The Menopause Brain – by Dr. Lisa Mosconi
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
With her PhD in neuroscience and nuclear medicine (a branch of radiology, used for certain types of brain scans, amongst other purposes), whereas many authors will mention “brain fog” as a symptom of menopause, Dr. Mosconi can (and will) point to a shadowy patch on a brain scan and say “that’s the brain fog, there”.
And so on for many other symptoms of menopause that are commonly dismissed as “all in your head”, notwithstanding that “in your head” is the worst place for a problem to be. You keep almost your entire self in there!
Dr. Mosconi covers how hormones influence not just our moods in a superficial way, but also change the structure of our brain over time.
Importantly, she also gives an outline of how to stay on the ball; what things to watch out for when your doctor probably won’t, and what things to ask for when your doctor probably won’t suggest them.
Bottom line: if menopause is a thing in your life (or honestly, even if it isn’t but you are running on estrogen rather than testosterone), then this is a book for you.
Click here to check out The Menopause Brain, and look after yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Menopause: 50 Things You Need to Know – by Dr. Felice Gersh

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Can you list 50 important facts about the menopause? If not, you’ll surely find things to learn in here.
The book is divided into three main sections:
- What to expect in perimenopause
- What to expect in early menopause
- What to expect in late menopause
Each section comes with an alarming array of symptoms, ranging from perimenopause fatigue and acne to late menopause tooth loss and vaginal prolapse. This is not to say that everyone will experience everything (fortunately), but rather, that these are the things that can happen and should not arrive unexpected.
Helpfully, of course, Dr. Gersh also gives advice on how to improve your energy and skin health, as well as keep your teeth and vagina in place. And similar professional insights for the rest of the “50 things you need to know”.
The style is like one big (182 pages) patient information leaflet—thus, very clear, explaining everything, and offering reassurance where possible and also what things are reasonable cause for seeking personalized medical attention.
Bottom line: if menopause is in your future, present, or very near past, this is an excellent book for you.
Click here to check out Menopause: 50 Things You Need To Know, and know them!
Share This Post
-

10almonds Tells The Tea…
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Let’s Bust Some Myths!
It’s too late after puberty, hormones won’t change xyz
While yes, many adult trans people dearly wish they’d been able to medically transition before going through the “wrong” puberty, the truth is that a lot of changes will still occur later… even to “unchangeable” things like the skeleton.
The body is remaking itself throughout life, and hormones tell it how to do that. Some parts are just quicker or slower than others. Also: the skeleton is pulled-on constantly by our muscles, and in a battle of muscle vs bone, muscle will always win over time.
Examples of this include:
- trans men building bigger bones to support their bigger muscles
- trans women getting smaller, with wider hips and a pelvic tilt
Trans people have sporting advantages
Assuming at least a year’s cross-sex hormonal treatment, there is no useful advantage to being trans when engaging in a sport. There are small advantages and disadvantages (which goes for any person’s body, really). For example:
- Trans women will tend to be taller than cis women on average…
- …but that larger frame is now being powered by smaller muscles, because they shrink much quicker than the skeleton.
- Trans men taking T are the only athletes allowed to take testosterone…
- …but they will still often be smaller than their fellow male competitors, for example.
Read: Do Trans Women Athletes Have Advantages? (A rather balanced expert overview, which does also cover trans men)
There’s a trans population explosion; it’s a social contagion epidemic!

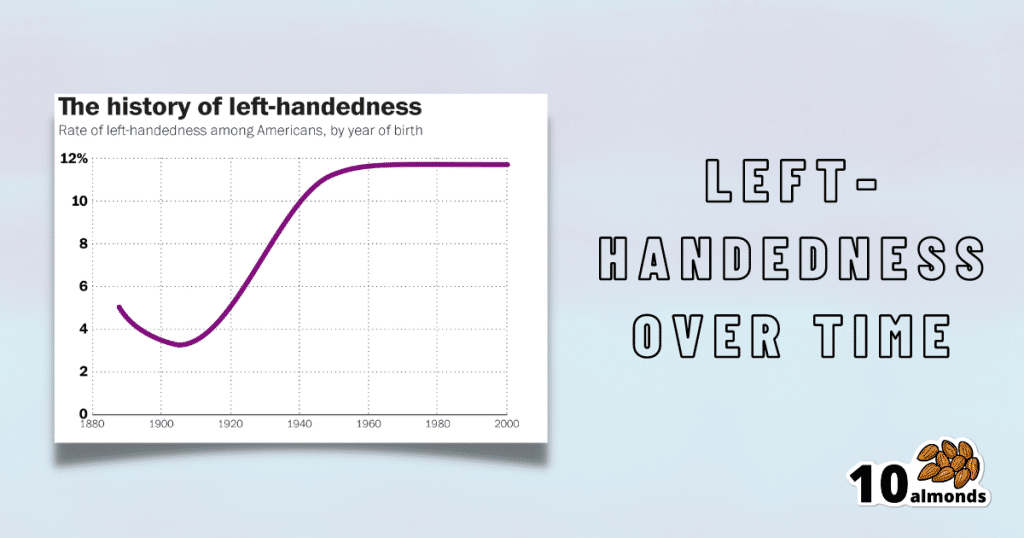
Source for figures: The Overall Rate Of Left-Handedness (Researchgate)
Left-handed people used to make up around 3% of the population… Until the 1920s, when that figure jumped sharply upwards, before plateauing at around 12% in around 1960, where it’s stayed since. What happened?! Simple, schools stopped forcing children to use their right hand.
Today, people ask for trans healthcare because they know it exists! Decades ago, it wasn’t such common knowledge.
The same explanation can be applied to other “population explosions” such as for autism and ADHD.
Fun fact: Mt. Everest was “discovered” in 1852, but scientists suspect it probably existed long before then! People whose ancestors were living on it long before 1852 also agree. Sometimes something exists for a long time, and only comes to wider public awareness later.
Transgender healthcare is too readily available, especially to children!
To believe some press outlets, you’d think:
- HRT is available from school vending machines,
- kids can get a walk-in top surgery at recess,
- and there’s an after-school sterilization club.
In reality, while availability varies from place to place, trans healthcare is heavily gatekept. Even adults have trouble getting it, often having to wait years and/or pay large sums of money… and get permission from a flock of doctors, psychologists, and the like. For those under the age of 18, it’s almost impossible in many places, even with parental support.
Puberty-blockers shouldn’t be given to teenagers, as the effects are irreversible
Quick question: who do you think should be given puberty-blockers? For whom do you think they were developed? Not adults, for sure! They were not developed for trans teens either, but for cis pre-teens with precocious puberty, to keep puberty at bay, to do it correctly later. Nobody argues they’re unsafe for much younger cis children, and only object when it’s trans teens.
They’re not only safe and reversible, but also self-reversing. Stop taking them, and the normally scheduled puberty promptly ensues by itself. For trans kids, the desired effect is to buy the kid time to make an informed and well-considered decision. After all, the effects of the wrong puberty are really difficult to undo!
A lot of people rush medical transition and regret it!
Trans people wish it could be rushed! It’s a lot harder to get gender-affirming care as a trans person, than it is to get the same (or comparable) care as a cis person. Yes, cis people get gender-affirming care, from hormones to surgeries, and have done for a long time.
As for regret… Medical transition has around a 1% regret rate. For comparison, hip replacement has a 4.8% regret rate and knee replacement has a 17.1% regret rate.
A medical procedure with a 99% success rate would generally be considered a miracle cure!
Share This Post
-

Alpha, beta, theta: what are brain states and brain waves? And can we control them?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There’s no shortage of apps and technology that claim to shift the brain into a “theta” state – said to help with relaxation, inward focus and sleep.
But what exactly does it mean to change one’s “mental state”? And is that even possible? For now, the evidence remains murky. But our understanding of the brain is growing exponentially as our methods of investigation improve.
Brain-measuring tech is evolving
Currently, no single approach to imaging or measuring brain activity gives us the whole picture. What we “see” in the brain depends on which tool we use to “look”. There are myriad ways to do this, but each one comes with trade-offs.
We learnt a lot about brain activity in the 1980s thanks to the advent of magnetic resonance imaging (MRI).
Eventually we invented “functional MRI”, which allows us to link brain activity with certain functions or behaviours in real time by measuring the brain’s use of oxygenated blood during a task.
We can also measure electrical activity using EEG (electroencephalography). This can accurately measure the timing of brain waves as they occur, but isn’t very accurate at identifying which specific areas of the brain they occur in.
Alternatively, we can measure the brain’s response to magnetic stimulation. This is very accurate in terms of area and timing, but only as long as it’s close to the surface.
What are brain states?
All of our simple and complex behaviours, as well as our cognition (thoughts) have a foundation in brain activity, or “neural activity”. Neurons – the brain’s nerve cells – communicate by a sequence of electrical impulses and chemical signals called “neurotransmitters”.
Neurons are very greedy for fuel from the blood and require a lot of support from companion cells. Hence, a lot of measurement of the site, amount and timing of brain activity is done via measuring electrical activity, neurotransmitter levels or blood flow.
We can consider this activity at three levels. The first is a single-cell level, wherein individual neurons communicate. But measurement at this level is difficult (laboratory-based) and provides a limited picture.
As such, we rely more on measurements done on a network level, where a series of neurons or networks are activated. Or, we measure whole-of-brain activity patterns which can incorporate one or more so-called “brain states”.
According to a recent definition, brain states are “recurring activity patterns distributed across the brain that emerge from physiological or cognitive processes”. These states are functionally relevant, which means they are related to behaviour.
Brain states involve the synchronisation of different brain regions, something that’s been most readily observed in animal models, usually rodents. Only now are we starting to see some evidence in human studies.
Various kinds of states
The most commonly-studied brain states in both rodents and humans are states of “arousal” and “resting”. You can picture these as various levels of alertness.
Studies show environmental factors and activity influence our brain states. Activities or environments with high cognitive demands drive “attentional” brain states (so-called task-induced brain states) with increased connectivity. Examples of task-induced brain states include complex behaviours such as reward anticipation, mood, hunger and so on.
In contrast, a brain state such as “mind-wandering” seems to be divorced from one’s environment and tasks. Dropping into daydreaming is, by definition, without connection to the real world.
We can’t currently disentangle multiple “states” that exist in the brain at any given time and place. As mentioned earlier, this is because of the trade-offs that come with recording spatial (brain region) versus temporal (timing) brain activity.
Brain states vs brain waves
Brain state work can be couched in terms such as alpha, delta and so forth. However, this is actually referring to brain waves which specifically come from measuring brain activity using EEG.
EEG picks up on changing electrical activity in the brain, which can be sorted into different frequencies (based on wavelength). Classically, these frequencies have had specific associations:
- gamma is linked with states or tasks that require more focused concentration
- beta is linked with higher anxiety and more active states, with attention often directed externally
- alpha is linked with being very relaxed, and passive attention (such as listening quietly but not engaging)
- theta is linked with deep relaxation and inward focus
- and delta is linked with deep sleep.
Brain wave patterns are used a lot to monitor sleep stages. When we fall asleep we go from drowsy, light attention that’s easily roused (alpha), to being relaxed and no longer alert (theta), to being deeply asleep (delta).
Can we control our brain states?
The question on many people’s minds is: can we judiciously and intentionally influence our brain states?
For now, it’s likely too simplistic to suggest we can do this, as the actual mechanisms that influence brain states remain hard to detangle. Nonetheless, researchers are investigating everything from the use of drugs, to environmental cues, to practising mindfulness, meditation and sensory manipulation.
Controversially, brain wave patterns are used in something called “neurofeedback” therapy. In these treatments, people are given feedback (such as visual or auditory) based on their brain wave activity and are then tasked with trying to maintain or change it. To stay in a required state they may be encouraged to control their thoughts, relax, or breathe in certain ways.
The applications of this work are predominantly around mental health, including for individuals who have experienced trauma, or who have difficulty self-regulating – which may manifest as poor attention or emotional turbulence.
However, although these techniques have intuitive appeal, they don’t account for the issue of multiple brain states being present at any given time. Overall, clinical studies have been largely inconclusive, and proponents of neurofeedback therapy remain frustrated by a lack of orthodox support.
Other forms of neurofeedback are delivered by MRI-generated data. Participants engaging in mental tasks are given signals based on their neural activity, which they use to try and “up-regulate” (activate) regions of the brain involved in positive emotions. This could, for instance, be useful for helping people with depression.
Another potential method claimed to purportedly change brain states involves different sensory inputs. Binaural beats are perhaps the most popular example, wherein two different wavelengths of sound are played in each ear. But the evidence for such techniques is similarly mixed.
Treatments such as neurofeedback therapy are often very costly, and their success likely relies as much on the therapeutic relationship than the actual therapy.
On the bright side, there’s no evidence these treatment do any harm – other than potentially delaying treatments which have been proven to be beneficial.

Susan Hillier, Professor: Neuroscience and Rehabilitation, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
Related Posts
-

Carrot vs Sweet Potato – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing carrot to sweet potato, we picked the sweet potato.
Why?
Both are great! But there’s a winner in the end:
Looking at the macros first, sweet potato has more protein carbs, and fiber, and is thus the “more food per food” item. If they are both cooked the same, then the glycemic index is comparable, despite the carrot’s carbs having more sucrose and the sweet potato’s carbs having more starch. We’ll call this category a tie.
In terms of vitamins, carrots have more of vitamins B9 and K, while sweet potatoes have more of vitamins B1, B2, B3, B5, B6. B7, C, E, and choline. Both are equally high in vitamin A. Thus, the vitamins category is an overwhelming win for sweet potato.
When it comes to minerals, carrots are not higher in any minerals (unless we count that they are slightly higher in sodium, but that is not generally considered a plus for most people in most places most of the time), while sweet potato is higher in calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. Another easy win for sweet potato.
Adding up the sections makes for a clear win for the sweet potato as the more nutritionally dense option, but as ever, enjoy either or both!
Want to learn more?
You might like to read:
What’s Your Plant Diversity Score?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
How much does your phone’s blue light really delay your sleep? Relax, it’s just 2.7 minutes
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s one of the most pervasive messages about technology and sleep. We’re told bright, blue light from screens prevents us falling asleep easily. We’re told to avoid scrolling on our phones before bedtime or while in bed. We’re sold glasses to help filter out blue light. We put our phones on “night mode” to minimise exposure to blue light.
But what does the science actually tell us about the impact of bright, blue light and sleep? When our group of sleep experts from Sweden, Australia and Israel compared scientific studies that directly tested this, we found the overall impact was close to meaningless. Sleep was disrupted, on average, by less than three minutes.
We showed the message that blue light from screens stops you from falling asleep is essentially a myth, albeit a very convincing one.
Instead, we found a more nuanced picture about technology and sleep.

Mangostar/Shutterstock What we did
We gathered evidence from 73 independent studies with a total of 113,370 participants of all ages examining various factors that connect technology use and sleep.
We did indeed find a link between technology use and sleep, but not necessarily what you’d think.
We found that sometimes technology use can lead to poor sleep and sometimes poor sleep can lead to more technology use. In other words, the relationship between technology and sleep is complex and can go both ways.
How is technology supposed to harm sleep?
Technology is proposed to harm our sleep in a number of ways. But here’s what we found when we looked at the evidence:
- bright screen light – across 11 experimental studies, people who used a bright screen emitting blue light before bedtime fell asleep an average of only 2.7 minutes later. In some studies, people slept better after using a bright screen. When we were invited to write about this evidence further, we showed there is still no meaningful impact of bright screen light on other sleep characteristics including the total amount or quality of sleep
- arousal is a measure of whether people become more alert depending on what they’re doing on their device. Across seven studies, people who engaged in more alerting or “exciting” content (for example, video games) lost an average of only about 3.5 minutes of sleep compared to those who engaged in something less exciting (for example, TV). This tells us the content of technology alone doesn’t affect sleep as much as we think
- we found sleep disruption at night (for example, being awoken by text messages) and sleep displacement (using technology past the time that we could be sleeping) can lead to sleep loss. So while technology use was linked to less sleep in these instances, this was unrelated to being exposed to bright, blue light from screens before bedtime.
Which factors encourage more technology use?
Research we reviewed suggests people tend to use more technology at bedtime for two main reasons:
- to “fill the time” when they’re not yet sleepy. This is common for teenagers, who have a biological shift in their sleep patterns that leads to later sleep times, independent of technology use.
- to calm down negative emotions and thoughts at bedtime, for apparent stress reduction and to provide comfort.
There are also a few things that might make people more vulnerable to using technology late into the night and losing sleep.
We found people who are risk-takers or who lose track of time easily may turn off devices later and sacrifice sleep. Fear of missing out and social pressures can also encourage young people in particular to stay up later on technology.
What helps us use technology sensibly?
Last of all, we looked at protective factors, ones that can help people use technology more sensibly before bed.
The two main things we found that helped were self-control, which helps resist the short-term rewards of clicking and scrolling, and having a parent or loved one to help set bedtimes.
We found having a parent or loved one to help set bedtimes encourages sensible use of technology. fast-stock/Shutterstock Why do we blame blue light?
The blue light theory involves melatonin, a hormone that regulates sleep. During the day, we are exposed to bright, natural light that contains a high amount of blue light. This bright, blue light activates certain cells at the back of our eyes, which send signals to our brain that it’s time to be alert. But as light decreases at night, our brain starts to produce melatonin, making us feel sleepy.
It’s logical to think that artificial light from devices could interfere with the production of melatonin and so affect our sleep. But studies show it would require light levels of about 1,000-2,000 lux (a measure of the intensity of light) to have a significant impact.
Device screens emit only about 80-100 lux. At the other end of the scale, natural sunlight on a sunny day provides about 100,000 lux.
What’s the take-home message?
We know that bright light does affect sleep and alertness. However our research indicates the light from devices such as smartphones and laptops is nowhere near bright or blue enough to disrupt sleep.
There are many factors that can affect sleep, and bright, blue screen light likely isn’t one of them.
The take-home message is to understand your own sleep needs and how technology affects you. Maybe reading an e-book or scrolling on socials is fine for you, or maybe you’re too often putting the phone down way too late. Listen to your body and when you feel sleepy, turn off your device.
Chelsea Reynolds, Casual Academic/Clinical Educator and Clinical Psychologist, College of Education, Psychology and Social Work, Flinders University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Myofascial Training – by Ester Albini
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Fascia is an oft-forgotten part of the body—if something that is so ubiquitous and varied can be described as a single part. And yet, it arguably is—precisely because it is the connective tissue that holds everything else together, so by its nature, it’s ultimately a one-piece thing.
This “one-piece thing” is responsible for permitting us movement, and is also responsible for restricting our movement. As such, when it comes to mobility, we can stretch our muscles all day long and it won’t mean a thing if our fascia is stiff. And notably, fascia has a much slower turnover time (in terms of how quickly the body replaces it) than muscle, so fascia is almost always going to be the limiting factor.
Pilates instructor (with many certifications) Albini gives the reader the tools to loosen up that limiting factor. It’ll take time and consistency (it takes the body around 18 months to fully rebuild fascia, so that’s the timeframe for an ultimate “job done” to then just be maintained), but there are also some results to be enjoyed immediately, by virtue of myofascial release
In style, the book is half textbook, half workbook. She explains a lot of the anatomy and physiology of fascia (and does so very well). This book is, in this reviewer’s opinion, better than the usual go-to professional guidebook to fascia (i.e., for physiotherapists etc) that costs more than twice the price and is half as clear (the other book’s diagrams are unnecessarily abstract, the photos fuzzy, and the prose tedious). This book, in contrast, has very clear diagrams, hundreds of high-quality color photos, and excellent explanations that are aimed at the layperson, and/but aren’t afraid to get technical either; she just explains the technicalities well too.
The workbook side of things is a vast array of exercises to do, including for specific issues and to combat various lifestyle problems, as well as to just support general health and more mobility than most people think is possible for them.
Bottom line: if you’d like better mobility and have been neglecting your fascia (or have been a bit confused by it), this book is going to be your new best friend.
Click there to check out Myofascial Training, and free your body’s movements!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: