The Midlife Cyclist – by Phil Cavell
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Whether stationary cycling in your living room, or competing in the Tour de France, there’s a lot more to cycling than “push the pedals”—if you want to get good benefits and avoid injury, in any case.
This book explores the benefits of different kinds of cycling, the biomechanics of various body positions, and the physiology of different kinds of performance, and the impact these things have on everything from your joints to your heart to your telomeres.
The style is very much conversational, with science included, and a readiness to acknowledge in cases where the author is guessing or going with a hunch, rather than something being well-evidenced. This kind of honesty is always good to see, and it doesn’t detract from where the science is available and clear.
One downside for some readers will be that while Cavell does endeavour to cover sex differences in various aspects of how they relate to the anatomy and physiology (mostly: the physiology) of cycling, the book is written from a male perspective and the author clearly understands that side of things better. For other readers, of course, this will be a plus.
Bottom line: if you enjoy cycling, or you’re thinking of taking it up but it seems a bit daunting because what if you do it wrong and need a knee replacement in a few years or what if you hurt your spine or something, then this is the book to set your mind at ease, and put you on the right track.
Click here to check out The Midlife Cyclist, and enjoy the cycle of life!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

From Strength to Strength – by Dr. Arthur Brooks

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For most professions, there are ways in which performance can be measured, and the average professional peak varies by profession, but averages are usually somewhere in the 30–45 range, with a pressure to peak between 25–35.
With a peak by age 45 or perhaps 50 at the latest (aside from some statistical outliers, of course), what then to expect at age 50+? Not long after that, there’s a reason for mandatory retirement ages in some professions.
Dr. Brooks examines the case for accepting that rather than fighting it, and/but making our weaknesses into our strengths as we go. If our fluid intelligence slows, our accumulated crystal intelligence (some might call it “wisdom“) can make up for it, for example.
But he also champions the idea of looking outside of ourselves; of the importance of growing and fostering connections; giving to those around us and receiving support in turn; not transactionally, but just as a matter of mutualism of the kind found in many other species besides our own. Indeed, Dr. Brooks gives the example of a grove of aspen trees (hence the cover art of this book) that do exactly that.
The style is very accessible in terms of language but with frequent scientific references, so very much a “best of both worlds” in terms of readability and information-density.
Bottom line: if ever you’ve wondered at what age you might outlive your usefulness, this book will do as the subtitle suggests, and help you carve out your new place.
Click here to check out From Strength To Strength, and find yours!
Share This Post
-

Continuous Glucose Monitors Without Diabetes: Pros & Cons
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The “Glucose Goddess”, biochemist Jessie Inchauspé, gives us the low-down:
Knowledge is power (but watch out)
A continuous glucose monitor (CGM) is a device that continually monitors glucose levels, without the need to stab one’s finger every few hours to test blood.
It was designed for diabetics, especially for those with Type 1 Diabetes, where around-the-clock monitoring is necessary for appropriate insulin dosing.
For non-diabetics, they can be a good way of learning what our body’s response to various foods and activities is like, the better to be able to tweak our habits to avoid undue glucose spikes (which are harmful for our pancreas, liver, heart, brain, kidneys, and more).
How it works: there’s a sensor that sits on the arm (or elsewhere, but the arm is a popular placement) with a little probe that goes under the skin. It’s applied using a device that inserts it automatically using a needle (you only need to press a button, you don’t need to guide the needle yourself); the needle then retracts, leaving the soft, flexible probe in place. Having been attached, that sensor can now stay in place for 2 weeks (usually; depends on brand, but for example FreeStyle Libre, the most popular brand, the sensors last 2 weeks), and yes, it’s fine to bathe/shower/etc with it. When you want an update from your CGM, you scan it with your phone (or you can buy a dedicated reader, but that is more expensive and unnecessary), and it uploads the data since your last scan.
Pros: it’s convenient and gives a lot of data, so even if you only use it for a short period of time (for example, a month) you can get a very good idea of what affects your blood sugar levels and how. Also, because of the constant nature of the monitoring, it helps avoid accidental sample bias of the kind that can occur with manual testing, by testing a little too soon or too late, and missing a spike/dip.
Cons: it can be expensive, depending on where you live and what options are available for you locally, so you might not want to do it long-term (since that would require buying two sensors per month). It’s also, for all its wealth of data, slightly less accurate than fingerprick testing—that’s because it takes an interstitial reading instead of directly from the blood. For this reason, if you test both ways, you may find a discrepancy of about 3mg/dL. Given that the healthy range is about 70–140mg/dL, a discrepancy of 3mg/dL is probably not going to be important, but it is a thing to mention can (and probably will) happen.
Patterns to bear in mind (with any kind of blood sugar monitoring):
- Dawn phenomenon: a natural glucose rise upon waking.
- Exercise-induced spikes (normal due to energy demands).
- Fat in meals slowing glucose absorption.
- Different foods can sometimes cause a double-wave after dinner (because glucose from different foods is absorbed differently, and/or different foods affect insulin response independent of glucose)
- Steep, rapid spikes that are more harmful than gradual, sustained increases.
- Vitamin C spikes: temporary chemical interference with the sensor, not actual glucose rises.
- Nighttime glucose dips (often false readings caused by sleeping position).
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
10 Ways To Balance Blood Sugars
Take care!
Share This Post
-

Do We Need Supplements, And Do They Work?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Does our diet need a little help?

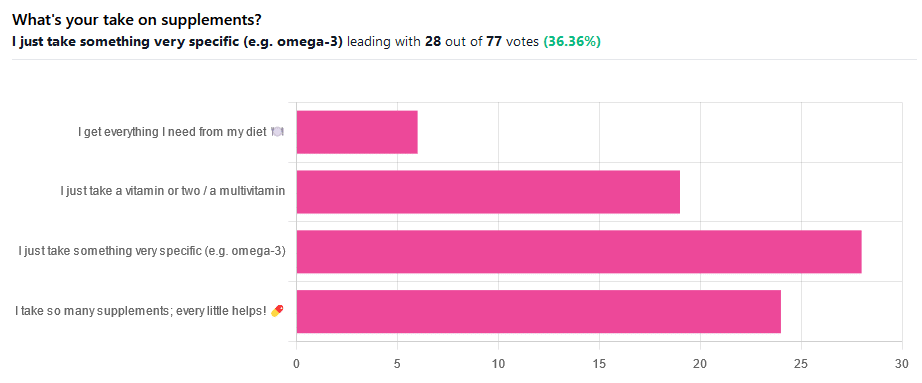
We asked you for your take on supplements, and got the above-illustrated, below-described set of results.
- The largest minority of respondents (a little over a third) voted for “I just take something very specific”
- The next most respondents voted for “I take so many supplements; every little helps!”
- Almost as many voted for “I just take a vitamin or two / a multivitamin”
- Fewest, about 8%, voted for “I get everything I need from my diet”
But what does the science say?
Food is less nutritious now than it used to be: True or False?
True or False depending on how you measure it.
An apple today and an apple from a hundred years ago are likely to contain the same amounts of micronutrients per apple, but a lower percentage of micronutrients per 100g of apple.
The reason for this is that apples (and many other food products; apples are just an arbitrary example) have been selectively bred (and in some cases, modified) for size, and because the soil mineral density has remained the same, the micronutrients per apple have not increased commensurate to the increase in carbohydrate weight and/or water weight. Thus, the resultant percentage will be lower, despite the quantity remaining the same.
We’re going to share some science on this, and/but would like to forewarn readers that the language of this paper is a bit biased, as it looks to “debunk” claims of nutritional values dropping while skimming over “yes, they really have dropped percentage-wise” in favor of “but look, the discrete mass values are still the same, so that’s just a mathematical illusion”.
The reality is, it’s no more a mathematical illusion than is the converse standpoint of saying the nutritional value is the same, despite the per-100g values dropping. After all, sometimes we eat an apple as-is; sometimes we buy a bag of frozen chopped fruit. That 500g bag of chopped fruit is going to contain less copper (for example) than one from decades past.
Here’s the paper, and you’ll see what we mean:
Supplements aren’t absorbed properly and thus are a waste of money: True or False?
True or False depending on the supplement (and your body, and the rest of your diet)
Many people are suffering from dietary deficiencies of vitamins and minerals, that could be easily correctable by supplementation:

However, as this study by Dr. Fang Fang Zhang shows, a lot of vitamin and mineral supplementation does not appear to have much of an effect on actual health outcomes, vis-à-vis specific diseases. She looks at:
- Cardiovascular disease
- Cancer
- Type 2 diabetes
- Osteoporosis
Her key take-aways from this study were:
- Randomised trial evidence does not support use of vitamin, mineral, and fish oil supplements to reduce the risk of non-communicable diseases
- People using supplements tend to be older, female, and have higher education, income, and healthier lifestyles than people who do not use them
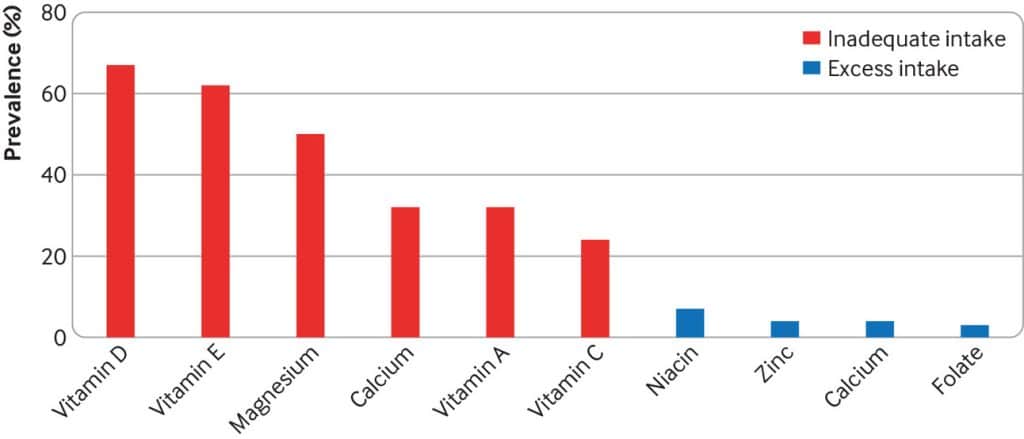
- Use of supplements appreciably reduces the prevalence of inadequate intake for most nutrients but also increases the prevalence of excess intake for some nutrients
- Further research is needed to assess the long term effects of supplements on the health of the general population and in individuals with specific nutritional needs, including those from low and middle income countries
Read her damning report: Health effects of vitamin and mineral supplements
On the other hand…
This is almost entirely about blanket vitamin-and-mineral supplementation. With regard to fish oil supplementation, many commercial fish oil supplements break down in the stomach rather than the intestines, and don’t get absorbed well. Additionally, many people take them in forms that aren’t pleasant, and thus result in low adherence (i.e., they nominally take them, but in fact they just sit on the kitchen counter for a year).
One thing we can conclude from this is that it’s good to check the science for any given supplement before taking it, and know what it will and won’t help for. Our “Monday Research Review” editions of 10almonds do this a lot, although we tend to focus on herbal supplements rather than vitamins and minerals.
We can get everything we need from our diet: True or False?
Contingently True (but here be caveats)
In principle, if we eat the recommended guideline amounts of various macro- and micro-nutrients, we will indeed get all that we are generally considered to need. Obviously.
However, this may come with:
- Make sure to get enough protein… Without too much meat, and also without too much carbohydrate, such as from most plant sources of protein
- Make sure to get enough carbohydrates… But only the right kinds, and not too much, nor at the wrong time, and without eating things in the wrong order
- Make sure to get enough healthy fats… Without too much of the unhealthy fats that often exist in the same foods
- Make sure to get the right amount of vitamins and minerals… We hope you have your calculators out to get the delicate balance of calcium, magnesium, potassium, phosphorus, and vitamin D right.
That last one’s a real pain, by the way. Too much or too little of one or another and the whole set start causing problems, and several of them interact with several others, and/or compete for resources, and/or are needed for the others to do their job.
And, that’s hard enough to balance when you’re taking supplements with the mg/µg amount written on them, never mind when you’re juggling cabbages and sardines.
On the topic of those sardines, don’t forget to carefully balance your omega-3, -6, and -9, and even within omega-3, balancing ALA, EPA, and DHA, and we hope you’re juggling those HDL and LDL levels too.
So, when it comes to getting everything we need from our diet, for most of us (who aren’t living in food deserts and/or experiencing food poverty, or having a medical condition that restricts our diet), the biggest task is not “getting enough”, it’s “getting enough of the right things without simultaneously overdoing it on the others”.
With supplements, it’s a lot easier to control what we’re putting in our bodies.
And of course, unless our diet includes things that usually can’t be bought in supermarkets, we’re not going to get the benefits of taking, as a supplement, such things as:
Etc.
So, there definitely are supplements with strong science-backed benefits, that probably can’t be found on your plate!
Share This Post
Related Posts
-
What’s the difference between period pain and endometriosis pain?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Menstruation, or a period, is the bleeding that occurs about monthly in healthy people born with a uterus, from puberty to menopause. This happens when the endometrium, the tissue that lines the inside of the uterus, is shed.
Endometriosis is a condition that occurs when endometrium-like tissue is found outside the uterus, usually within the pelvic cavity. It is often considered a major cause of pelvic pain.
Pelvic pain significantly impacts quality of life. But how can you tell the difference between period pain and endometriosis?

Polina Zimmerman/Pexels Periods and period pain
Periods involve shedding the 4-6 millimetre-thick endometrial lining from the inside of the uterus.
As the lining detaches from the wall of the uterus, the blood vessels which previously supplied the lining bleed. The uterine muscles contract, expelling the blood and crumbled endometrium.
The crumbled endometrium and blood mostly pass through the cervix and vagina. But almost everyone back-bleeds via their fallopian tubes into their pelvic cavity. This is known as “retrograde menstruation”.
Most of the lining is shed through the vagina. Andrey_Popov/Shutterstock The process of menstrual shedding is caused by inflammatory substances, which also cause nausea, vomiting, diarrhoea, headaches, aches, pains, dizziness, feeling faint, as well as stimulating pain receptors.
These inflammatory substances are responsible for the pain and symptoms in the week before a period and the first few days.
For women with heavy periods, their worst days of pain are usually the heaviest days of their period, coinciding with more cramps to expel clots and more retrograde bleeding.
Many women also have pain when they are releasing an egg from their ovary at the time of ovulation. Ovulation or mid-cycle pain can be worse in those who bleed more, as those women are more likely to bleed into the ovulation follicle.
Around 90% of adolescents experience period pain. Among these adolescents, 20% will experience such severe period pain they need time off from school and miss activities. These symptoms are too often normalised, without validation or acknowledgement.
What about endometriosis?
Many symptoms have been attributed to endometriosis, including painful periods, pain with sex, bladder and bowel-related pain, low back pain and thigh pain.
Other pain-related conditions such migraines and chronic fatigue have also been linked to endometriosis. But these other pain-related symptoms occur equally often in people with pelvic pain who don’t have endometriosis.
One in five adolescents who menstrate experience severe symptoms. CGN089/Shutterstock Repeated, significant period and ovulation pain can eventually lead some people to develop persistent or chronic pelvic pain, which lasts longer than six months. This appears to occur through a process known as central sensitisation, where the brain becomes more sensitive to pain and other sensory stimuli.
Central sensitisation can occur in people with persistent pain, independent of the presence or absence of endometriosis.
Eventually, many people with period and/or persistent pelvic pain will have an operation called a laparoscopy, which allows surgeons to examine organs in the pelvis and abdomen, and diagnose and treat endometriosis.
Yet only 50% of those with identical pain symptoms who undergo a laparoscopy will end up having endometriosis.
Endometriosis is also found in pain-free women. So we cannot predict who does and doesn’t have endometriosis from symptoms alone.
How is this pain managed?
Endometriosis surgery usually involves removing lesions and adhesions. But at least 30% of people return to pre-surgery pain levels within six months or have more pain than before.
After surgery, emergency department presentations for pain are unchanged and 50% have repeat surgery within a few years.
Suppressing periods using hormonal therapies (such as continuous oral contraceptive pills or progesterone-only approaches) can suppress endometriosis and reduce or eliminate pain, independent of the presence or absence of endometriosis.
Not every type or dose of hormonal medications suits everyone, so medications need to be individualised.
The current gold-standard approach to manage persistent pelvic pain involves a multidisciplinary team approach, with the aim of achieving sustained remission and improving quality of life. This may include:
- physiotherapy for pelvic floor and other musculoskeletal problems
- management of bladder and bowel symptoms
- support for self-managing pain
- lifestyle changes including diet and exercise
- psychological or group therapy, as our moods, stress levels and childhood events can affect how we feel and experience pain.
Whether you have period pain, chronic pelvic pain or pain you think is associated with endometriosis, if you feel pain, it’s real. If it’s disrupting your life, you deserve to be taken seriously and treated as the whole person you are.
Sonia R. Grover, Senior Research Fellow, Murdoch Children’s Research Institute; Clinical Professor of Gynaecology, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

I’ve been diagnosed with cancer. How do I tell my children?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
With around one in 50 adults diagnosed with cancer each year, many people are faced with the difficult task of sharing the news of their diagnosis with their loved ones. Parents with cancer may be most worried about telling their children.
It’s best to give children factual and age-appropriate information, so children don’t create their own explanations or blame themselves. Over time, supportive family relationships and open communication help children adjust to their parent’s diagnosis and treatment.
It’s natural to feel you don’t have the skills or knowledge to talk with your children about cancer. But preparing for the conversation can improve your confidence.
Benjamin Manley/Unsplash Preparing for the conversation
Choose a suitable time and location in a place where your children feel comfortable. Turn off distractions such as screens and phones.
For teenagers, who can find face-to-face conversations confronting, think about talking while you are going for a walk.
Consider if you will tell all children at once or separately. Will you be the only adult present, or will having another adult close to your child be helpful? Another adult might give your children a person they can talk to later, especially to answer questions they might be worried about asking you.
Choose the time and location when your children feel comfortable. Craig Adderley/Pexels Finally, plan what to do after the conversation, like doing an activity with them that they enjoy. Older children and teenagers might want some time alone to digest the news, but you can suggest things you know they like to do to relax.
Also consider what you might need to support yourself.
Preparing the words
Parents might be worried about the best words or language to use to make sure the explanations are at a level their child understands. Make a plan for what you will say and take notes to stay on track.
The toughest part is likely to be saying to your children that you have cancer. It can help to practise saying those words out aloud.
Ask family and friends for their feedback on what you want to say. Make use of guides by the Cancer Council, which provide age-appropriate wording for explaining medical terms like “cancer”, “chemotherapy” and “tumour”.
Having the conversation
Being open, honest and factual is important. Consider the balance between being too vague, and providing too much information. The amount and type of information you give will be based on their age and previous experiences with illness.
Remember, if things don’t go as planned, you can always try again later.
Start by telling your children the news in a few short sentences, describing what you know about the diagnosis in language suitable for their age. Generally, this information will include the name of the cancer, the area of the body affected and what will be involved in treatment.
Let them know what to expect in the coming weeks and months. Balance hope with reality. For example:
The doctors will do everything they can to help me get well. But, it is going to be a long road and the treatments will make me quite sick.
Check what your child knows about cancer. Young children may not know much about cancer, while primary school-aged children are starting to understand that it is a serious illness. Young children may worry about becoming unwell themselves, or other loved ones becoming sick.
Young children might worry about other loved ones becoming sick. Pixabay/Pexels Older children and teenagers may have experiences with cancer through other family members, friends at school or social media.
This process allows you to correct any misconceptions and provides opportunities for them to ask questions. Regardless of their level of knowledge, it is important to reassure them that the cancer is not their fault.
Ask them if there is anything they want to know or say. Talk to them about what will stay the same as well as what may change. For example:
You can still do gymnastics, but sometimes Kate’s mum will have to pick you up if I am having treatment.
If you can’t answer their questions, be OK with saying “I’m not sure”, or “I will try to find out”.
Finally, tell children you love them and offer them comfort.
How might they respond?
Be prepared for a range of different responses. Some might be distressed and cry, others might be angry, and some might not seem upset at all. This might be due to shock, or a sign they need time to process the news. It also might mean they are trying to be brave because they don’t want to upset you.
Children’s reactions will change over time as they come to terms with the news and process the information. They might seem like they are happy and coping well, then be teary and clingy, or angry and irritable.
Older children and teenagers may ask if they can tell their friends and family about what is happening. It may be useful to come together as a family to discuss how to inform friends and family.
What’s next?
Consider the conversation the first of many ongoing discussions. Let children know they can talk to you and ask questions.
Resources might also help; for example, The Cancer Council’s app for children and teenagers and Redkite’s library of free books for families affected by cancer.
If you or other adults involved in the children’s lives are concerned about how they are coping, speak to your GP or treating specialist about options for psychological support.
Cassy Dittman, Senior Lecturer/Head of Course (Undergraduate Psychology), Research Fellow, Manna Institute, CQUniversity Australia; Govind Krishnamoorthy, Senior Lecturer, School of Psychology and Wellbeing, Post Doctoral Fellow, Manna Institute, University of Southern Queensland, and Marg Rogers, Senior Lecturer, Early Childhood Education; Post Doctoral Fellow, Manna Institute, University of New England
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Podiatrists Debunk 11 Feet Myths
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Podiatrists Dr. Sarah Haller and Dr. Brad Schaeffer put us on a better path:
Don’t get wrong-footed
We’ll not keep the 11 myths a mystery; they are…
- “You have warts because your feet are dirty.”
False! Warts are caused by a virus, not dirt. Viruses can be picked up from surfaces like yoga mats, pools, gyms, and showers. - “Bunions are caused by wearing heels.”
False! Bunions are genetic deformities where the bone behind the big toe shifts. Heels might worsen them but don’t cause them. - “Cutting the sides of my toenail will prevent an ingrown toenail.”
False! Toenails should be cut straight across. Cutting the sides can make ingrown toenails worse. - “Pedicures gave me toenail fungus.”
Partially true! You can get fungus from many places, but safe, sterile pedicures are generally fine. - “Only athletes get athlete’s foot.”
False! Athlete’s foot is a fungal infection caused by warm, moist environments. Anyone can get it, not just athletes. - “My feet are fine because I trained them to walk in stilettos.”
False! You can get used to stilettos, but they aren’t healthy long-term. They shorten the Achilles tendon and put pressure on the foot. - “You can’t do anything for a broken toe.”
False! Broken toes can be treated and should be checked by a doctor. They may need to be set for proper healing. - “It’s normal for your feet to hurt from standing all day.”
False! Foot pain isn’t normal and can be prevented with proper footwear, support, and compression socks. - “All inserts are the same.”
False! Everyone’s feet are different. Some may benefit from over-the-counter insoles, but others need custom orthotics. - “Sprained ankles are no big deal.”
False! Sprains can damage ligaments and lead to instability or arthritis if untreated. Proper stabilization is essential. - “If I can walk after an injury, I don’t need to see a doctor.”
False! You can still have serious injuries like fractures even if you can walk. Always get checked after an injury.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Steps For Keeping Your Feet A Healthy Foundation
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- “You have warts because your feet are dirty.”