time of day that we sleep. The most common example of this is called “social jet lag”, where weekday sleep (getting up early to get to work or school) is vastly different to weekend sleep (late nights and sleep ins). This can result in a sleepy, grouchy start to the week on Monday. Sleep tourism may be similar, if you do not come back home with the intention to prioritise sleep.
So we should be mindful that as well as sleeping well on holiday, it is important to optimise conditions at home to get consistent, adequate sleep every night.
Good sleep hygiene doesn’t require a passport. Maridav/Shutterstock 5 tips for having a sleep holiday at home
An AI-powered mattress and a sleep butler at home might be the dream. But these features are not the only way we can optimise our sleep environment and give ourselves the best chance to get a good night’s sleep. Here are five ideas to start the night right:
1. avoid bright artificial light in the evening (such as bright overhead lights, phones, laptops)
2. make your bed as comfortable as possible with fresh pillows and a supportive mattress
3. use black-out window coverings and maintain a cool room temperature for the ideal sleeping environment
4. establish an evening wind-down routine, such as a warm shower and reading a book before bed or even a “sleepy girl mocktail”
5. use consistency as the key to a good sleep routine. Aim for a similar bedtime and wake time – even on weekends.
Charlotte Gupta, Senior postdoctoral research fellow, Appleton Institute, HealthWise research group, CQUniversity Australia and Dean J. Miller, Adjunct Research Fellow, Appleton Institute of Behavioural Science, CQUniversity Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: