Red Lentils vs Oats – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing red lentils to oats, we picked the oats.
Why?
In terms of macros, oats have more protein, carbs, fiber, and even a little fat—mostly healthy mono- and polyunsaturated fats, thus making them the more nutritionally dense. That said, red lentils have the lower glycemic index, (low GI compared to oats’ medium GI) which offsets that, so we’ll call this category a tie.
In the category of vitamins, red lentils have more of vitamins B6, B9, and choline, while oats have more of vitamins B1, B2, and B5. Another tie!
When it comes to minerals, however, we have a tiebreaker category: red lentils have more selenium, while oats have more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, and zinc. An easy win for oats this time!
So, thanks to the minerals, oats are the clear winner in total. But by all means, enjoy either or both; diversity is good!
Want to learn more?
You might like to read:
The Best Kind Of Fiber For Overall Health? ← it’s β-glucan, the kind find in oats!
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Pomegranate vs Cherries – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing pomegranate to cherries, we picked the pomegranate.
Why?
In terms of macros, pomegranate is slightly higher in carbs, and/but 4x higher in fiber. That’s already a good start for pomegranates. Lest we be accused of cherry-picking, though, we’ll mention that pomegranate is also slightly higher in protein and fat, for what it’s worth—which is not a lot. As with most fruits, the protein and fat numbers are low importance next to the carb:fiber ratio.
When it comes to vitamins, pomegranate has more of vitamins B1, B2, B5, B6, B9. E. K, and choline. On the other hand, cherries have more of vitamins A and B3. The two fruits are equal in vitamin C. This all makes for a clear win for pomegranate.
In the category of minerals, pomegranate boasts more copper, magnesium, phosphorus, potassium, selenium, and zinc. In contrast, cherries have slightly more calcium. Another win for pomegranate.
Both of these fruits have beneficial polyphenols, each with a slightly different profile, but neither pressingly better than the other.
In short: as ever with healthy foods, enjoy both—diversity is good! But if you’re going to pick on, we recommend the pomegranate.
Want to learn more?
You might like to read:
- Pomegranate Peel’s Potent Potential ← so don’t throw it away!
- Cherries’ Very Healthy Wealth Of Benefits!
Take care!
Share This Post
-

When BMI Doesn’t Measure Up
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When BMI Doesn’t Quite Measure Up
Last month, we did a “Friday Mythbusters” edition of 10almonds, tackling many of the misconceptions surrounding obesity. Amongst them, we took a brief look at the usefulness (or lack thereof) of the Body Mass Index (BMI) scale of weight-related health for individuals. By popular subscriber request, we’re now going to dive a little deeper into that today!
The wrong tool for the job
BMI was developed as a tool to look at large-scale demographic trends, stemming from a population study of white European men, who were for the purpose of the study (the widescale health of the working class in that geographic area in that era), considered a reasonable default demographic.
In other words: as a system, it’s now being used in a way it was never made for, and the results of that misappropriation of an epidemiological tool for individual health are predictably unhelpful.
If you want to know yours…
Here’s the magic formula for calculating your BMI:
- Metric: divide your weight in kilograms by your height in square meters
- Imperial: divide your weight in pounds by your height in square inches and then multiply by 703
“What if my height doesn’t come in square meters or square inches, because it’s a height, not an area?”
We know. Take your height and square it anyway. If this seems convoluted and arbitrary, yes, it is.
But!
While on the one hand it’s convoluted and arbitrary… On the other hand, it’s also a gross oversimplification. So, yay for the worst of both worlds?
If you don’t want to grab a calculator, here’s a quick online tool to calculate it for you.
So, how did you score?
According to the CDC, a BMI score…
- Under 18.5 is underweight
- 18.5 to 24.9 is normal
- 25 to 29.9 is overweight
- 30 and over is obese
And, if we’re looking at a representative sample of the population, where the representation is average white European men of working age, that’s not a bad general rule of thumb.
For the rest of us, not so representative
BMI is a great and accurate tool as a rule of thumb, except for…
Women
An easily forgotten demographic, due to being a mere 51% of the world’s population, women generally have a higher percentage of body fat than men, and this throws out BMI’s usefulness.
If pregnant or nursing
A much higher body weight and body fat percentage—note that these are two things, not one. Some of the extra weight will be fat to nourish the baby; some will be water weight, and if pregnant, some will be the baby (or babies!). BMI neither knows nor cares about any of these things. And, this is a big deal, because BMI gets used by healthcare providers to judge health risks and guide medical advice.
People under the age of 16 or over the age of 65
Not only do people below and above those ages (respectively) tend to be shorter—which throws out the calculations and mean health risks may increase before the BMI qualifies as overweight—but also:
- BMI under 23 in people over the age of 65 is associated with a higher health risk
- A meta-analysis showed that a BMI of 27 was the best in terms of decreased mortality risk for the over-65 age group
This obviously flies in the face of conventional standards regards BMI—as you’ll recall from the BMI brackets we listed above.
Read the science: BMI and all-cause mortality in older adults: a meta-analysis
Athletic people
A demographic often described in scientific literature as “athletes”, but that can be misleading. When we say “athletes”, what comes to mind? Probably Olympians, or other professional sportspeople.
But also athletic, when it comes to body composition, are such people as fitness enthusiasts and manual laborers. Which makes for a lot more people affected by this!
Athletic people tend to have more lean muscle mass (muscle weighs more than fat), and heavier bones (can’t build strong muscles on weak bones, so the bones get stronger too, which means denser)… But that lean muscle mass can actually increase metabolism and help ward off many of the very same things that BMI is used as a risk indicator for (e.g. heart disease, and diabetes). So people in this category will actually be at lower risk, while (by BMI) getting told they are at higher risk.
If not white
Physical characteristics of race can vary by more than skin color, relevant considerations in this case include, for example:
- Black people, on average, not only have more lean muscle mass and less fat than white people, but also, have completely different risk factors for diseases such as diabetes.
- Asian people, on average, are shorter than white people, and as such may see increased health risks before BMI qualifies as overweight.
- Hispanic people, on average, again have different physical characteristics that throw out the results, in a manner that would need lower cutoffs to be even as “useful” as it is for white people.
Further reading on this: BMI and the BIPOC Community
In summary:
If you’re an average white European working-age man, BMI can sometimes be a useful general guide. If however you fall into one or more of the above categories, it is likely to be inaccurate at best, if not outright telling the opposite of the truth.
What’s more useful, then?
For heart disease risk and diabetes risk both, waist circumference is a much more universally reliable indicator. And since those two things tend to affect a lot of other health risks, it becomes an excellent starting point for being aware of many aspects of health.
Pregnancy will still throw off waist circumference a little (measure below the bump, not around it!), but it will nevertheless be more helpful than BMI even then, as it becomes necessary to just increase the numbers a little, according to gestational month and any confounding factors e.g. twins, triplets, etc. Ask your obstetrician about this, as it’s beyond the scope of today’s newsletter!
As to what’s considered a risk:
- Waist circumference of more than 35 inches for women
- Waist circumference of more than 40 inches for men
These numbers are considered applicable across demographics of age, sex, ethnicity, and lifestyle.
There are more options than just waist circumference though; we delve into them in detail here:
Take care!
Share This Post
-
Cows’ Milk, Bird Flu, & You
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to dairy products, generally speaking, fermented ones (such as most cheeses and yogurts) are considered healthy in moderation, and unfermented ones have their pros and cons that can be argued and quibbled “until the cows come home”. We gave a broad overview, here:
Furthermore, you may recall that there’s some controversy/dissent about when human babies can have cows’ milk:
When can my baby drink cow’s milk? It’s sooner than you think
So, what about bird flu now?
Earlier this year, the information from the dairy industry was that it was nothing to be worried about for the time being:
Bird Flu Is Bad for Poultry and Dairy Cows. It’s Not a Dire Threat for Most of Us — Yet.
More recently, the latest science has found:
❝We found a first-order decay rate constant of −2.05 day–1 equivalent to a T99 of 2.3 days. Viral RNA remained detectable for at least 57 days with no degradation. Pasteurization (63 °C for 30 min) reduced infectious virus to undetectable levels and reduced viral RNA concentrations, but reduction was less than 1 log10.
The prolonged persistence of viral RNA in both raw and pasteurized milk has implications for food safety assessments and environmental surveillance❞
You can find the study here:
Infectivity and Persistence of Influenza A Virus in Raw Milk
In short: raw milk keeps the infectious virus; pasteurization appears to render it uninfectious, though viral RNA remains present.
This is relevant, because of the bird flu virus being found in milk:
World Health Organization | H5N1 strain of bird flu found in milk
To this end, a moratorium has been placed on the sale of raw milk, first by the California Dept of Public Health (following an outbreak in California):
California halts sales of raw milk due to bird flu virus contamination
And then, functionally, by the USDA, though rather than an outright ban, it’s requiring testing for the virus:
USDA orders testing of milk supply for presence of bird flu virus
So, is pasteurized milk safe?
The official answer to this, per the FDA, is… Honestly, a lot of hand-wringing and shrugging. What we do know is:
- the bird flu virus has been found in pasteurized milk too
- the test for this is very sensitive, and has the extra strength/weakness that viral fragments will flag it as a positive
- it is assumed that the virus was inactivated by the pasteurization process
- it could, however, have been the entire virus, the test simply does not tell us which
In the FDA’s own words:
❝The pasteurization process has served public health well for more than 100 years. Even if the virus is detected in raw milk, pasteurization is generally expected to eliminate pathogens to a level that does not pose a risk to consumer health❞
So, there we have it: the FDA does not have a reassurance exactly, but it does have a general expectation.
Source: US Officials: Bird flu viral fragments found in pasteurized milk
Want to know more?
You might like this mythbusting edition we did a little while back:
Pasteurization: What It Does And Doesn’t Do ← this is about its effect on risks and nutrients
Take care!
Share This Post

Related Posts
-
Don’t Do *This* If You’re Over 50 (And Want Better Sleep)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Michael Breus, sleep specialist, explains:
Don’t make these mistakes
Dr. Breus recommends avoiding…
- Misusing magnesium: magnesium is a helpful sleep aid but must be carefully monitored. Recommended doses are 250mg for women and 300–350 mg for men, with slight adjustments for hot climates or active lifestyles. Overdosing can cause stomach issues, diarrhea, and dehydration, disrupting sleep. He recommends starting with magnesium glycinate for fewer stomach issues, and later mix with magnesium citrate. Always check supplements to avoid excessive magnesium intake.
- Misusing melatonin: melatonin production declines after age 55–60, making low-dose supplementation (0.5–1 mg) beneficial. He recommends, however, avoiding high doses (3–10mg), and he recommends to take it 90 minutes before bedtime. Melatonin interacts with some medications (including some meds for blood pressure or depression), so consult a pharmacist before use to avoid risks like serotonin syndrome.
- Going to bed too early: going to bed too early disrupts circadian rhythms and reduces sleep drive, causing earlier waking. Now, being an “early bird” is a generally healthy thing, but if you’re already getting up at 5am, say, you probably want your schedule to not continue to creep further forwards until you become nocturnal. Set a consistent wake-up time and count 7.5 hours backward (plus a set time to fall asleep, e.g. 20 minutes, but you’ll know what it is for you) to determine bedtime.
- Excessive caffeine consumption: from the heading, it may seem like a no-brainer, but older adults metabolize caffeine 33% slower on average, prolonging its effects. Dr. Breus recommends to reduce intake with “caffeine fading,” switching to half-caffeinated coffee for a while and then considering transitioning to decaf. He also suggests enjoying increasingly lower-caffeine teas, like black tea in the morning, matcha in the afternoon, and herbal tea at night to reduce caffeine’s impact on sleep.
- Falling foul of serotonin: avoid taking 5-HTP supplements with SSRI antidepressants like Prozac or Zoloft due to the risk of serotonin syndrome.
- Consider checking for physical problems: if you regularly wake up tired and/or groggy (despite having ostensibly had enough sleep, and there not being a pharmaceutical explanation for your grogginess), consider screening for sleep apnea. Home sleep tests are a convenient way to identify and treat this common but often undiagnosed condition.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
How to Fall Asleep Faster: CBT-Insomnia Treatment
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Dating apps could have negative effects on body image and mental health, our research shows
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Around 350 million people globally use dating apps, and they amass an estimated annual revenue of more than US$5 billion. In Australia, 49% of adults report using at least one online dating app or website, with a further 27% having done so in the past.
But while dating apps have helped many people find romantic partners, they’re not all good news.
In a recent review, my colleagues and I found using dating apps may be linked to poorer body image, mental health and wellbeing.

Dikushin Dmitry/Shutterstock We collated the evidence
Our study was a systematic review, where we collated the results of 45 studies that looked at dating app use and how this was linked to body image, mental health or wellbeing.
Body image refers to the perceptions or feelings a person has towards their own appearance, often relating to body size, shape and attractiveness.
Most of the studies we included were published in 2020 onwards. The majority were carried out in Western countries (such as the United States, the United Kingdom and Australia). Just under half of studies included participants of all genders. Interestingly, 44% of studies observed men exclusively, while only 7% included just women.
Of the 45 studies, 29 looked at the impact of dating apps on mental health and wellbeing and 22 considered the impact on body image (some looked at both). Some studies examined differences between users and non-users of dating apps, while others looked at whether intensity of dating app use (how often they’re used, how many apps are used, and so on) makes a difference.
More than 85% of studies (19 of 22) looking at body image found significant negative relationships between dating app use and body image. Just under half of studies (14 of 29) observed negative relationships with mental health and wellbeing.
The studies noted links with problems including body dissatisfaction, disordered eating, depression, anxiety and low self-esteem.
Dating apps are becoming increasingly common. But could their use harm mental health? Rachata Teyparsit/Shutterstock It’s important to note our research has a few limitations. For example, almost all studies included in the review were cross-sectional – studies that analyse data at a particular point in time.
This means researchers were unable to discern whether dating apps actually cause body image, mental health and wellbeing concerns over time, or whether there is simply a correlation. They can’t rule out that in some cases the relationship may go the other way, meaning poor mental health or body image increases a person’s likelihood of using dating apps.
Also, the studies included in the review were mostly conducted in Western regions with predominantly white participants, limiting our ability to generalise the findings to all populations.
Why are dating apps linked to poor body image and mental health?
Despite these limitations, there are plausible reasons to expect there may be a link between dating apps and poorer body image, mental health and wellbeing.
Like a lot of social media, dating apps are overwhelmingly image-centric, meaning they have an emphasis on pictures or videos. Dating app users are initially exposed primarily to photos when browsing, with information such as interests or hobbies accessible only after manually clicking through to profiles.
Because of this, users often evaluate profiles based primarily on the photos attached. Even when a user does click through to another person’s profile, whether or not they “like” someone may still often be determined primarily on the basis of physical appearance.
This emphasis on visual content on dating apps can, in turn, cause users to view their appearance as more important than who they are as a person. This process is called self-objectification.
People who experience self-objectification are more likely to scrutinise their appearance, potentially leading to body dissatisfaction, body shame, or other issues pertaining to body image.
Dating apps are overwhelmingly image-centric. Studio Romantic/Shutterstock There could be several reasons why mental health and wellbeing may be impacted by dating apps, many of which may centre around rejection.
Rejection can come in many forms on dating apps. It can be implied, such as having a lack of matches, or it can be explicit, such as discrimination or abuse. Users who encounter rejection frequently on dating apps may be more likely to experience poorer self-esteem, depressive symptoms or anxiety.
And if rejection is perceived to be based on appearance, this could lead again to body image concerns.
What’s more, the convenience and game-like nature of dating apps may lead people who could benefit from taking a break to keep swiping.
What can app developers do? What can you do?
Developers of dating apps should be seeking ways to protect users against these possible harms. This could, for example, include reducing the prominence of photos on user profiles, and increasing the moderation of discrimination and abuse on their platforms.
The Australian government has developed a code of conduct – to be enforced from April 1 this year – to help moderate and reduce discrimination and abuse on online dating platforms. This is a positive step.
Despite the possible negatives, research has also found dating apps can help build confidence and help users meet new people.
If you use dating apps, my colleagues and I recommend choosing profile images you feel display your personality or interests, or photos with friends, rather than semi-clothed images and selfies. Engage in positive conversations with other users, and block and report anyone who is abusive or discriminatory.
It’s also sensible to take breaks from the apps, particularly if you’re feeling overwhelmed or dejected.
If this article has raised issues for you, or if you’re concerned about someone you know, call Lifeline on 13 11 14. The Butterfly Foundation provides support for eating disorders and body image issues, and can be reached on 1800 334 673.
Zac Bowman, PhD Candidate, College of Education, Psychology & Social Work, Flinders University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Red Light, Go!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Casting Yourself In A Healthier Light

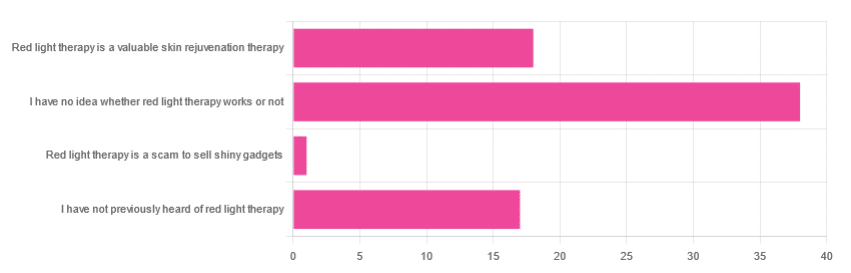
In Tuesday’s newsletter, we asked you for your opinion of red light therapy (henceforth: RLT), and got the above-depicted, below-described, set of responses:
- About 51% said “I have no idea whether light therapy works or not”
- About 24% said “Red light therapy is a valuable skin rejuvenation therapy”
- About 23% said “I have not previously heard of red light therapy”
- One (1) person said: “Red light therapy is a scam to sell shiny gadgets”
A number of subscribers wrote with personal anecdotes of using red light therapy to beneficial effect, for example:
❝My husband used red light therapy after surgery on his hand. It did seem to speed healing of the incision and there is very minimal scarring. I would like to know if the red light really helped or if he was just lucky❞
~ 10almonds subscriber
And one wrote to report having observed mixed results amongst friends, per:
❝Some people it works, others I’ve seen it breaks them out❞
~ 10almonds subscriber
So, what does the science say?
RLT rejuvenates skin, insofar as it reduces wrinkles and fine lines: True or False?
True! This one’s pretty clear-cut, so we’ll just give one example study of many, which found:
❝The treated subjects experienced significantly improved skin complexion and skin feeling, profilometrically assessed skin roughness, and ultrasonographically measured collagen density.
The blinded clinical evaluation of photographs confirmed significant improvement in the intervention groups compared with the control❞
~ Dr. Alexander Wunsch & Dr. Karsten Matuschka
RLT helps speed up healing of wounds: True or False?
True! There is less science for this than the above claim, but the studies that have been done are quite compelling, for example this NASA technology study found that…
❝LED produced improvement of greater than 40% in musculoskeletal training injuries in Navy SEAL team members, and decreased wound healing time in crew members aboard a U.S. Naval submarine.❞
Read more: Effect of NASA light-emitting diode irradiation on wound healing
RLT’s benefits are only skin-deep: True or False?
False, probably, but we’d love to see more science for this, to be sure.
However, it does look like wavelengths in the near-infrared spectrum reduce the abnormal tau protein and neurofibrillary tangles associated with Alzheimer’s disease, resulting in increased blood flow to the brain, and a decrease in neuroinflammation:
Therapeutic Potential of Photobiomodulation In Alzheimer’s Disease: A Systematic Review
Would you like to try RLT for yourself?
There are some contraindications, for example:
- if you have photosensitivity (for obvious reasons)
- if you have Lupus (mostly because of the above)
- if you have hyperthyroidism (because if you use RLT to your neck as well as face, it may help stimulate thyroid function, which in your case is not what you want)
As ever, please check with your own doctor if you’re not completely sure; we can’t cover all bases here, and cannot speak for your individual circumstances.
For most people though, it’s very safe, and if you’d like to try it, here’s an example product on Amazon, and by all means do read reviews and shop around for the ideal device for you
Take care! 😎
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: