Can Saturated Fats Be Healthy?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Saturated Fat: What’s The Truth?
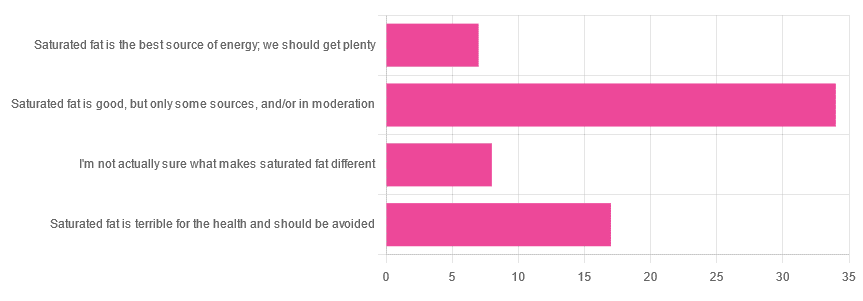
We asked you for your health-related opinion of saturated fat, and got the above-pictured, below-described, set of results.
- Most recorded votes were for “Saturated fat is good, but only some sources, and/or in moderation”
- This is an easy one to vote for, because of the “and/or in moderation” part, which tends to be a “safe bet” for most things.
- Next most popular was “Saturated fat is terrible for the health and should be avoided”
- About half as many recorded votes were for “I’m not actually sure what makes saturated fat different”, which is a very laudable option to click. Admitting when we don’t know things (and none of us know everything) is a very good first step to learning about them!
- Fewest recorded votes were for “Saturated fat is the best source of energy; we should get plenty”.
So, what does the science say?
First, a bit of physics, chemistry, and biology
You may be wondering what, exactly, saturated fats are “saturated” with. That’s a fair question, so…
All fats have a molecular structure made up of carbon, hydrogen, and oxygen atoms. Saturated fats are saturated with hydrogen, and thus have only single bonds between carbon atoms (unsaturated fats have at least one double-bond between carbon atoms).
The observable effect this has on them, is that fats that are saturated with hydrogen are solid at room temperature, whereas unsaturated fats are liquid at room temperature. Their different properties also make for different interactions inside the human body, including how likely or not they are to (for example) clog arteries.
See also: Could fat in your bloodstream cause blood clots?
Saturated fat is the best source of energy; we should get plenty: True or False?
False, in any reasonable interpretation, anyway. That is to say, if your idea of “plenty” is under 13g (e.g: two tablespoons of butter, and no saturated fat from other sources, e.g. meat) per day, then yes, by all means feel free to eat plenty. More than that, though, and you might want to consider trimming it down a bit.
The American Heart Association has this to say:
❝When you hear about the latest “diet of the day” or a new or odd-sounding theory about food, consider the source.
The American Heart Association recommends limiting saturated fats, which are found in butter, cheese, red meat and other animal-based foods, and tropical oils.
Decades of sound science has proven it can raise your “bad” cholesterol and put you at higher risk for heart disease.❞
Source: The American Heart Association Diet and Lifestyle Recommendations on Saturated Fat
The British Heart Foundation has a similar statement:
❝Despite what you read in the media, our advice is clear: replace saturated fats with unsaturated fats and avoid trans fats. Saturated fat is the kind of fat found in butter, lard, ghee, fatty meats and cheese. This is linked to an increased risk of heart and circulatory disease❞
Source: British Heart Foundation: What does fat do and what is saturated fat?
As for the World Health Organization:
❝1. WHO strongly recommends that adults and children reduce saturated fatty acid intake to 10% of total energy intake
2. WHO suggests further reducing saturated fatty acid intake to less than 10% of total energy intake
3. WHO strongly recommends replacing saturated fatty acids in the diet with polyunsaturated fatty acids; monounsaturated fatty acids from plant sources; or carbohydrates from foods containing naturally occurring dietary fibre, such as whole grains, vegetables, fruits and pulses.❞
Source: Saturated fatty acid and trans-fatty acid intake for adults and children: WHO guideline
Please note, organizations such as the AHA, the BHF, and the WHO are not trying to sell us anything, and just would like us to not die of heart disease, the world’s #1 killer.
As for “the best source of energy”…
We evolved to eat (much like our nearest primate cousins) a diet consisting mostly of fruits and other edible plants, with a small supplementary amount of animal-source protein and fats.
That’s not to say that because we evolved that way we have to eat that way—we are versatile omnivores. But for example, we are certainly not complete carnivores, and would quickly sicken and die if we tried to live on only meat and animal fat (we need more fiber, more carbohydrates, and many micronutrients that we usually get from plants)
The closest that humans tend to come to doing such is the ketogenic diet, which focuses on a high fat, low carbohydrate imbalance, to promote ketosis, in which the body burns fat for energy.
The ketogenic diet does work, and/but can cause a lot of health problems if a lot of care is not taken to avoid them.
See for example: 7 Keto Risks To Keep In Mind
Saturated fat is terrible for the health and should be avoided: True or False?
False, if we are talking about “completely”.
Firstly, it’s practically impossible to cut out all saturated fats, given that most dietary sources of fat are a mix of saturated, unsaturated (mono- and poly-), and trans fats (which are by far the worst, but beyond the scope of today’s main feature).
Secondly, a lot of research has been conducted and found insignificant or inconclusive results, in cases where saturated fat intake was already within acceptable levels (per the recommendations we mentioned earlier), and then cut down further.
Rather than fill up the newsletter with individual studies of this kind here’s a high-quality research review, looking at 19 meta-analyses, each of those meta-analyses having looked at many studies:
Dietary saturated fat and heart disease: a narrative review
Saturated fat is good, but only some sources, and/or in moderation: True or False?
True! The moderation part is easy to guess, so let’s take a look at the “but only some sources”.
We were not able to find any convincing science to argue for health-based reasons to favor plant- or animal-sourced saturated fat. However…
Not all saturated fats are created equal (there are many kinds), and also many of the foods containing them have additional nutrients, or harmful compounds, that make a big difference to overall health, when compared gram-for-gram in terms of containing the same amount of saturated fat.
For example:
- Palm oil’s saturated fat contains a disproportionate amount of palmitic acid, which raises LDL (“bad” cholesterol) without affecting HDL (“good” cholesterol), thus having an overall heart-harmful effect.
- Most animal fats contain a disproportionate amount of stearic acid, which has statistically insignificant effects on LDL and HDL levels, and thus is broadly considered “heart neutral” (in moderation!)
- Coconut oil’s saturated fat contains a disproportionate amount of lauric acid, which raises total cholesterol, but mostly HDL without affecting LDL, thus having an overall heart-beneficial effect (in moderation!)
Do you know what’s in the food you eat?
Test your knowledge with the BHF’s saturated fat quiz!
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

From banning junk food ads to a sugar tax: with diabetes on the rise, we can’t afford to ignore the evidence any longer

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There are renewed calls this week for the Australian government to implement a range of measures aimed at improving our diets. These include restrictions on junk food advertising, improvements to food labelling, and a levy on sugary drinks.
This time the recommendations come from a parliamentary inquiry into diabetes in Australia. Its final report, tabled in parliament on Wednesday, was prepared by a parliamentary committee comprising members from across the political spectrum.
The release of this report could be an indication that Australia is finally going to implement the evidence-based healthy eating policies public health experts have been recommending for years.
But we know Australian governments have historically been unwilling to introduce policies the powerful food industry opposes. The question is whether the current government will put the health of Australians above the profits of companies selling unhealthy food.

benjamas11/Shutterstock Diabetes in Australia
Diabetes is one of the fastest growing chronic health conditions in the nation, with more than 1.3 million people affected. Projections show the number of Australians diagnosed with the condition is set to rise rapidly in coming decades.
Type 2 diabetes accounts for the vast majority of cases of diabetes. It’s largely preventable, with obesity among the strongest risk factors.
This latest report makes it clear we need an urgent focus on obesity prevention to reduce the burden of diabetes. Type 2 diabetes and obesity cost the Australian economy billions of dollars each year and preventive solutions are highly cost-effective.
This means the money spent on preventing obesity and diabetes would save the government huge amounts in health care costs. Prevention is also essential to avoid our health systems being overwhelmed in the future.
What does the report recommend?
The report puts forward 23 recommendations for addressing diabetes and obesity. These include:
- restrictions on the marketing of unhealthy foods to children, including on TV and online
- improvements to food labelling that would make it easier for people to understand products’ added sugar content
- a levy on sugary drinks, where products with higher sugar content would be taxed at a higher rate (commonly called a sugar tax).
These key recommendations echo those prioritised in a range of reports on obesity prevention over the past decade. There’s compelling evidence they’re likely to work.
Restrictions on unhealthy food marketing
There was universal support from the committee for the government to consider regulating marketing of unhealthy food to children.
Public health groups have consistently called for comprehensive mandatory legislation to protect children from exposure to marketing of unhealthy foods and related brands.
An increasing number of countries, including Chile and the United Kingdom, have legislated unhealthy food marketing restrictions across a range of settings including on TV, online and in supermarkets. There’s evidence comprehensive policies like these are having positive results.
In Australia, the food industry has made voluntary commitments to reduce some unhealthy food ads directly targeting children. But these promises are widely viewed as ineffective.
The government is currently conducting a feasibility study on additional options to limit unhealthy food marketing to children.
But the effectiveness of any new policies will depend on how comprehensive they are. Food companies are likely to rapidly shift their marketing techniques to maximise their impact. If any new government restrictions do not include all marketing channels (such as TV, online and on packaging) and techniques (including both product and brand marketing), they’re likely to fail to adequately protect children.
Food labelling
Food regulatory authorities are currently considering a range of improvements to food labelling in Australia.
For example, food ministers in Australia and New Zealand are soon set to consider mandating the health star rating front-of-pack labelling scheme.
Public health groups have consistently recommended mandatory implementation of health star ratings as a priority for improving Australian diets. Such changes are likely to result in meaningful improvements to the healthiness of what we eat.
Regulators are also reviewing potential changes to how added sugar is labelled on product packages. The recommendation from the committee to include added sugar labelling on the front of product packaging is likely to support this ongoing work.
But changes to food labelling laws are notoriously slow in Australia. And food companies are known to oppose and delay any policy changes that might hurt their profits.
Health star ratings are not compulsory in Australia. BLACKDAY/Shutterstock A sugary drinks tax
Of the report’s 23 recommendations, the sugary drinks levy was the only one that wasn’t universally supported by the committee. The four Liberal and National party members of the committee opposed implementation of this policy.
As part of their rationale, the dissenting members cited submissions from food industry groups that argued against the measure. This follows a long history of the Liberal party siding with the sugary drinks industry to oppose a levy on their products.
The dissenting members didn’t acknowledge the strong evidence that a sugary drinks levy has worked as intended in a wide range of countries.
In the UK, for example, a levy on sugary drinks implemented in 2018 has successfully lowered the sugar content in UK soft drinks and reduced sugar consumption.
The dissenting committee members argued a sugary drinks levy would hurt families on lower incomes. But previous Australian modelling has shown the two most disadvantaged quintiles would reap the greatest health benefits from such a levy, and accrue the highest savings in health-care costs.
What happens now?
Improvements to population diets and prevention of obesity will require a comprehensive and coordinated package of policy reforms.
Globally, a range of countries facing rising epidemics of obesity and diabetes are starting to take such strong preventive action.
In Australia, after years of inaction, this week’s report is the latest sign that long-awaited policy change may be near.
But meaningful and effective policy change will require politicians to listen to the public health evidence rather than the protestations of food companies concerned about their bottom line.
Gary Sacks, Professor of Public Health Policy, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Decoding Hormone Balancing in Ads
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Time!
This is the bit whereby each week, we respond to subscriber questions/requests/etc
Have something you’d like to ask us, or ask us to look into? Hit reply to any of our emails, or use the feedback widget at the bottom, and a Real Human™ will be glad to read it!
Q: As to specific health topics, I would love to see someone address all these Instagram ads targeted to women that claim “You only need to ‘balance your hormones’ to lose weight, get ripped, etc.” What does this mean? Which hormones are they all talking about? They all seem to be selling a workout program and/or supplements or something similar, as they are ads, after all. Is there any science behind this stuff or is it mostly hot air, as I suspect?
Thank you for asking this, as your question prompted yesterday’s main feature, What Does “Balancing Your Hormones” Even Mean?
That’s a great suggestion also about addressing ads (and goes for health-related things in general, not just hormonal stuff) and examining their claims, what they mean, how they work (if they work!), and what’s “technically true but may
be misleading* cause confusion”*We don’t want companies to sue us, of course.
Only, we’re going to need your help for this one, subscribers!
See, here at 10almonds we practice what we preach. We limit screen time, we focus on our work when working, and simply put, we don’t see as many ads as our thousands of subscribers do. Also, ads tend to be targeted to the individual, and often vary from country to country, so chances are good that we’re not seeing the same ads that you’re seeing.
So, how about we pull together as a bit of a 10almonds community project?
- Step 1: add our email address to your contacts list, if you haven’t already
- Step 2: When you see an ad you’re curious about, select “share” (there is usually an option to share ads, but if not, feel free to screenshot or such)
- Step 3: Send the ad to us by email
We’ll do the rest! Whenever we have enough ads to review, we’ll do a special on the topic.
We will categorically not be able to do this without you, so please do join in—Many thanks in advance!
Share This Post
-

The Sweet Truth About Glycine
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Make Your Collagen Work Better

This is Dr. James Nicolantonio. He’s a doctor of pharmacy, and a research scientist. He has a passion for evidence-based nutrition, and has written numerous books on the subject.
Controversy! Dr. DiNicolatonio’s work has included cardiovascular research, in which field he has made the case for increasing (rather than decreasing) the recommended amount of salt in our diet. This, of course, goes very much against the popular status quo.
We haven’t reviewed that research so we won’t comment on it here, but we thought it worth a mention as a point of interest. We’ll investigate his claims in that regard another time, though!
Today, however, we’ll be looking at his incisive, yet not controversial, work pertaining to collagen and glycine.
A quick recap on collagen
We’ve written about collagen before, and its importance for maintaining… Well, pretty much most of our body, really, buta deficiency in collagen can particularly weaken bones and joints.
On a more surface level, collagen’s also important for healthy elastic skin, and many people take it for that reason alone,
Since collagen is found only in animals, even collagen supplements are animal-based (often marine collagen or bovine collagen). However, if we don’t want to consume those, we can (like most animals) synthesize it ourselves from the relevant amino acids, which we can get from plants (and also laboratories, in some cases).
You can read our previous article about this, here:
We Are Such Stuff As Fish Are Made Of
What does he want us to know about collagen?
We’ll save time and space here: first, he’d like us to know the same as what we said in our article above
However, there is also more:
Let’s assume that your body has collagen to process. You either consumed it, or your body has synthesized it. We’ll skip describing the many steps of collagen synthesis, fascinating as that is, and get to the point:
When our body weaves together collagen fibrils out of the (triple-helical) collagen molecules…
- the cross-linking of the collagen requires lysyl oxidase
- the lysyl oxidase (which we make inside us) deanimates some other amino acids yielding aldehydes that allow the stable cross-links important for the high tensile strength of collagen, but to do that, it requires copper
- in order to use the copper it needs to be in its reduced cuprous form and that requires vitamin C
- but moving it around the body requires vitamin A
So in other words: if you are taking (or synthesizing) collagen, you also need copper and vitamins A and C.
However! Just to make things harder, if you take copper and vitamin C together, it’ll reduce the copper too soon in the wrong place.
Dr. DiNicolantonio therefore advises taking vitamin C after copper, with a 75 minutes gap between them.
What does he want us to know about glycine?
Glycine is one of the amino acids that makes up collagen. Specifically, it makes up every third amino acid in collagen, and even more specifically, it’s also the rate-limiting factor in the formation of glutathione, which is a potent endogenous (i.e., we make it inside us) antioxidant that works hard to fight inflammation inside the body.
What this means: if your joints are prone to inflammation, being glycine-deficient means a double-whammy of woe.
As well as being one of the amino acids most key to collagen production, glycine has another collagen-related role:
First, the problem: as we age, glycated collagen accumulates in the skin and cartilage (that’s bad; there is supposed to be collagen there, but not glycated).
More on glycation and what it is and why it is so bad:
Are You Eating Advanced Glycation End-Products? The Trouble Of The AGEs
Now, the solution: glycine suppresses advanced glycation end products, including the glycation of collagen.
See for example:
With these three important functions of glycine in mind…
Dr. DiNicolantonio therefore advises getting glycine at a dose of 100mg/kg/day. So, if you’re the same size as this rather medium-sized writer, that means 7.2g/day.
Where can I get it?
Glycine is found in many foods, including gelatin for those who eat that, eggs for the vegetarians, and spinach for vegans.
However, if you’d like to simply take it as a supplement, here’s an example product on Amazon
(the above product is not clear whether it’s animal-derived or not, so if that’s important to you, shop around. This writer got some locally that is certified vegan, but is in Europe rather than N. America, which won’t help most of our subscribers)
Note: pure glycine is a white crystalline powder that has the same sweetness as glucose. Indeed, that is how it got its name, from the Greek “γλυκύς”, pronounced /ɡly.kýs/, meaning “sweet”. Yes, same etymology as glucose.
So don’t worry that you’ve been conned if you order it and think “this is sugar!”; it just looks and tastes the same.
That does mean you should buy from a reputable source though, as a con would be very easy!
this does also mean that if you like a little sugar/sweetener in your tea or coffee, glycine can be used as a healthy substitute.
If you don’t like sweet tastes, then, condolences. This writer pours two espresso coffees (love this decaffeinated coffee that actually tastes good), puts the glycine in the first, and then uses the second to get rid of the sweet taste of the first. So that’s one way to do it.
Enjoy (if you can!)
Share This Post




Related Posts
-

Blueberry & Banana Collagen Baked Oats
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Good news for vegans/vegetarians! While we include an optional tablespoon of collagen powder in this recipe, the whole recipe is already geared around collagen synthesis, so it’s very collagen-boosting even with just the plants, providing collagen’s building blocks of protein, zinc, and vitamins C and D (your miraculous body will use these to assemble the collagen inside you).
You will need
- 2 cups oats, whence the protein and zinc
- 1 cup milk (your preference what kind; we recommend almond for flavor; whether you choose plant or animal though, it should be fortified with vitamin D)
- 2 bananas, peeled and mashed
- 4 oz blueberries, whence the vitamin C (frozen is fine) (chopped dried apricots are also a fine substitute if that’s more convenient)
- 1 oz flaked almonds, whence the protein and zinc
- 1 tbsp pumpkin seeds, whence the protein and zinc
- 1 tbsp flax seeds, whence the protein and zinc
- Optional: 1 tbsp maple syrup
- Optional: 1 tbsp collagen powder, dissolved in 1 oz hot water
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 350℉ / 180℃.
2) Mix the oats with 2 cups boiling water; allow to stand for 10–15 minutes, and then drain any excess water.
3) Mix the mashed bananas with the remaining ingredients except the milk and blueberries, stirring thoroughly.
4) Add the softened oats, and stir those in thoroughly too.
5) Add the milk and blueberries, in that order, stirring gently if using fresh blueberries, lest they get crushed.
6) Pour the mixture into an 8″ square cake tin that you have lined with baking paper, and smooth the top.
7) Bake for about 40 minutes or until firm and golden brown. Allow to cool; it will firm up more while it does.
8) Cut into squares or bars, and serve or store for later.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
We Are Such Stuff As Fish Are Made Of ← our main feature about collagen
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Some women’s breasts can’t make enough milk, and the effects can be devastating
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many new mothers worry about their milk supply. For some, support from a breastfeeding counsellor or lactation consultant helps.
Others cannot make enough milk no matter how hard they try. These are women whose breasts are not physically capable of producing enough milk.
Our recently published research gives us clues about breast features that might make it difficult for some women to produce enough milk. Another of our studies shows the devastating consequences for women who dream of breastfeeding but find they cannot.
Some breasts just don’t develop
Unlike other organs, breasts are not fully developed at birth. There are key developmental stages as an embryo, then again during puberty and pregnancy.
At birth, the breast consists of a simple network of ducts. Usually during puberty, the glandular (milk-making) tissue part of the breast begins to develop and the ductal network expands. Then typically, further growth of the ductal network and glandular tissue during pregnancy prepares the breast for lactation.
But our online survey of women who report low milk supply gives us clues to anomalies in how some women’s breasts develop.
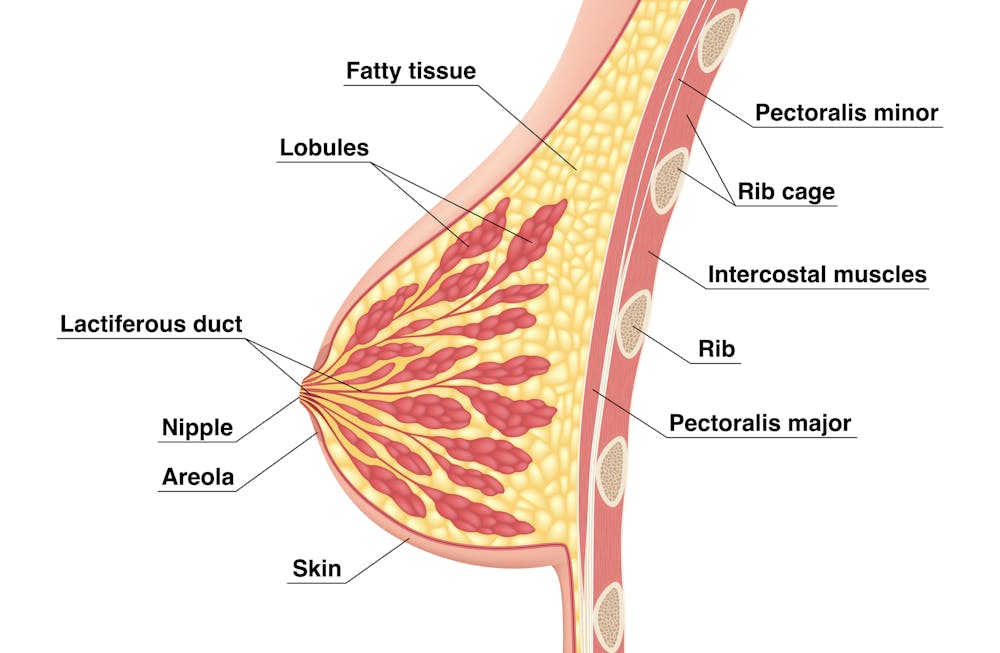
We’re not talking about women with small breasts, but women whose glandular tissue (shown in this diagram as “lobules”) is underdeveloped and have a condition called breast hypoplasia.
Sometimes not enough glandular tissue, shown here as lobules, develop.
Tsuyna/ShutterstockWe don’t know how common this is. But it has been linked with lower rates of exclusive breastfeeding.
We also don’t know what causes it, with much of the research conducted in animals and not humans.
However, certain health conditions have been associated with it, including polycystic ovary syndrome and other endocrine (hormonal) conditions. A high body-mass index around the time of puberty may be another indicator.
Could I have breast hypoplasia?
Our survey and other research give clues about who may have breast hypoplasia.
But it’s important to note these characteristics are indicators and do not mean women exhibiting them will definitely be unable to exclusively breastfeed.
Indicators include:
- a wider than usual gap between the breasts
- tubular-shaped (rather than round) breasts
- asymmetric breasts (where the breasts are different sizes or shapes)
- lack of breast growth in pregnancy
- a delay in or absence of breast fullness in the days after giving birth
In our survey, 72% of women with low milk supply had breasts that did not change appearance during pregnancy, and about 70% reported at least one irregular-shaped breast.
The effects
Mothers with low milk supply – whether or not they have breast hyoplasia or some other condition that limits their ability to produce enough milk – report a range of emotions.
Research, including our own, shows this ranges from frustration, confusion and surprise to intense or profound feelings of failure, guilt, grief and despair.
Some mothers describe “breastfeeding grief” – a prolonged sense of loss or failure, due to being unable to connect with and nourish their baby through breastfeeding in the way they had hoped.
These feelings of failure, guilt, grief and despair can trigger symptoms of anxiety and depression for some women.
Feelings of failure, guilt, grief and despair were common.
Bricolage/ShutterstockOne woman told us:
[I became] so angry and upset with my body for not being able to produce enough milk.
Many women’s emotions intensified when they discovered that despite all their hard work, they were still unable to breastfeed their babies as planned. A few women described reaching their “breaking point”, and their experience felt “like death”, “the worst day of [my] life” or “hell”.
One participant told us:
I finally learned that ‘all women make enough milk’ was a lie. No amount of education or determination would make my breasts work. I felt deceived and let down by all my medical providers. How dare they have no answers for me when I desperately just wanted to feed my child naturally.
Others told us how they learned to accept their situation. Some women said they were relieved their infant was “finally satisfied” when they began supplementing with formula. One resolved to:
prioritise time with [my] baby over pumping for such little amounts.
Where to go for help
If you are struggling with low milk supply, it can help to see a lactation consultant for support and to determine the possible cause.
This will involve helping you try different strategies, such as optimising positioning and attachment during breastfeeding, or breastfeeding/expressing more frequently. You may need to consider taking a medication, such as domperidone, to see if your supply increases.
If these strategies do not help, there may be an underlying reason why you can’t make enough milk, such as insufficient glandular tissue (a confirmed inability to make a full supply due to breast hypoplasia).
Even if you have breast hypoplasia, you can still breastfeed by giving your baby extra milk (donor milk or formula) via a bottle or using a supplementer (which involves delivering milk at the breast via a tube linked to a bottle).
More resources
The following websites offer further information and support:
- Australian Breastfeeding Association
- Lactation Consultants of Australia and New Zealand
- Royal Women’s Hospital, Melbourne
- Supply Line Breastfeeders Support Group of Australia Facebook support group
- IGT And Low Milk Supply Support Group Facebook support group
- Breastfeeding Medicine Network Australia/New Zealand
- Supporting breastfeeding grief (a collection of resources).
Shannon Bennetts, a research fellow at La Trobe University, contributed to this article.

Renee Kam, PhD candidate and research officer, La Trobe University and Lisa Amir, Professor in Breastfeeding Research, La Trobe University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Knitting helps Tom Daley switch off. Its mental health benefits are not just for Olympians
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Olympian Tom Daley is the most decorated diver in Britain’s history. He is also an avid knitter. At the Paris 2024 Olympics Daley added a fifth medal to his collection – and caught the world’s attention knitting a bright blue “Paris 24” jumper while travelling to the games and in the stands.
At the Tokyo Olympics, where Daley was first spotted knitting, he explained its positive impact on his mental health.
It just turned into my mindfulness, my meditation, my calm and my way to escape the stresses of everyday life and, in particular, going to an Olympics.
The mental health benefits of knitting are well established. So why is someone famous like Daley knitting in public still so surprising?
Africa Voice/Shutterstock Knitting is gendered
Knitting is usually associated with women – especially older women – as a hobby done at home. In a large international survey of knitting, 99% of respondents identified as female.
But the history of yarn crafts and gender is more tangled. In Europe in the middle ages, knitting guilds were exclusive and reserved for men. They were part of a respected Europe-wide trade addressing a demand for knitted products that could not be satisfied by domestic workers alone.
The industrial revolution made the production of clothed goods cheaper and faster than hand-knitting. Knitting and other needle crafts became a leisure activity for women, done in the private sphere of the home.
World Wars I and II turned the spotlight back on knitting as a “patriotic duty”, but it was still largely taken up by women.
During COVID lockdowns, knitting saw another resurgence. But knitting still most often makes headlines when men – especially famous men like Daley or actor Ryan Gosling – do it.
Men who knit are often seen as subverting the stereotype it’s an activity for older women.
Knitting the stress away
Knitting can produce a sense of pride and accomplishment. But for an elite sportsperson like Daley – whose accomplishments already include four gold medals and one silver – its benefits lie elsewhere.
Olympics-level sport relies on perfect scores and world records. When it comes to knitting, many of the mental health benefits are associated with the process, rather than the end result.
Daley says knitting is the “one thing” that allows him to switch off completely, describing it as “my therapy”. https://www.youtube.com/embed/6wwXGOki–c?wmode=transparent&start=0
The Olympian says he could
knit for hours on end, honestly. There’s something that’s so satisfying to me about just having that rhythm and that little “click-clack” of the knitting needles. There is not a day that goes by where I don’t knit.
Knitting can create a “flow” state through rhythmic, repetitive movements of the yarn and needle. Flow offers us a balance between challenge, accessibility and a sense of control.
It’s been shown to have benefits relieving stress in high-pressure jobs beyond elite sport. Among surgeons, knitting has been found to improve wellbeing as well as manual dexterity, crucial to their role.
For other health professionals – including oncology nurses and mental health workers – knitting has helped to reduce “compassion fatigue” and burnout. Participants described the soothing noise of their knitting needles. They developed and strengthened team bonds through collective knitting practices. https://www.youtube.com/embed/dTTJjD_q2Ik?wmode=transparent&start=0 A Swiss psychiatrist says for those with trauma, knitting yarn can be like “knitting the two halves” of the brain “back together”.
Another study showed knitting in primary school may boost children’s executive function. That includes the ability to pay attention, remember relevant details and block out distractions.
As a regular creative practice, it has also been used in the treatment of grief, depression and subduing intrusive thoughts, as well countering chronic pain and cognitive decline.
Knitting is a community
The evidence for the benefits of knitting is often based on self-reporting. These studies tend to produce consistent results and involve large population samples.
This may point to another benefit of knitting: its social aspect.
Knitting and other yarn crafts can be done alone, and usually require simple materials. But they also provide a chance to socialise by bringing people together around a common interest, which can help reduce loneliness.
The free needle craft database and social network Ravelry contains more than one million patterns, contributed by users. “Yarn bombing” projects aim to engage the community and beautify public places by covering objects such as benches and stop signs with wool.
The interest in Daley’s knitting online videos have formed a community of their own.
In them he shows the process of making the jumper, not just the finished product. That includes where he “went wrong” and had to unwind his work.
His pride in the finished product – a little bit wonky, but “made with love” – can be a refreshing antidote to the flawless achievements often on display at the Olympics.
Michelle O’Shea, Senior Lecturer, School of Business, Western Sydney University and Gabrielle Weidemann, Associate Professor in Psychological Science, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: