Tempeh vs Tofu – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing tempeh to tofu, we picked the tempeh.
Why?
Per 100g, tempeh has about 1.5x as many calories, about 2x as much protein, about 3x as much fiber, and about 4x the carbohydrates.
Which latter sounds like a lot, but really, the amounts here are small—tempeh is under 12% carbohydrates, and most of that is treated by the body as fiber (e.g. it’s a resistant starch).
Both have no sugar, and both have more or less the same (tiny) amount of fat.
Micronutrients, you ask? As they’re both made from soybeans, the micronutrient profiles are similar, but exact amounts will depend on the method used, so by all means check labels if comparing products in store. By and large, there’s usually not much difference, though.
You can see sample stats here:
In summary
Both are great, and/but tempeh is the more nutrient-dense of the two.
Therefore, tempeh is the healthier option, unless you are on a very strictly calorie-controlled diet, in which case, tofu will give you more quantity per calorie.
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What are heart rate zones, and how can you incorporate them into your exercise routine?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you spend a lot of time exploring fitness content online, you might have come across the concept of heart rate zones. Heart rate zone training has become more popular in recent years partly because of the boom in wearable technology which, among other functions, allows people to easily track their heart rates.
Heart rate zones reflect different levels of intensity during aerobic exercise. They’re most often based on a percentage of your maximum heart rate, which is the highest number of beats your heart can achieve per minute.
But what are the different heart rate zones, and how can you use these zones to optimise your workout?
The three-zone model
While there are several models used to describe heart rate zones, the most common model in the scientific literature is the three-zone model, where the zones may be categorised as follows:
- zone 1: 55%–82% of maximum heart rate
- zone 2: 82%–87% of maximum heart rate
- zone 3: 87%–97% of maximum heart rate.
If you’re not sure what your maximum heart rate is, it can be calculated using this equation: 208 – (0.7 × age in years). For example, I’m 32 years old. 208 – (0.7 x 32) = 185.6, so my predicted maximum heart rate is around 186 beats per minute.
There are also other models used to describe heart rate zones, such as the five-zone model (as its name implies, this one has five distinct zones). These models largely describe the same thing and can mostly be used interchangeably.
What do the different zones involve?
The three zones are based around a person’s lactate threshold, which describes the point at which exercise intensity moves from being predominantly aerobic, to predominantly anaerobic.
Aerobic exercise uses oxygen to help our muscles keep going, ensuring we can continue for a long time without fatiguing. Anaerobic exercise, however, uses stored energy to fuel exercise. Anaerobic exercise also accrues metabolic byproducts (such as lactate) that increase fatigue, meaning we can only produce energy anaerobically for a short time.
On average your lactate threshold tends to sit around 85% of your maximum heart rate, although this varies from person to person, and can be higher in athletes.

Wearable technology has taken off in recent years. Ketut Subiyanto/Pexels In the three-zone model, each zone loosely describes one of three types of training.
Zone 1 represents high-volume, low-intensity exercise, usually performed for long periods and at an easy pace, well below lactate threshold. Examples include jogging or cycling at a gentle pace.
Zone 2 is threshold training, also known as tempo training, a moderate intensity training method performed for moderate durations, at (or around) lactate threshold. This could be running, rowing or cycling at a speed where it’s difficult to speak full sentences.
Zone 3 mostly describes methods of high-intensity interval training, which are performed for shorter durations and at intensities above lactate threshold. For example, any circuit style workout that has you exercising hard for 30 seconds then resting for 30 seconds would be zone 3.
Striking a balance
To maximise endurance performance, you need to strike a balance between doing enough training to elicit positive changes, while avoiding over-training, injury and burnout.
While zone 3 is thought to produce the largest improvements in maximal oxygen uptake – one of the best predictors of endurance performance and overall health – it’s also the most tiring. This means you can only perform so much of it before it becomes too much.
Training in different heart rate zones improves slightly different physiological qualities, and so by spending time in each zone, you ensure a variety of benefits for performance and health.
So how much time should you spend in each zone?
Most elite endurance athletes, including runners, rowers, and even cross-country skiers, tend to spend most of their training (around 80%) in zone 1, with the rest split between zones 2 and 3.
Because elite endurance athletes train a lot, most of it needs to be in zone 1, otherwise they risk injury and burnout. For example, some runners accumulate more than 250 kilometres per week, which would be impossible to recover from if it was all performed in zone 2 or 3.
Of course, most people are not professional athletes. The World Health Organization recommends adults aim for 150–300 minutes of moderate intensity exercise per week, or 75–150 minutes of vigorous exercise per week.
If you look at this in the context of heart rate zones, you could consider zone 1 training as moderate intensity, and zones 2 and 3 as vigorous. Then, you can use heart rate zones to make sure you’re exercising to meet these guidelines.
What if I don’t have a heart rate monitor?
If you don’t have access to a heart rate tracker, that doesn’t mean you can’t use heart rate zones to guide your training.
The three heart rate zones discussed in this article can also be prescribed based on feel using a simple 10-point scale, where 0 indicates no effort, and 10 indicates the maximum amount of effort you can produce.
With this system, zone 1 aligns with a 4 or less out of 10, zone 2 with 4.5 to 6.5 out of 10, and zone 3 as a 7 or higher out of 10.
Heart rate zones are not a perfect measure of exercise intensity, but can be a useful tool. And if you don’t want to worry about heart rate zones at all, that’s also fine. The most important thing is to simply get moving.
Hunter Bennett, Lecturer in Exercise Science, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Women want to see the same health provider during pregnancy, birth and beyond
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hazel Keedle, Western Sydney University and Hannah Dahlen, Western Sydney University
In theory, pregnant women in Australia can choose the type of health provider they see during pregnancy, labour and after they give birth. But this is often dependent on where you live and how much you can afford in out-of-pocket costs.
While standard public hospital care is the most common in Australia, accounting for 40.9% of births, the other main options are:
- GP shared care, where the woman sees her GP for some appointments (15% of births)
- midwifery continuity of care in the public system, often called midwifery group practice or caseload care, where the woman sees the same midwife of team of midwives (14%)
- private obstetrician care (10.6%)
- private midwifery care (1.9%).
Given the choice, which model would women prefer?
Our new research, published BMC Pregnancy and Childbirth, found women favoured seeing the same health provider throughout pregnancy, in labour and after they have their baby – whether that’s via midwifery group practice, a private midwife or a private obstetrician.
Assessing strengths and limitations
We surveyed 8,804 Australian women for the Birth Experience Study (BESt) and 2,909 provided additional comments about their model of maternity care. The respondents were representative of state and territory population breakdowns, however fewer respondents were First Nations or from culturally or linguistically diverse backgrounds.
We analysed these comments in six categories – standard maternity care, high-risk maternity care, GP shared care, midwifery group practice, private obstetric care and private midwifery care – based on the perceived strengths and limitations for each model of care.
Overall, we found models of care that were fragmented and didn’t provide continuity through the pregnancy, birth and postnatal period (standard care, high risk care and GP shared care) were more likely to be described negatively, with more comments about limitations than strengths.
What women thought of standard maternity care in hospitals
Women who experienced standard maternity care, where they saw many different health care providers, were disappointed about having to retell their story at every appointment and said they would have preferred continuity of midwifery care.
Positive comments about this model of care were often about a midwife or doctor who went above and beyond and gave extra care within the constraints of a fragmented system.
The model of care with the highest number of comments about limitations was high-risk maternity care. For women with pregnancy complications who have their baby in the public system, this means seeing different doctors on different days.
Some respondents received conflicting advice from different doctors, and said the focus was on their complications instead of their pregnancy journey. One woman in high-risk care noted:
The experience was very impersonal, their focus was my cervix, not preparing me for birth.
Why women favoured continuity of care
Overall, there were more positive comments about models of care that provided continuity of care: private midwifery care, private obstetric care and midwifery group practice in public hospitals.
Women recognised the benefits of continuity and how this included informed decision-making and supported their choices.
The model of care with the highest number of positive comments was care from a privately practising midwife. Women felt they received the “gold standard of maternity care” when they had this model. One woman described her care as:
Extremely personable! Home visits were like having tea with a friend but very professional. Her knowledge and empathy made me feel safe and protected. She respected all of my decisions. She reminded me often that I didn’t need her help when it came to birthing my child, but she was there if I wanted it (or did need it).
However, this is a private model of care and women need to pay for it. So there are barriers in accessing this model of care due to the cost and the small numbers working in Australia, particularly in regional, rural and remote areas, among other barriers.
Women who had private obstetricians were also positive about their care, especially among women with medical or pregnancy complications – this type of care had the second-highest number of positive comments.
This was followed by women who had continuity of care from midwives in the public system, which was described as respectful and supportive.
However, one of the limitations about continuity models of care is when the woman doesn’t feel connected to her midwife or doctor. Some women who experienced this wished they had the opportunity to choose a different midwife or doctor.
What about shared care with a GP?
While shared care between the GP and hospital model of care is widely promoted in the public maternity care system as providing continuity, it had a similar number of negative comments to those who had fragmented standard hospital care.
Considering there is strong evidence about the benefits of midwifery continuity of care, and this model of care appears to be most acceptable to women, it’s time to expand access so all Australian women can access continuity of care, regardless of their location or ability to pay.
Hazel Keedle, Senior Lecturer of Midwifery, Western Sydney University and Hannah Dahlen, Professor of Midwifery, Associate Dean Research and HDR, Midwifery Discipline Leader, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Collard Greens vs Kale – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing collard greens to kale, we picked the collard greens.
Why?
Once again we have Brassica oleracea vs Brassica oleracea, (the same species that is also broccoli, cauliflower, Brussels sprouts, various kinds of cabbage, and more) and once again there are nutritional differences between the two cultivars:
In terms of macros, collard greens have more protein, equal carbs, and 2x the fiber. So that’s a win for collard greens.
In the category of vitamins, collard greens have more of vitamins B2, B3, B5, B9, E, and choline, while kale has more of vitamins A, B1, B6, C, and K. Nominally a 6:5 win for collard greens, though it’s worth noting that while most of the margins of difference are about the same, collard greens have more than 10x the choline, too.
When it comes to minerals, collard greens have more calcium, iron, magnesium, manganese, and phosphorus, while kale has more copper, potassium, selenium, and zinc. A genuinely marginal 5:4 win for collard greens this time.
All in all, a clear win for collard greens over the (otherwise rightly) established superfood kale. Collard greens just don’t get enough appreciation in comparison!
Want to learn more?
You might like to read:
What’s Your Plant Diversity Score? ← another reason it’s good to mix things up rather than just using the same ingredients out of habit!
Take care!
Share This Post

Related Posts
-
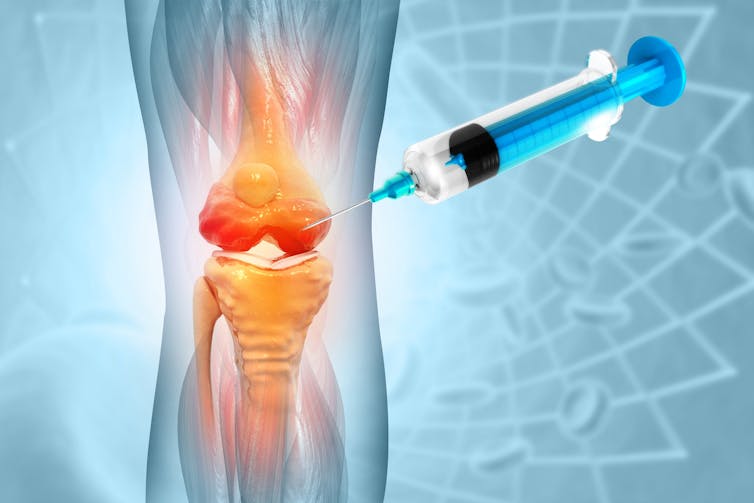
People are getting costly stem cell injections for knee osteoarthritis. But we don’t know if they work
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
More than 500 million people around the world live with osteoarthritis. The knee is affected more often than any other joint, with symptoms (such as pain, stiffness and reduced movement) affecting work, sleep, sport and daily activities.
Knee osteoarthritis is often thought of as thinning of the protective layer of cartilage within the joint. But we now understand it affects all the structures of the joint, including the bones, muscles and nerve endings.
While there are things that can be done to manage the symptoms of knee osteoarthritis, there is no cure, and many people experience persistent pain. As a result, an opportunity exists for as yet unproven treatments to enter the market, often before regulatory safeguards can be put in place.
Stem cell injections are one such treatment. A new review my colleagues and I published this week finds that evidence of their benefits and harms remains elusive.
Marinesea/Shutterstock Stem cell treatments
Stem cells are already established as treatments for some diseases – mostly disorders of the blood, bone marrow or immune system – which has led to suggestions they could be used for a much wider array of conditions.
Stem cells have been touted as promising treatments for osteoarthritis because they have special properties which allow them to replicate and develop into the mature healthy cells that make up our body’s organs and other tissues, including cartilage.
Stem cell treatments for osteoarthritis generally involve taking a sample of tissue from a site that is rich in stem cells (such as bone marrow or fat), treating it to increase the number of stem cells, then injecting it into the joint.
The hope is that if the right type of stem cells can be introduced into an osteoarthritic joint in the right way and at the right time, they may help to repair damaged structures in the joint, or have other effects such as reducing inflammation.
But no matter how convincing the theory, we need good evidence for effectiveness and safety before a new therapy is adopted into practice.
Stem cells have been touted as promising treatments for osteoarthritis. But what does the evidence say? crystal light/Shutterstock Stem cell injections have not been approved by Australia’s Therapeutic Goods Administration for the treatment of osteoarthritis. Nonetheless, some clinics in Australia and around the world still offer them.
Because of the regulatory restrictions, we don’t have reliable numbers on how many procedures are being done.
They’re not covered by Medicare, so the procedure can cost the consumer thousands of dollars.
And, as with any invasive procedure, both the harvest of stem cells and the joint injection procedure may carry the potential for harm, such as infection.
What we found
Our new review, published by the independent, international group the Cochrane Collaboration, looks at all 25 randomised trials of stem cell injections for knee osteoarthritis that have been conducted worldwide to date. Collectively, these studies involved 1,341 participants.
We found stem cell injections may slightly improve pain and function compared with a placebo injection, but the size of the improvement may be too small for the patient to notice.
The evidence isn’t strong enough to determine whether there is any improvement in quality of life following a stem cell injection, whether cartilage regrows, or to estimate the risk of harm.
This means we can’t confidently say yet whether any improvement that might follow a stem cell injection is worth the risk (or the cost).
Osteoarthritis of the knee is the most common type of osteoarthritis. michaelheim/Shutterstock Hope or hype?
It’s not surprising we invest hope in finding a transformative treatment for such a common and disabling condition. Belief in the benefits of stem cells is widespread – more than three-quarters of Americans believe stem cells can relieve arthritis pain and more than half believe this treatment to be curative.
But what happens if a new treatment is introduced to practice before it has been clearly proven to be safe and effective?
The use of an unproven, invasive therapy is not just associated with the risks of the intervention itself. Even if the treatment were harmless, there is the risk of unnecessary cost, inconvenience, and a missed opportunity for the patient to use existing therapies that are known to be effective.
What’s more, if we need to play catch-up to try to establish an evidence base for a treatment that’s already in practice, we risk diverting scarce research resources towards a therapy that may not prove to be effective, simply because the genie is out of the bottle.
There are some ways to manage the symptoms of knee osteoarthritis. PeopleImages.com – Yuri A/Shutterstock Working towards a clearer answer
Several more large clinical trials are currently underway, and should increase our understanding of whether stem cell injections are safe and effective for knee osteoarthritis.
Our review incorporates “living evidence”. This means we will continue to add the results of new trials as soon as they’re published, so the review is always up to date, and offers a comprehensive and trustworthy summary to help people with osteoarthritis and their health-care providers to make informed decisions.
In the meantime, there are a number of evidence-based treatment options. Non-drug treatments such as physiotherapy, regular exercise, maintaining a healthy weight, and cognitive behavioural therapy can be more effective than you think. Anti-inflammatory and pain medications can also play a supporting role.
Importantly, it’s not inevitable that osteoarthritic joints get worse with time. So, even though joint replacement surgery is often highly effective, it’s the last resort and fortunately, many people never need to take this step.
Samuel Whittle, ANZMUSC Practitioner Fellow, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Gut Renovation – by Dr. Roshini Raj, with Sheila Buff
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Unless we actually feel something going on down there, gut health is an oft-neglected part of overall health—which is unfortunate, because invisible as it may often be, it affects so much.
Gastroenterologist Dr. Roshini Raj gives us all the need-to-know information, explanations of why things happen the way they do with regard to the gut, and tips, tricks, and hacks to improve matters.
She also does some mythbusting along the way, and advises about what things don’t make a huge difference, including what medications don’t have a lot of evidence for their usefulness.
The style is easy-reading pop-science, with plenty of high-quality medical content.
Reading between the lines, a lot of the book as it stands was probably written by the co-author, Sheila Buff, who is a professional ghostwriter and specializes in working closely with doctors to produce works that are readable and informative to the layperson while still being full of the doctor’s knowledge and expertise. So a reasonable scenario is that Dr. Raj gave her extensive notes, she took it from there, passed it back to her for medical corrections, and they had a little back and forth until it was done. Whatever their setup, the end result was definitely good!
Bottom line: if you’d like a guide to gut health that’s practical and easy to read, while being quite comprehensive and certainly a lot more than “eat probiotics and fiber”, then this book is a fine choice.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Why Belly Fat Is The Last To Go (& 3 Signs You’re Nearly There)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cori Lefkowitz, of “Strong At Every Age” advises:
See the signs
It’s usually the last place to shrink, even though it’s the first place we want; it doesn’t help that most people quit too early or obsess over the scale, which can sabotage progress.
Three mistakes to avoid:
- Unduly focusing on calories: not only are listed caloric values often misleading, calorie-counting typically leads to restriction, fatigue, and rebound weight gain, none of which are good. Instead, track macros to keep your metabolism ticking over nicely, build/maintain muscle, and make what you’re doing sustainable.
- Prioritizing hard work over intentional work: random hard workouts and extreme restrictions will ultimately burn you out. Instead, every action should serve a clear purpose towards your goals, so do make a point of planning ahead from time to time (e.g. each month, make a plan, follow it, and then review your progress to plan again for the next month).
- Not following a workout progression: stringing random moves together won’t normally build lean muscle. Instead, she advises to repeat a structured plan for 3–6 weeks, progressively challenge yourself, measure results, and repeat until you’ve got to where you want to be.
Three signs you’re nearly there:
- Seeing more definition in other body parts: fat often comes off first from areas we don’t care about; this can even make the belly look bigger temporarily, but it’s actually progress!
- Clothes fitting more loosely: even without scale changes, fat loss and recomposition show up in how clothing fits over time.
- Improvements in performance, sleep, and health: stronger workouts, better energy, and healthier markers mean your body is functioning better and supporting fat loss.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Can You Shrink A Waist In Seven Days?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: