ADHD… As An Adult?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
ADHD—not just for kids!
Consider the following:
- If a kid has consistent problems paying attention, it’s easy and common to say “Aha, ADHD!”
- If a young adult has consistent problems paying attention, it’s easy and common to say “Aha, a disinterested ne’er-do-well!”
- If an older adult has consistent problems paying attention, it’s easy and common to say “Aha, a senior moment!”
Yet, if we recognize that ADHD is fundamentally a brain difference in children (and we do; there are physiological characteristics that we can test), and we can recognize that as people get older our brains typically have less neuroplasticity (ability to change) than when we are younger rather than less, then… Surely, there are just as many adults with ADHD as kids!
After all, that rather goes with the linear nature of time and the progressive nature of getting older.
So why do kids get diagnoses so much more often than adults?
Parents—and schools—can find children’s ADHD challenging, and it’s their problem, so they look for an explanation, and ADHD isn’t too difficult to find as a diagnosis.
Meanwhile, adults with ADHD have usually developed coping mechanisms, have learned to mask and/or compensate for their symptoms, and we expect adults to manage their own problems, so nobody’s rushing to find an explanation on their behalf.
Additionally, the stigma of neurodivergence—especially something popularly associated with children—isn’t something that many adults will want for themselves.
But, if you have an ADHD brain, then recognizing that (even if just privately to yourself) can open the door to much better management of your symptoms… and your life.
So what does ADHD look like in adults?
ADHD involves a spread of symptoms, and not everyone will have them all, or have them in the same magnitude. However, very commonly most noticeable traits include:
- Lack of focus (ease of distraction)
- Conversely: high focus (on the wrong things)
- To illustrate: someone with ADHD might set out to quickly tidy the sock drawer, and end up Marie Kondo-ing their entire wardrobe… when they were supposed to doing something else
- Conversely: high focus (on the wrong things)
- Poor time management (especially: tendency to procrastinate)
- Forgetfulness (of various kinds—for example, forgetting information, and forgetting to do things)
Want To Take A Quick Test? Click Here ← this one is reputable, and free. No sign in required; the test is right there.
Wait, where’s the hyperactivity in this Attention Deficit Hyperactivity Disorder?
It’s often not there. ADHD is simply badly-named. This stems from how a lot of mental health issues are considered by society in terms of how much they affect (and are observable by) other people. Since ADHD was originally noticed in children (in fact being originally called “Hyperkinetic Reaction of Childhood”), it ended up being something like:
“Oh, your brain has an inconvenient relationship with dopamine and you are driven to try to correct that by shifting attention from boring things to stimulating things? You might have trouble-sitting-still disorder”
Hmm, this sounds like me (or my loved one); what to do now at the age of __?
Some things to consider:
- If you don’t want medication (there are pros and cons, beyond the scope of today’s article), you might consider an official diagnosis not worth pursuing. That’s fine if so, because…
- More important than whether or not you meet certain diagnostic criteria, is whether or not the strategies recommended for it might help you.
- Whether or not you talk to other people about it is entirely up to you. Maybe it’s a stigma you’d rather avoid… Or maybe it’ll help those around you to better understand and support you.
- Either way, you might want to learn more about ADHD in adults. Today’s article was about recognizing it—we’ll write more about managing it another time!
In the meantime… We recommended a great book about this a couple of weeks ago; you might want to check it out:
Click here to see our review of “The Silent Struggle: Taking Charge of ADHD in Adults”!
Note: the review is at the bottom of that page. You’ll need to scroll past the video (which is also about ADHD) without getting distracted by it and forgetting you were there to see about the book. So:
- Click the above link
- Scroll straight to the review!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Couple’s Guide to Thriving with ADHD – by Melissa Orlov and Nancie Kohlenberger

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
ADHD (what a misleadingly-named condition) is most often undiagnosed in adults, especially older adults, and has far-reaching effects. This book explores those!
Oftentimes ADHD is not a deficit of attention, it’s just a lack of choice about where one’s attention goes. And the H? It’s mostly not what people think it is. The diagnostic criteria have moved far beyond the original name.
But in a marriage, ADHD symptoms such as wandering attention, forgetfulness, impulsiveness, and a focus on the “now” to the point of losing sight of the big picture (the forgotten past and the unplanned future), can cause conflict.
The authors write in a way that is intended for the ADHD and/or non-ADHD partner to read, and ideally, for both to read.
They shine light on why people with or without ADHD tend towards (or away from) certain behaviours, what miscommunications can arise, and how to smooth them over.
Best of all, an integrated plan for getting you both on the same page, so that you can tackle anything that arises, as the diverse team (with quite different individual strengths) that you are.
Bottom line: if you or a loved one has ADHD symptoms, this book can help you navigate and untangle what can otherwise sometimes get a little messy.
Click here to check out The Couple’s Guide to Thriving with ADHD, and learn how to do just that!
Share This Post
-

Is It Possible To Lose Weight Quickly?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In Victorian England, weight-loss trends like the dangerous tapeworm diet were popular. While modern fad diets can seem less extreme, they often promise similarly fast results. However, these quick fixes can have similarly harmful consequences:
Not so fast
To illustrate the difference between gradual and extreme dieting, the video bids us consider two identical twins, Sam and Felix:
- Sam adopts a gradual approach, slowly reducing calorie intake and exercising regularly. This causes his body to burn glycogen stores before transitioning to fat as an energy source. Regular exercise helps Sam maintain muscle mass, which boosts his metabolism and supports sustained weight loss.
- Felix drastically cuts calories, forcing his body into starvation mode. He quickly depletes glycogen stores, loses muscle mass, and burns fewer calories, making long-term weight loss more difficult. Although Felix might initially lose water weight, this is temporary and unsustainable.
You cannot “just lose it quickly now, and then worry about healthiness once the weight’s gone”, because you will lose health much more quickly than you will lose fat, and that will sabotage, rather than help, your fat loss journey.Healthy weight loss requires gradual, balanced changes in diet and exercise tailored to individual needs. Extreme diets, whether through calorie restriction or things like elimination of carbs or fats, are unsustainable and shock the body. It’s important to prioritize long-term health over societal pressures for quick weight loss and focus on developing a sustainable, healthy lifestyle.
In short, the quickest way to lose weight and keep it off (without dying), is to lose it slowly.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
How To Lose Weight (Healthily)
Take care!
Share This Post
-

Best Salt for Neti Pots?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
❓ Q&A With 10almonds Subscribers!
Q: What kind of salt is best for neti pots?
A: Non-iodised salt is usually recommended, but really, any human-safe salt is fine. By this we mean for example:
- Sodium chloride (like most kitchen salts),
- Potassium chloride (as found in “reduced sodium” kitchen salts), or
- Magnesium sulfate (also known as epsom salts).
Share This Post


-

Farmed Fish vs Wild Caught
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝Is it good to eat farm raised fish?❞
We’ll answer this as a purely health-related question (and thus not considering economy, ecology, ethics, or taste).
It’s certainly not as good as wild-caught fish, for several reasons, some more serious than others:
Farmed fish can have quite a different nutritional profile to wild-caught fish, and also contain more contaminants, including heavy metals.
For example, farmed fish tend to have much higher fat content for the same amount of protein, but lower levels of minerals and other nutrients. Here are two side-by-side:
Wild-caught salmon | Farmed salmon
See also:
Quantitative analysis of the benefits and risks of consuming farmed and wild salmon
Additionally, because fish in fish farms tend to be very susceptible to diseases (because of the artificially cramped and overcrowded environment), fish farms tend to make heavy use of antibiotics, which can cause all sorts of problems down the line:
So definitely, “let the buyer beware”!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why ’10almonds’? Newsletter Name Explained
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day!
Each Thursday, we respond to subscriber questions and requests! If it’s something small, we’ll answer it directly; if it’s something bigger, we’ll do a main feature in a follow-up day instead!
So, no question/request to big or small; they’ll just get sorted accordingly
Remember, you can always hit reply to any of our emails, or use the handy feedback widget at the bottom. We always look forward to hearing from you!
Q: Why is your newsletter called 10almonds? Maybe I missed it in the intro email, but my curiosity wants to know the significance. Thanks!”
It’s a reference to a viral Facebook hoax! There was a post going around that claimed:
❝HEADACHE REMEDY. Eat 10–12 almonds, the equivalent of two aspirins, next time you have a headache❞ ← not true!
It made us think about how much health-related disinformation there was online… So, calling ourselves 10almonds was a bit of a tongue-in-cheek reference to that story… but also a reminder to ourselves:
We must always publish information with good scientific evidence behind it!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Natto vs Tofu – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
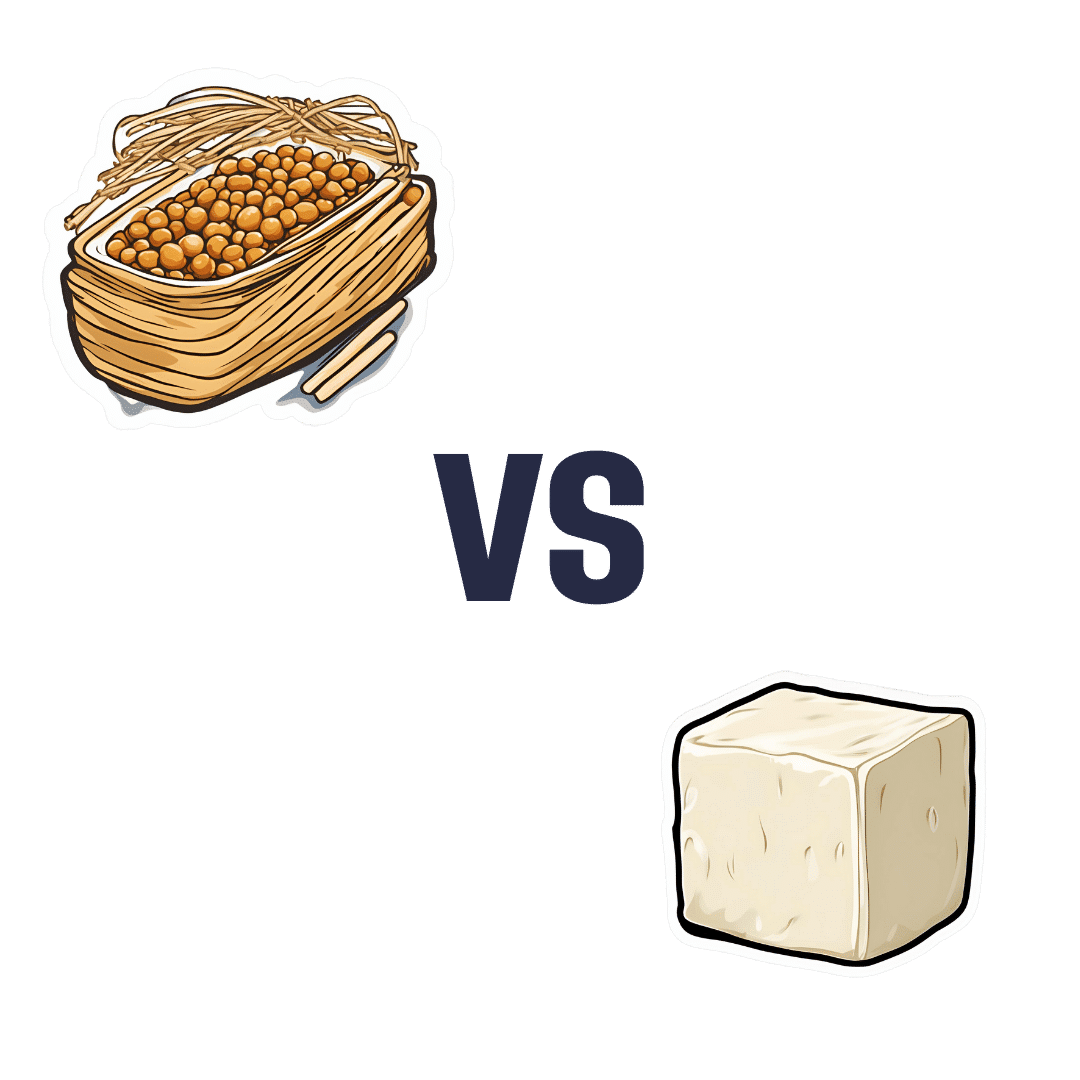
When comparing nattō to tofu, we picked the nattō.
Why?
In other words, in the comparison of fermented soy to fermented soy, we picked the fermented soy. But the relevant difference here is that nattō is fermented whole soybeans, while tofu is fermented soy milk of which the coagulated curds are then compressed into a block—meaning that the nattō is the one that has “more food per food”.
Looking at the macros, it’s therefore no surprise that nattō has a lot more fiber to go with its higher carb count; it also has slightly more protein. You may be wondering what tofu has more of, and the answer is: water.
In terms of vitamins, nattō has more of vitamins B2, B4, B6, C, E, K, and choline, while tofu has more of vitamins A, B3, and B9. So, a 7:3 win for nattō, even before considering that that vitamin C content of nattō is 65x more than what tofu has.
When it comes to minerals, nattō has more copper, iron, magnesium, manganese, potassium, and zinc, while tofu has more calcium, phosphorus, and selenium. So, a 6:3 win for nattō, and yes, the margins of difference are comparable (being 2–3x more for most of these minerals).
In short, both of these foods are great, but nattō is better.
Want to learn more?
You might like to read:
21% Stronger Bones in a Year at 62? Yes, It’s Possible (No Calcium Supplements Needed!)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: