Rebuilding Milo – by Dr. Aaron Horschig
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The author, a doctor of physical therapy, also wrote another book that we reviewed a while ago, “The Squat Bible” (which is also excellent, by the way). This time, it’s all about resistance training in the context of fixing a damaged body.
Resistance training is, of course, very important for general health, especially as we get older. However, it’s easy to do it wrongly and injure oneself, and indeed, if one is carrying some injury and/or chronic pain, it becomes necessary to know how to fix that before continuing—without just giving up on training, because that would be a road to ruin in terms of muscle and bone maintenance.
The book explains all the necessary anatomy, with clear illustrations too. He talks equipment, keeping things simple and practical, letting the reader know which things actually matter in terms of quality, and what things are just unnecessary fanciness and/or counterproductive.
Most of the book is divided into chapters per body part, e.g. back pain, shoulder pain, ankle pain, hip pain, knee pain, etc; what’s going on, and how to fix it to rebuild it stronger.
The style is straightforward and simple, neither overly clinical nor embellished with overly casual fluff. Just, clear simple explanations and instructions.
Bottom line: if you’d like to get stronger and/or level up your resistance training, but are worried about an injury or chronic condition, this book can set you in good order.
Click here to check out Rebuilding Milo, and rebuild yourself!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What Happens To Your Body When You Do 100 Glute Bridges Every Day

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Not just for a sculpted butt:
Benefits
With consistent daily glute bridge practice, you may expect:
- Rounder, toned butt: targets the gluteus maximus, toning and lifting the butt for a rounder appearance.
- Improved posture: strengthens glutes to support the spine and pelvis, alleviating lower back and hip pain. Stretches tight hip flexors from prolonged sitting.
- Stronger lower back: glutes support the lower back and spine, reducing pain and making it easier to lift heavy objects. Activating the glutes transfers force from legs to core, preventing injuries.
- Stronger knees: stabilizes the knee joint and promotes alignment by engaging glutes, hamstrings, and quadriceps, reducing knee pain.
- Sculpted hamstrings: contracts hamstrings during lifts for strength, while stretching them on the way down increases flexibility.
- Increased hip flexibility: strengthens muscles around the hip joint, improving mobility and counteracting tight hips from sedentary habits.
- Reduced back pain: strengthens glutes to correct pelvic tilt and reduce strain on the lower back.
- Faster running speed: improves hip extension, strengthens hamstrings, and activates the gluteus medius for better running power and balance.
- Enhanced strength training performance: strengthens glutes, back, and knees, improving performance in exercises like squats and deadlifts.
As for how to get going, the video offers the following very sound advice: begin with 25–30 reps per session and gradually increase to sets of 100 daily. It should take about 5 minutes (that’s 3 seconds per repetition). Results can be seen in as little as 2 weeks, with significant changes after a month of consistent practice.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Strong Curves: A Woman’s Guide to Building a Better Butt and Body – by Bret Contreras & Kellie Davis
Take care!
Share This Post
-
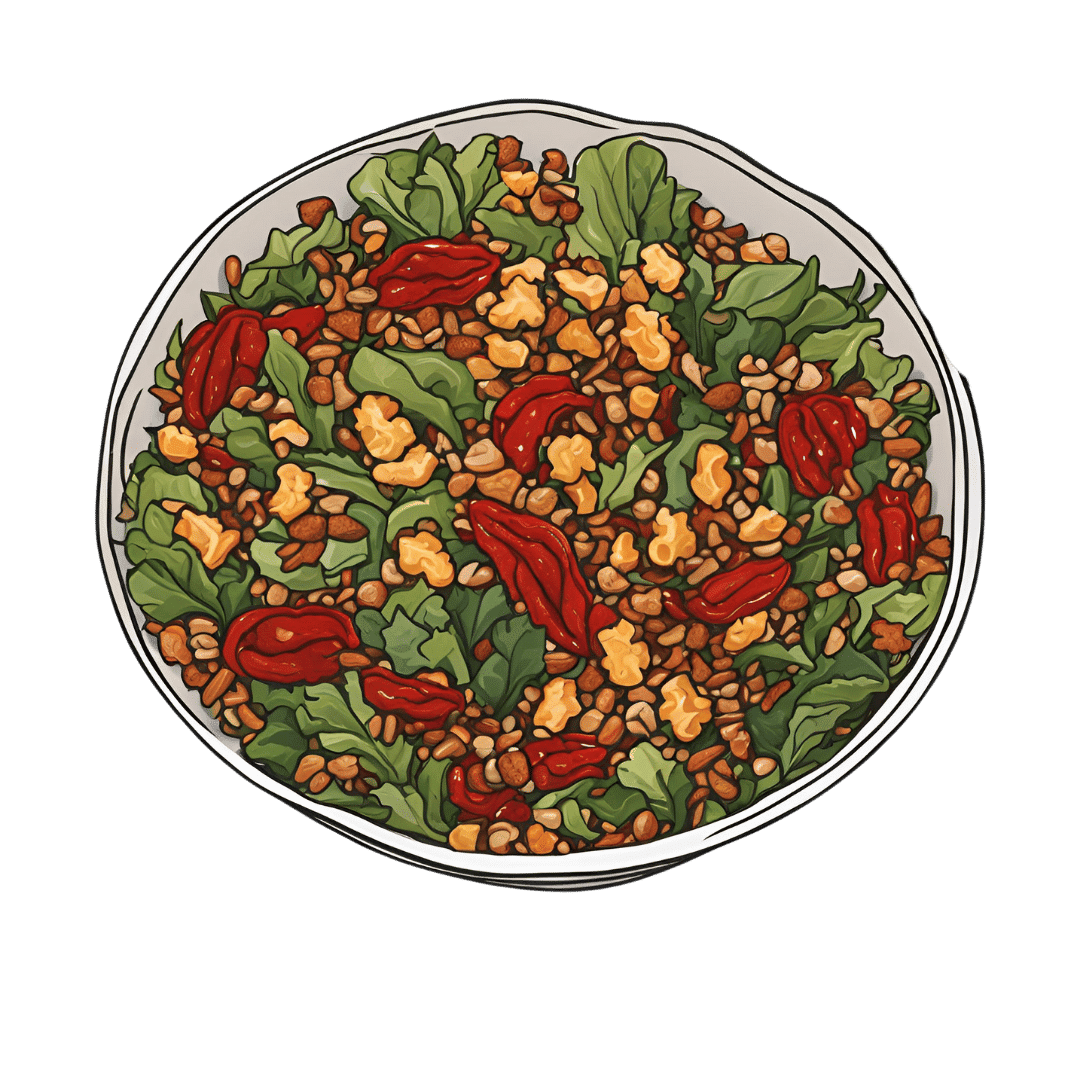
Crispy Tempeh & Warming Mixed Grains In Harissa Dressing
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Comfort food that packs a nutritional punch! Lots of protein, fiber, vitamins, minerals, and healthy fats, and more polyphenols than you can shake a fork at.
You will need
- 1 lb cooked mixed whole grains (your choice what kind; gluten-free options include buckwheat, quinoa, millet)
- 7 oz tempeh, cut into ½” cubes
- 2 red peppers, cut into strips
- 10 baby plum tomatoes, halved
- 1 avocado, pitted, peeled, and diced
- 1 bulb garlic, paperwork done but cloves left whole
- 1 oz black olives, pitted and halved
- 4 tbsp extra virgin olive oil
- 2 tbsp harissa paste
- 2 tbsp soy sauce (ideally tamari)
- 1 tbsp nutritional yeast
- 1 tbsp chia seeds
- 2 tsp black pepper, coarse ground
- 1 tsp red chili flakes
- 1 handful chopped fresh flat-leaf parsley
- ½ tsp MSG or 1 tsp low-sodium salt
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 400℉ / 200℃.
2) Combine the red pepper strips with the tomatoes, garlic, 2 tbsp of the olive oil, and the MSG/salt, tossing thoroughly to ensure an even coating. Spread them on a lined baking tray, and roast for about 25 minutes. Remove when done, and allow to cool a little.
3) Combine the tempeh with the soy sauce and nutritional yeast flakes, tossing thoroughly to ensure an even coating. Spread them on a lined baking tray, and roast for about 25 minutes, tossing regularly to ensure it is crispy on all sides. If you get started on the tempeh as soon as the vegetables are in the oven, these should be ready only a few minutes after the vegetables.
4) Whisk together the remaining olive oil and harissa paste in a small bowl, to make the dressing,
5) Mix everything in a big serving bowl. By “everything” we mean the roasted vegetables, the crispy tempeh, the mixed grains, the dressing, the chia seeds, the black pepper, the red chili flakes, and the flat leaf parsley.
6) Serve warm.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Grains: Bread Of Life, Or Cereal Killer?
- Tempeh vs Tofu – Which is Healthier?
- Our Top 5 Spices: How Much Is Enough For Benefits?
Take care!
Share This Post
-

Cognitive Enhancement Without Drugs
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cognitive Enhancement Without Drugs

This is Elizabeth Ricker. She’s a Harvard-and-MIT-trained neuroscientist and researcher, who now runs the “Citizen Science” DIY-neurohacking organization, NeuroEducate.
Sounds fun! What’s it about?
The philosophy that spurs on her research and practice can be summed up as follows:
❝I’m not going to leave my brain up to my doctor or [anyone else]… My brain is my own responsibility, and I’m going to do the best that I can to optimize it❞
Her goal is not just to optimize her own brain though; she wants to make the science accessible to everyone.
What’s this about Citizen Science?
“Citizen Science” is the idea that while there’s definitely an important role in society for career academics, science itself should be accessible to all. And, not just the conclusions, but the process too.
This can take the form of huge experiments, often facilitated these days by apps where we opt-in to allow our health metrics (for example) to be collated with many thousands of others, for science. It can also involve such things as we talked about recently, getting our own raw genetic data and “running the numbers” at home to get far more comprehensive and direct information than the genetic testing company would ever provide us.
For Ricker, her focus is on the neuroscience side of biohacking, thus, neurohacking.
I’m ready to hack my brain! Do I need a drill?
Happily not! Although… Bone drills for the skull are very convenient instruments that make it quite hard to go wrong even with minimal training. The drill bit has a little step/ledge partway down, which means you can only drill through the thickness of the skull itself, before the bone meeting the wider part of the bit stops you from accidentally drilling into the brain. Still, please don’t do this at home.
What you can do at home is a different kind of self-experimentation…
If you want to consider which things are genuinely resulting in cognitive enhancement and which things are not, you need to approach the matter like a scientist. That means going about it in an organized fashion, and recording results.
There are several ways cognitive enhancement can be measured, including:
- Learning and memory
- Executive function
- Emotional regulation
- Creative intelligence
Let’s look at each of them, and what can be done. We don’t have a lot of room here; we’re a newsletter not a book, but we’ll cover one of Ricker’s approaches for each:
Learning and memory
This one’s easy. We’re going to leverage neuroplasticity (neurons that fire together, wire together!) by simple practice, and introduce an extra element to go alongside your recall. Perhaps a scent, or a certain item of clothing. Tell yourself that clinical studies have shown that this will boost your recall. It’s true, but that’s not what’s important; what’s important is that you believe it, and bring the placebo effect to bear on your endeavors.
You can test your memory with word lists, generated randomly by AI, such as this one:
You’ll soon find your memory improving—but don’t take our word for it!
Executive function
Executive function is the aspect of your brain that tells the other parts how to work, when to work, and when to stop working. If you’ve ever spent 30 minutes thinking “I need to get up” but you were stuck in scrolling social media, that was executive dysfunction.
This can be trained using the Stroop Color and Word Test, which shows you words, specifically the names of colors, which will themselves be colored, but not necessarily in the color the word pertains to. So for example, you might be shown the word “red”, colored green. Your task is to declare either the color of the word only, ignoring the word itself, or the meaning of the word only, ignoring its appearance. It can be quite challenging, but you’ll get better quite quickly:
The Stroop Test: Online Version
Emotional Regulation
This is the ability to not blow up angrily at the person with whom you need to be diplomatic, or to refrain from laughing when you thought of something funny in a sombre situation.
It’s an important part of cognitive function, and success or failure can have quite far-reaching consequences in life. And, it can be trained too.
There’s no online widget for this one, but: when and if you’re in a position to safely* do so, think about something that normally triggers a strong unwanted emotional reaction. It doesn’t have to be something life-shattering, but just something that you feel in some way bad about. Hold this in your mind, sit with it, and practice mindfulness. The idea is to be able to hold the unpleasant idea in your mind, without becoming reactive to it, or escaping to more pleasant distractions. Build this up.
*if you perchance have PTSD, C-PTSD, or an emotional regulation disorder, you might want to talk this one through with a qualified professional first.
Creative Intelligence
Another important cognitive skill, and again, one that can be cultivated and grown.
The trick here is volume. A good, repeatable test is to think of a common object (e.g. a rock, a towel, a banana) and, within a time constraint (such as 15 minutes) list how many uses you can think of for that item.
Writer’s storytime: once upon a time, I was sorting through an inventory of medical equipment with a colleague, and suggested throwing out our old arterial clamps, as we had newer, better ones—in abundance. My colleague didn’t want to part with them, so I challenged him “Give me one use for these, something we could in some possible world use them for that the new clamps don’t do better, and we’ll keep them”. He said “Thumbscrews”, and I threw my hands up in defeat, saying “Fine!”, as he had technically fulfilled my condition.
What’s the hack to improve this one? Just more volume. Creativity, as it turns out, isn’t something we can expend—like a muscle, it grows the more we use it. And because the above test is repeatable (with different objects), you can track your progress.
And if you feel like using your grown creative muscle to write/paint/compose/etc your magnum opus, great! Or if you just want to apply it to the problem-solving of everyday life, also great!
In summary…
Our brain is a wonderful organ with many functions. Society expects us to lose these as we get older, but the simple, scientific truth is that we can not only maintain our cognitive function, but also enhance and grow it as we go.
Want to know more from today’s featured expert?
You might enjoy her book, “Smarter Tomorrow”, which we reviewed back in March
Share This Post

-
Most adults will gain half a kilo this year – and every year. Here’s how to stop ‘weight creep’
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
As we enter a new year armed with resolutions to improve our lives, there’s a good chance we’ll also be carrying something less helpful: extra kilos. At least half a kilogram, to be precise.
“Weight creep” doesn’t have to be inevitable. Here’s what’s behind this sneaky annual occurrence and some practical steps to prevent it.

Allgo/Unsplash Small gains add up
Adults tend to gain weight progressively as they age and typically gain an average of 0.5 to 1kg every year.
While this doesn’t seem like much each year, it amounts to 5kg over a decade. The slow-but-steady nature of weight creep is why many of us won’t notice the extra weight gained until we’re in our fifties.
Why do we gain weight?
Subtle, gradual lifestyle shifts as we progress through life and age-related biological changes cause us to gain weight. Our:
- activity levels decline. Longer work hours and family commitments can see us become more sedentary and have less time for exercise, which means we burn fewer calories
- diets worsen. With frenetic work and family schedules, we sometimes turn to pre-packaged and fast foods. These processed and discretionary foods are loaded with hidden sugars, salts and unhealthy fats. A better financial position later in life can also result in more dining out, which is associated with a higher total energy intake
- sleep decreases. Busy lives and screen use can mean we don’t get enough sleep. This disturbs our body’s energy balance, increasing our feelings of hunger, triggering cravings and decreasing our energy
Insufficient sleep can increase our appetite. Craig Adderley/Pexels - stress increases. Financial, relationship and work-related stress increases our body’s production of cortisol, triggering food cravings and promoting fat storage
- metabolism slows. Around the age of 40, our muscle mass naturally declines, and our body fat starts increasing. Muscle mass helps determine our metabolic rate, so when our muscle mass decreases, our bodies start to burn fewer calories at rest.
We also tend to gain a small amount of weight during festive periods – times filled with calorie-rich foods and drinks, when exercise and sleep are often overlooked. One study of Australian adults found participants gained 0.5 kilograms on average over the Christmas/New Year period and an average of 0.25 kilograms around Easter.
Why we need to prevent weight creep
It’s important to prevent weight creep for two key reasons:
1. Weight creep resets our body’s set point
Set-point theory suggests we each have a predetermined weight or set point. Our body works to keep our weight around this set point, adjusting our biological systems to regulate how much we eat, how we store fat and expend energy.
When we gain weight, our set point resets to the new, higher weight. Our body adapts to protect this new weight, making it challenging to lose the weight we’ve gained.
But it’s also possible to lower your set point if you lose weight gradually and with an interval weight loss approach. Specifically, losing weight in small manageable chunks you can sustain – periods of weight loss, followed by periods of weight maintenance, and so on, until you achieve your goal weight.
Holidays can also come with weight gain. Zan Lazarevic/Unsplash 2. Weight creep can lead to obesity and health issues
Undetected and unmanaged weight creep can result in obesity which can increase our risk of heart disease, strokes, type 2 diabetes, osteoporosis and several types of cancers (including breast, colorectal, oesophageal, kidney, gallbladder, uterine, pancreatic and liver).
A large study examined the link between weight gain from early to middle adulthood and health outcomes later in life, following people for around 15 years. It found those who gained 2.5 to 10kg over this period had an increased incidence of type 2 diabetes, heart disease, strokes, obesity-related cancer and death compared to participants who had maintained a stable weight.
Fortunately, there are steps we can take to build lasting habits that will make weight creep a thing of the past.
7 practical steps to prevent weight creep
1. Eat from big to small
Aim to consume most of your food earlier in the day and taper your meal sizes to ensure dinner is the smallest meal you eat.
A low-calorie or small breakfast leads to increased feelings of hunger, specifically appetite for sweets, across the course of the day.
We burn the calories from a meal 2.5 times more efficiently in the morning than in the evening. So emphasising breakfast over dinner is also good for weight management.
Aim to consume bigger breakfasts and smaller dinners. Michael Burrows/Pexels 2. Use chopsticks, a teaspoon or an oyster fork
Sit at the table for dinner and use different utensils to encourage eating more slowly.
This gives your brain time to recognise and adapt to signals from your stomach telling you you’re full.
3. Eat the full rainbow
Fill your plate with vegetables and fruits of different colours first to support eating a high-fibre, nutrient-dense diet that will keep you feeling full and satisfied.
Meals also need to be balanced and include a source of protein, wholegrain carbohydrates and healthy fat to meet our dietary needs – for example, eggs on wholegrain toast with avocado.
4. Reach for nature first
Retrain your brain to rely on nature’s treats – fresh vegetables, fruit, honey, nuts and seeds. In their natural state, these foods release the same pleasure response in the brain as ultra-processed and fast foods, helping you avoid unnecessary calories, sugar, salt and unhealthy fats.
5. Choose to move
Look for ways to incorporate incidental activity into your daily routine – such as taking the stairs instead of the lift – and boost your exercise by challenging yourself to try a new activity.
Just be sure to include variety, as doing the same activities every day often results in boredom and avoidance.
Try new activities or sports to keep your interest up. Cottonbro Studio/Pexels 6. Prioritise sleep
Set yourself a goal of getting a minimum of seven hours of uninterrupted sleep each night, and help yourself achieve it by avoiding screens for an hour or two before bed.
7. Weigh yourself regularly
Getting into the habit of weighing yourself weekly is a guaranteed way to help avoid the kilos creeping up on us. Aim to weigh yourself on the same day, at the same time and in the same environment each week and use the best quality scales you can afford.
At the Boden Group, Charles Perkins Centre, we are studying the science of obesity and running clinical trials for weight loss. You can register here to express your interest.
Nick Fuller, Clinical Trials Director, Department of Endocrinology, RPA Hospital, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why are people on TikTok talking about going for a ‘fart walk’? A gastroenterologist weighs in
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Fart walks” have become a cultural phenomenon, after a woman named Mairlyn Smith posted online a now-viral video about how she and her husband go on walks about 60 minutes after dinner and release their gas.
Smith, known on TikTok as @mairlynthequeenoffibre and @mairlynsmith on Instagram, has since appeared on myriad TV and press interviews extolling the benefits of a fart walk. Countless TikTok and Instagram users and have now shared their own experiences of feeling better after taking up the #fartwalk habit.
So what’s the evidence behind the fart walk? And what’s the best way to do it?
CandyBox Images/Shutterstock Exercise can help get the gas out
We know exercise can help relieve bloating by getting gas moving and out of our bodies.
Researchers from Barcelona, Spain in 2006 asked eight patients complaining of bloating, seven of whom had irritable bowel syndrome, to avoid “gassy” foods such as beans for two days and to fast for eight hours before their study.
Each patient was asked to sit in an armchair, in order to avoid any effects of body position on the movement of gas. Gas was pumped directly into their small bowel via a thin plastic tube that went down their mouth, and the gas expelled from the body was collected into a bag via a tube placed in the rectum. This way, the researchers could determine how much gas was retained in the gut.
The patients were then asked to pedal on a modified exercise bike while remaining seated in their armchairs.
The researchers found that much less gas was retained in the patients’ gut when they exercised. They determined exercise probably helped the movement and release of intestinal gas.
Walking may have another bonus; it may trigger a nerve reflex that helps propel foods and gas contents through the gut.
Walking can also increase internal abdominal pressure as you use your abdominal muscles to stay upright and balance as you walk. This pressure on the colon helps to push intestinal gas out.
Proper fart walk technique
One study from Iran studied the effects of walking in 94 individuals with bloating.
They asked participants to carry out ten to 15 minutes of slow walking (about 1,000 steps) after eating lunch and dinner. They filled out gut symptom questionnaires before starting the program and again at the end of the four week program.
The researchers found walking after meals resulted in improvements to gut symptoms such as belching, farting, bloating and abdominal discomfort.
Now for the crucial part: in the Iranian study, there was a particular way in which participants were advised to walk. They were asked to clasp hands together behind their back and to flex their neck forward.
The clasped hands posture leads to more internal abdominal pressure and therefore more gentle squeezing out of gas from the colon. The flexed neck posture decreases the swallowing of air during walking.
This therefore is the proper fart walk technique, based on science.
Could walking with your hands behind your back yield better or more farts? candy candy/Shutterstock What about constipation?
A fart walk can help with constipation.
One study involved middle aged inactive patients with chronic constipation, who did a 12 week program of brisk walking at least 30 minutes a day – combined with 11 minutes of strength and flexibility exercises.
This program, the researchers found, improved constipation symptoms through reduced straining, less hard stools and more complete evacuation.
It also appears that the more you walk the better the benefits for gut symptoms.
In patients with irritable bowel syndrome, one study increasing the daily step count to 9,500 steps from 4,000 steps led to a 50% reduction in the severity of their symptoms.
And just 30 minutes of a fart walk has been shown to improve blood sugar levels after eating.
Walking after eating can help keep your blood sugar levels under control. IndianFaces/Shutterstock What if I can’t get outside the house?
If getting outside the house after dinner is impossible, could you try walking slowly on a treadmill or around the house for 1,000 steps?
If not, perhaps you could borrow an idea from the Barcelona research: sit back in an armchair and pedal using a modified exercise bike. Any type of exercise is better than none.
Whatever you do, don’t be a couch potato! Research has found more leisure screen time is linked to a greater risk of developing gut diseases.
We also know physical inactivity during leisure time and eating irregular meals are linked to a higher risk of abdominal pain, bloating and altered bowel motions.
Try the fart walk today
It may not be for everyone but this simple physical activity does have good evidence behind it. A fart walk can improve common symptoms such as bloating, abdominal discomfort and constipation.
It can even help lower blood sugar levels after eating.
Will you be trying a fart walk today?
Vincent Ho, Associate Professor and clinical academic gastroenterologist, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

From Dr. Oz to Heart Valves: A Tiny Device Charted a Contentious Path Through the FDA
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In 2013, the FDA approved an implantable device to treat leaky heart valves. Among its inventors was Mehmet Oz, the former television personality and former U.S. Senate candidate widely known as “Dr. Oz.”
In online videos, Oz has called the process that brought the MitraClip device to market an example of American medicine firing “on all cylinders,” and he has compared it to “landing a man on the moon.”
MitraClip was designed to spare patients from open-heart surgery by snaking hardware into the heart through a major vein. Its manufacturer, Abbott, said it offered new hope for people severely ill with a condition called mitral regurgitation and too frail to undergo surgery.
“It changed the face of cardiac medicine,” Oz said in a video.
But since MitraClip won FDA approval, versions of the device have been the subject of thousands of reports to the agency about malfunctions or patient injuries, as well as more than 1,100 reports of patient deaths, FDA records show. Products in the MitraClip line have been the subject of three recalls. A former employee has alleged in a federal lawsuit that Abbott promoted the device through illegal inducements to doctors and hospitals. The case is pending, and Abbott has denied illegally marketing the device.
The MitraClip story is, in many ways, a cautionary tale about the science, business, and regulation of medical devices.
Manufacturer-sponsored research on the device has long been questioned. In 2013, an outside adviser to the FDA compared some of the data marshaled in support of its approval to “poop.”
The FDA expanded its approval of MitraClip to a wider set of patients in 2019, based on a clinical trial in which Abbott was deeply involved and despite conflicting findings from another study.
In the three recalls, the first of which warned of potentially deadly consequences, neither the manufacturer nor the FDA withdrew inventory from the market. The company told doctors it was OK for them to continue using the recalled products.
In response to questions for this article, both Abbott and the FDA described MitraClip as safe and effective.
“With MitraClip, we’re addressing the needs of people with MR who often have no other options,” Abbott spokesperson Brent Tippen said. “Patients suffering from mitral regurgitation have severely limited quality of life. MitraClip can significantly improve survival, freedom for hospitalization and quality of life via a minimally invasive, now common procedure.”
An FDA spokesperson, Audra Harrison, said patient safety “is the FDA’s highest priority and at the forefront of our work in medical device regulation.”
She said reports to the FDA about malfunctions, injuries, and deaths that the device may have caused or contributed to are “consistent” with study results the FDA reviewed for its 2013 and 2019 approvals.
In other words: They were expected.
Inspiration in Italy
When a person has mitral regurgitation, blood flows backward through the mitral valve. Severe cases can lead to heart failure.
With MitraClip, flaps of the valve — known as “leaflets” — are clipped together at one or more points to achieve a tighter seal when they close. The clips are deployed via a catheter threaded through a major vein, typically from an incision in the groin. The procedure offers an alternative to connecting the patient to a heart-lung machine and repairing or replacing the mitral valve in open-heart surgery.
Oz has said in online videos that he got the idea after hearing a doctor describe a surgical technique for the mitral valve at a conference in Italy. “And on the way home that night, on a plane heading back to Columbia University, where I was on the faculty, I wrote the patent,” he told KFF Health News.
A patent obtained by Columbia in 2001, one of several associated with MitraClip, lists Oz first among the inventors.
But a Silicon Valley-based startup, Evalve, would develop the device. Evalve was later acquired by Abbott for about $400 million.
“I think the engineers and people at Evalve always cringe a little bit when they see Mehmet taking a lot of, you know, basically claiming responsibility for what was a really extraordinary team effort, and he was a small to almost no player in that team,” one of the company’s founders, cardiologist Fred St. Goar, told KFF Health News.
Oz did not respond to a request for comment on that statement.
As of 2019, the MitraClip device cost $30,000 per procedure, according to an article in a medical journal. According to the Abbott website, more than 200,000 people around the world have been treated with MitraClip.
Oz filed a financial disclosure during his unsuccessful run for the U.S. Senate in 2022 that showed him receiving hundreds of thousands of dollars in annual MitraClip royalties.
Abbott recently received FDA approval for TriClip, a variation of the MitraClip system for the heart’s tricuspid valve.
Endorsed ‘With Trepidation’
Before the FDA said yes to MitraClip in 2013, agency staffers pushed back.
Abbott had originally wanted the device approved for “patients with significant mitral regurgitation,” a relatively broad term. After the FDA objected, the company narrowed its proposal to patients at too-high risk for open-heart surgery.
Even then, in an analysis, the FDA identified “fundamental” flaws in Abbott’s data.
One example: The data compared MitraClip patients with patients who underwent open-heart surgery for valve repair — but the comparison might have been biased by differences in the expertise of doctors treating the two groups, the FDA analysis said. While MitraClip was implanted by a highly select, experienced group of interventional cardiologists, many of the doctors doing the open-heart surgeries had performed only a “very low volume” of such operations.
FDA “approval is not appropriate at this time as major questions of safety and effectiveness, as well as the overall benefit-risk profile for this device, remain unanswered,” the FDA said in a review prepared for a March 2013 meeting of a committee of outside advisers to the agency.
Some committee members expressed misgivings. “If your right shoe goes into horse poop and your left shoe goes into dog poop, it’s still poop,” cardiothoracic surgeon Craig Selzman said, according to a transcript.
The committee voted 5-4 against MitraClip on the question of whether it proved effective. But members voted 8-0 that they considered the device safe and 5-3 that the benefits of the device outweighed its risks.
Selzman voted yes on the last question “with trepidation,” he said at the time.
In October 2013, the FDA approved the MitraClip Clip Delivery System for a narrower group of patients: those with a particular type of mitral regurgitation who were considered a surgery risk.
“The reality is, there is no perfect procedure,” said Jason Rogers, an interventional cardiologist and University of California-Davis professor who is an Abbott consultant. The company referred KFF Health News to Rogers as an authority on MitraClip. He called MitraClip “extremely safe” and said some patients treated with it are “on death’s door to begin with.”
“At least you’re trying to do something for them,” he said.
Conflicting Studies
In 2019, the FDA expanded its approval of MitraClip to a wider set of patients.
The agency based that decision on a clinical trial in the United States and Canada that Abbott not only sponsored but also helped design and manage. It participated in site selection and data analysis, according to a September 2018 New England Journal of Medicine paper reporting the trial results. Some of the authors received consulting fees from Abbott, the paper disclosed.
A separate study in France reached a different conclusion. It found that, for some patients who fit the expanded profile, the device did not significantly reduce deaths or hospitalizations for heart failure over a year.
The French study, which appeared in the New England Journal of Medicine in August 2018, was funded by the government of France and Abbott. As with the North American study, some of the researchers disclosed they had received money from Abbott. However, the write-up in the journal said Abbott played no role in the design of the French trial, the selection of sites, or in data analysis.
Gregg Stone, one of the leaders of the North American study, said there were differences between patients enrolled in the two studies and how they were medicated. In addition, outcomes were better in the North American study in part because doctors in the U.S. and Canada had more MitraClip experience than their counterparts in France, Stone said.
Stone, a clinical trial specialist with a background in interventional cardiology, acknowledged skepticism toward studies sponsored by manufacturers.
“There are some people who say, ‘Oh, well, you know, these results may have been manipulated,’” he said. “But I can guarantee you that’s not the truth.”
‘Nationwide Scheme’
A former Abbott employee alleges in a lawsuit that after MitraClip won approval, the company promoted the device to doctors and hospitals using inducements such as free marketing support, the chance to participate in Abbott clinical trials, and payments for participating in “sham speaker programs.”
The former employee alleges that she was instructed to tell referring physicians that if they observed mitral regurgitation in their patients to “just send it” for a MitraClip procedure because “everything can be clipped.” She also alleges that, using a script, she was told to promote the device to hospital administrators based on financial advantages such as “growth opportunities through profitable procedures, ancillary tests, and referral streams.”
The inducements were part of a “nationwide scheme” of illegal kickbacks that defrauded government health insurance programs including Medicare and Medicaid, the lawsuit claims.
The company denied doing anything illegal and said in a court filing that “to help its groundbreaking therapy reach patients, Abbott needed to educate cardiologists and other healthcare providers.”
Those efforts are “not only routine, they are laudable — as physicians cannot use, or refer a patient to another doctor who can use, a device that they do not understand or in some cases even know about,” the company said in the filing.
Under federal law, the person who filed the suit can receive a share of any money the government recoups from Abbott. The suit was filed by a company associated with a former employee in Abbott’s Structural Heart Division, Lisa Knott. An attorney for the company declined to comment and said Knott had no comment.
Reports to the FDA
As doctors started using MitraClip, the FDA began receiving reports about malfunctions and cases in which the product might have caused or contributed to a death or an injury.
According to some reports, clips detached from valve flaps. Flaps became damaged. Procedures were aborted. Mitral leakage worsened. Doctors struggled to control the device. Clips became “entangled in chordae” — cord-like structures also known as heartstrings that connect the valve flaps to the heart muscle. Patients treated with MitraClip underwent corrective operations.
As of March 2024, the FDA had received more than 17,000 reports documenting more than 22,000 “events” involving mitral valve repair devices, FDA data shows. All but about 200 of those reports mention one iteration of MitraClip or another, a KFF Health News review of FDA data found.
Almost all the reports came from Abbott. The FDA requires manufacturers to submit reports when they learn of mishaps potentially related to their devices.
The reports are not proof that devices caused problems, and the same event might be reported multiple times. Other events may go unreported.
Despite the reports’ limitations, the FDA provides an analysis of them for the public on its website.
MitraClip’s risks weren’t a surprise.
Like the rapid-fire fine print in television ads for prescription drugs, the original product label for the device listed more than 60 types of potential complications.
Indeed, during clinical research on the device, about 6% of patients implanted with MitraClip died within 30 days, according to the label. Almost 1 in 4 — 23.6% – were dead within a year.
The FDA spokesperson, Harrison, pointed to a study originally published in 2021 in The Annals of Thoracic Surgery, based on a central registry of mitral valve procedures, that found lower rates of death after MitraClip went on the market.
“These data confirmed that the MitraClip device remains safe and effective in the real-world setting,” Harrison said.
But the study’s authors, several of whom disclosed financial or other connections to Abbott, said data was missing for more than a quarter of patients one year after the procedure.
A major measure of success would be the proportion of MitraClip patients who are alive “with an acceptable quality of life” a year after undergoing the procedure, the study said. Because such information was available for fewer than half of the living patients, “we have omitted those outcomes from this report,” the authors wrote.
If you’ve had an experience with MitraClip or another medical device and would like to tell KFF Health News about it, click here to share your story with us.
KFF Health News audience engagement producer Tarena Lofton contributed to this report.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: