The Tiniest Seeds With The Most Value
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If You’re Not Taking Chia, You’re Missing Out
Last Tuesday, we wrote about nutritional psychiatry, and the benefits of eating for one’s mental health.
You can check out Dr. Uma Naidoo’s to-dos, here:
The 6 Pillars Of Nutritional Psychiatry
In response, one of our subscribers wrote to mention:
❝Really interesting….just put chia seeds in my diet love them……taking the Drs advice.❞
~ Cindy, 10almonds subscriber
And then! On Friday, our tip at the top of the newsletter was:
Not sure how to incorporate chia seeds into your diet? It’s easier to want the benefits of their many brain-healthy (and otherwise-healthy, too) nutrients, than it is to know what to do with them necessarily, and not everyone enjoys seeds as a snack. So…
When you cook rice, throw in a tablespoon of chia seeds too. The cooking process will soften them and they won’t be texturally any different than the rice, but the nutrients will be all there.
They can also be thrown in with lentils, in the same fashion! Or oatmeal, when cooking it or making overnight oats.
We’ll be honest, it was Cindy’s comment that prompted us to suggest it. But wait! There was more to come in response:
❝You had a teaser ..on Chia seed.would of liked a article on the benefits . I’ve just discovered Chia seeds…❞
~ Cindy, 10almonds subscriber
So, Cindy, this one’s for you:
Nutritional powerhouse
First things first, these tiny seeds have a lot of nutrients. There are not many more nutrient-dense foods than this (there’s a kind of seaweed that might be a contender; we’ll have to do some research and get back to you).
Check them out:
USDA Nutritional Factsheet: Chia Seeds
So much protein and healthy fat, so many vitamins and minerals, and so many miscellaneous other micronutrients that we’d be here all day to list them (which is why we linked the above factsheet instead).
Antioxidants in abundance
These deserve a special mention, because they include quercetin which we’ve written about previously:
Fight Inflammation & Protect Your Brain, With Quercetin
…as well as quite a collection of others (including chlorogenic acid and caffeic acid, which may sound alarming but are great for lowering your blood pressure and against inflammation, respectively):
- The effect of chlorogenic acid on blood pressure: a systematic review and meta-analysis of randomized clinical trials
- Synthesis, preliminary bioevaluation and computational analysis of caffeic acid analogues
There are others too, with cardioprotective effects, liver-healthy effects, and anticancer properties:
Nutritional and therapeutic perspectives of Chia (Salvia hispanica L.): a review
Good for the heart and blood
Check it out:
- Chia flour supplementation reduces blood pressure in hypertensive subjects
- Chia seed (Salvia hispanica L.) supplementation to the diet of adults with type 2 diabetes improved systolic blood pressure: A randomized controlled trial
Oh, and about diabetes? There’s more, this time pertaining to reducing after-dinner blood sugars (or “postpranidial glycemia”, in sciencese):
- Reduction in postprandial glucose excursion and prolongation of satiety: possible explanation of the long-term effects of whole grain Salba (Salvia Hispanica L.)
- Effect of whole and ground Salba seeds (Salvia Hispanica L.) on postprandial glycemia in healthy volunteers: a randomized controlled, dose-response trial
Good for the brain
Regular 10almonds readers will know that “what’s good for the blood, is good for the brain” is a very good rule of thumb already, but their highomega-3 content makes them especially so:
What Omega-3 Fatty Acids Really Do For Us
Want some?
We don’t sell them, but you can probably find them in your local supermarket and/or health food store, and if you prefer getting things online, here for your convenience is an example product on Amazon
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Fennel vs Artichoke – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing fennel to artichoke, we picked the artichoke.
Why?
Both are great! But artichoke wins on nutritional density.
In terms of macros, artichoke has more protein and more fiber, for only slightly more carbs.
Vitamins are another win for artichoke, boasting more of vitamins B1, B2, B3, B5, B6, B9, and choline. Meanwhile, fennel has more of vitamins A, E, and K, which is also very respectable but does allow artichoke a 6:3 lead.
In the category of minerals, artichoke has a lot more copper, iron, magnesium, manganese, and phosphorus, while fennel has a little more calcium, potassium, and selenium.
One other relevant factor is that fennel is a moderate appetite suppressant, which may be good or bad depending on your food-related goals.
All in all though, we say the artichoke wins by virtue of its greater abundance of nutrients!
Want to learn more?
You might like to read:
What Matters Most For Your Heart? ← appropriately enough, with fennel hearts and artichoke hearts!
Take care!
Share This Post
-

Reading As A Cognitive Exercise
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Reading, Better
It is relatively uncontroversial to say that reading is good for cognitive health, but we don’t like to make claims without science if we can help it, so let’s get started:
There was a 2021 study, which found that even when controlling for many other factors, including highest level of education, socioeconomic status, and generalized pre-morbid intelligence:
❝high reading activity, as defined by almost daily reading, was associated with lower odds of cognitive decline, compared to low reading activity❞
Source: Can reading increase cognitive reserve?
However, not all reading is the same. And this isn’t just about complexity or size of vocabulary, either. It’s about engagement.
And that level of engagement remains the key factor, no matter how quickly or slowly someone reads, as the brain tends to automatically adjust reading speed per complexity, because the brain’s “processing speed” remains the same:
Read more: Cognitive coupling during reading
Everyone’s “processing speed” is different (and is associated with generalized intelligence and executive functions), though as a general rule of thumb, the more we practice it, the faster our processing speed gets. So if you balked at the notion of “generalized intelligence” being a factor, be reassured that this association goes both ways.
So is the key to just read more?
That’s a great first step! But…
The key factor still remains: engagement.
So what does that mean?
It is not just the text that engages you. You must also engage the text!
This is akin to the difference between learning to drive by watching someone else do it, and learning by getting behind the wheel and having a go.
When it comes to reading, it should not be a purely passive thing. Sure, if you are reading a fiction book at bedtime, get lost in it, by all means. But when it comes to non-fiction reading, engage with it actively!
For example, I (your writer here, hi), when reading non-fiction:
- Read at what is generally considered an unusually fast pace, but
- Write so many notes in the margins of physical books, and
- Write so many notes using the “Notes” function on my Kindle
And this isn’t just like a studious student taking notes. Half the time I am…
- objecting to content (disagreeing with the author), or
- at least questioning it, or which is especially important, or
- noting down questions that came to my mind as a result of what I am reading.
This latter is a bit like:
- when you are reading 10almonds, sometimes you will follow our links and go off down a research rabbit-hole of your own, and that’s great!
- sometimes you will disagree with something and write to tell us, and that’s great too (when this happens, one or the other or all of us will learn something, and yes, we have published corrections before now)!
- sometimes what you read here will prompt a further question, and you’ll send that to us, and guess what, also great! We love questions.
Now, if your enjoyment of 10almonds is entirely passive, don’t let us stop you (we know our readers like quick-and-easy knowledge, and that’s good too), it’s just, the more you actively engage with it, the more you’ll get out of it.
This, by the way, was also a lifelong habit of Leonardo da Vinci, which you can read about here:
How to Think Like Leonardo da Vinci: Seven Steps to Genius Every Day – by Michael J. Gelb
a very good book that we reviewed last year
How you read (i.e. what medium) matters too!
Are you reading this on a desktop/laptop, or a mobile device? That difference could matter more than the difference between paper and digital, according to this study from 2020 that found…
❝The cumulation of evidence from this and previous studies suggests that reading on a tablet affords different interactions between the reader and the text than reading on a computer screen.
Reading on a tablet might be more similar to reading on paper, and this may impact the attentional processes during reading❞
What if my mind wanders easily?
You can either go with it, or train to improve focus.
Going with it: just make sure you have more engaging reading to get distracted by. It’s all good.
Training focus: this is trickier, but worthwhile, as executive function (you will remember from earlier) was an important factor too, and training focus is training executive function.
As for one way to do that…
If you’d like a primer for getting going with that, then you may enjoy our previous main feature:
No-Frills, Evidence-Based Mindfulness
Enjoy!
Share This Post
-
What’s the difference between wholemeal and wholegrain bread? Not a whole lot
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you head to the shops to buy bread, you’ll face a variety of different options.
But it can be hard to work out the difference between all the types on sale.
For instance, you might have a vague idea that wholemeal or wholegrain bread is healthy. But what’s the difference?
Here’s what we know and what this means for shoppers in Australia and New Zealand.

Phish Photography/Shutterstock Let’s start with wholemeal bread
According to Australian and New Zealand food standards, wholemeal bread is made from flour containing all parts of the original grain (endosperm, germ and bran) in their original proportions.
Because it contains all parts of the grain, wholemeal bread is typically darker in colour and slightly more brown than white bread, which is made using only the endosperm.
Wholemeal flour is made from all parts of the grain. Rerikh/Shutterstock How about wholegrain bread?
Australian and New Zealand food standards define wholegrain bread as something that contains either the intact grain (for instance, visible grains) or is made from processed grains (flour) where all the parts of the grain are present in their original proportions.
That last part may sound familiar. That’s because wholegrain is an umbrella term that encompasses both bread made with intact grains and bread made with wholemeal flour. In other words, wholemeal bread is a type of wholegrain bread, just like an apple is a type of fruit.
Don’t be confused by labels such as “with added grains”, “grainy” or “multigrain”. Australian and New Zealand food standards don’t define these so manufacturers can legally add a small amount of intact grains to white bread to make the product appear healthier. This doesn’t necessarily make these products wholegrain breads.
So unless a product is specifically called wholegrain bread, wholemeal bread or indicates it “contains whole grain”, it is likely to be made from more refined ingredients.
Which one’s healthier?
So when thinking about which bread to choose, both wholemeal and wholegrain breads are rich in beneficial compounds including nutrients and fibre, more so than breads made from further-refined flour, such as white bread.
The presence of these compounds is what makes eating wholegrains (including wholemeal bread) beneficial for our overall health. Research has also shown eating wholegrains helps reduce the risk of common chronic diseases, such as heart disease.
The table below gives us a closer look at the nutritional composition of these breads, and shows some slight differences.
Wholegrain bread is slightly higher in fibre, protein, niacin (vitamin B3), iron, zinc, phosphorus and magnesium than wholemeal bread. But wholegrain bread is lower in carbohydrates, thiamin (vitamin B1) and folate (vitamin B9).
However the differences are relatively small when considering how these contribute to your overall dietary intake.
Which one should I buy?
Next time you’re shopping, look for a wholegrain bread (one made from wholemeal flour that has intact grains and seeds throughout) as your number one choice for fibre and protein, and to support overall health.
If you can’t find wholegrain bread, wholemeal bread comes in a very close second.
Wholegrain and wholemeal bread tend to cost the same, but both tend to be more expensive than white bread.
Margaret Murray, Senior Lecturer, Nutrition, Swinburne University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



-

The Brain As A Work-In-Progress
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
And The Brain Goes Marching On!

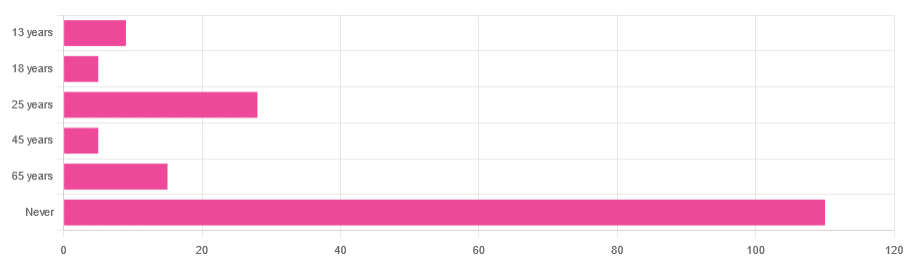
In Tuesday’s newsletter, we asked you “when does the human brain stop developing?” and got the above-depicted, below-described, set of responses:
- About 64% of people said “Never”
- About 16% of people said “25 years”
- About 9% of people said “65 years”
- About 5% of people said “13 years”
- About 3% of people said “18 years”
- About 3% of people said “45 years”
Some thoughts, before we get into the science:
An alternative wording for the original question was “when does the human brain finish developing”; the meaning is the same but the feeling is slightly different:
- “When does the human brain stop developing?” focuses attention on the idea of cessation, and will skew responses to later ages
- When does the human brain finish developing?” focuses on attention on a kind of “is it done yet?” and will skew responses to earlier ages
Ultimately, since we had to chose one word or another, we picked the shortest one, but it would have been interesting if we could have done an A/B test, and asked half one way, and half the other way!
Why we picked those ages
We picked those ages as poll options for reasons people might be drawn to them:
- 13 years: in English-speaking cultures, an important milestone of entering adolescence (note that the concept of a “teenager” is not precisely universal as most languages do not have “-teen” numbers in the same way; the concept of “adolescent” may thus be tied to other milestones)
- 18 years: age of legal majority in N. America and many other places
- 25 years: age popularly believed to be when the brain is finished developing, due to a study that we’ll talk about shortly (we guess that’s why there’s a spike in our results for this, too!)
- 45 years: age where many midlife hormonal changes occur, and many professionals are considered to have peaked in competence and start looking towards retirement
- 65 years: age considered “senior” in much of N. America and many other places, as well as the cut-off and/or starting point for a lot of medical research
Notice, therefore, how a lot of things are coming from places they really shouldn’t. For example, because there are many studies saying “n% of people over 65 get Alzheimer’s” or “n% of people over 65 get age-related cognitive decline”, etc, 65 becomes the age where we start expecting this—because of an arbitrary human choice of where to draw the cut-off for the study enrollment!
Similarly, we may look at common ages of legal majority, or retirement pensions, and assume “well it must be for a good reason”, and dear reader, those reasons are more often economically motivated than they are biologically reasoned.
So, what does the science say?
Our brains are never finished developing: True or False?
True! If we define “finished developing” as “we cease doing neurogenesis and neuroplasticity is no longer in effect”.
Glossary:
- Neurogenesis: the process of creating new brain cells
- Neuroplasticity: the process of the brain adapting to changes by essentially rebuilding itself to suit our perceived current needs
We say “perceived” because sometimes neuroplasticity can do very unhelpful things to us (e.g: psychological trauma, or even just bad habits), but on a biological level, it is always doing its best to serve our overall success as an organism.
For a long time it was thought that we don’t do neurogenesis at all as adults, but this was found to be untrue:
How To Grow New Brain Cells (At Any Age)
Summary of conclusions of the above: we’re all growing new brain cells at every age, even if we be in our 80s and with Alzheimer’s disease, but there are things we can do to enhance our neurogenic potential along the way.
Neuroplasticity will always be somewhat enhanced by neurogenesis (after all, new neurons get given jobs to do), and we reviewed a great book about the marvels of neuroplasticity including in older age:
Our brains are still developing up to the age of 25: True or False?
True! And then it keeps on developing after that, too. Now this is abundantly obvious considering what we just talked about, but see what a difference the phrasing makes? Now it makes it sound like it stops at 25, which this statement doesn’t claim at all—it only speaks for the time up to that age.
A lot of the popular press about “the brain isn’t fully mature until the age of 25” stems from a 2006 study that found:
❝For instance, frontal gray matter volume peaks at about age 11.0 years in girls and 12.1 years in boys, whereas temporal gray matter volume peaks at about age at 16.7 years in girls and 16.2 years in boys. The dorsal lateral prefrontal cortex, important for controlling impulses, is among the latest brain regions to mature without reaching adult dimensions until the early 20s.❞
Source: Structural Magnetic Resonance Imaging of the Adolescent Brain
There are several things to note here:
- The above statement is talking about the physical size of the brain growing
- Nowhere does he say “and stops developing at 25”
However… The study only looked at brains up to the age of 25. After that, they stopped looking, because the study was about “the adolescent brain” so there has to be a cut-off somewhere, and that was the cut-off they chose.
This is the equivalent of saying “it didn’t stop raining until four o’clock” when the reality is that four o’clock is simply when you gave up on checking.
The study didn’t misrepresent this, by the way, but the popular press did!
Another 2012 study looked at various metrics of brain development, and found:
- Synapse overproduction into the teens
- Cortex pruning into the late 20s
- Prefrontal pruning into middle age at least (they stopped looking)
- Myelination beyond middle age (they stopped looking)
Source: Experience and the developing prefrontal cortex ← check out figure 1, and make sure you’re looking at the human data not the rat data
So how’s the most recent research looking?
Here’s a 2022 study that looked at 123,984 brain scans spanning the age range from mid-gestation to 100 postnatal years, and as you can see from its own figure 1… Most (if not all) brain-things keep growing for life, even though most slow down at some point, they don’t stop:
Brain charts for the human lifespan ← check out figure 1; don’t get too excited about the ventricular volume column as that is basically “brain that isn’t being a brain”. Do get excited about the rest, though!
Want to know how not to get caught out by science being misrepresented by the popular press? Check out:
How Science News Outlets Can Lie To You (Yes, Even If They Cite Studies!)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Stand Up For Your Health (Or Don’t)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You may have heard the phrase “sitting is the new smoking”, and while the jury’s out on whether that’s accurate or not in terms of exactly how damaging it is, one thing that is universally agreed-upon is that sitting is indeed very bad.
It’s especially bad for your spine (because of being folded in ways it shouldn’t be), your muscles and associated nerves of the lower back and hip area, your abdominal organs (because of being compressed in ways they shouldn’t be), and your heart (because of arteries and veins being squashed up in ways they shouldn’t be), and if you remember how “what’s good for your heart is good for your brain”, the inverse is true, and what’s bad for your heart is also bad for your brain, which won’t get nourished with oxygen and nutrients and which won’t have its detritus removed as efficiently as it should; that’ll be left to build up in the brain instead.
First, elephant in the room: not everybody can stand, and of those who can, not everybody can stand for long. So obviously, work within what’s attainable for you.
Also note that while sitting is the disease-bringer/worsener, standing isn’t the only solution, for example:
- Walking is better than standing. You may be wondering: “who can’t stand but can walk?” and the answer is, a lot of people with certain kinds of chronic pain, for whom walking is less chronic-pain-exacerbating than standing, because the human body is built for movement and inactivity can worsen things even more than movement.
- See also: Managing Chronic Pain (Realistically)
- Lying down is better than sitting. One of the major problems with sitting is that your organs are all bunched up in ways they shouldn’t be. Lying down is, in this regard, closer to standing than sitting, because your body has a nice straight line to it.
- Sitting can be made less bad! For example:
- Sitting in a recliner chair in the reclined position is… Not great, if you’re then tilting your skull forwards to compensate, but if you’re just sitting back and relaxing, this is a lot better than sitting in the usual seated position, because again, it’s closer to lying down, which is closer to standing.
- Sitting in seiza (the traditional Japanese kneeling position) is, provided you do it correctly and with good posture, better than sitting in the traditional Western manner. The reason for this is simple: instead of having your torso and legs at 90°, they are at 120°ish, give or take the size of your thighs and butt (bigger being better in this regard), and even that angle can be made even better if you use a meditation bench like this one ← we’re eyeballing it and didn’t get out a protractor, but if you look at the model’s torso and thighs, that’s about 135° difference, which is huge improvement over the 90° you get while sitting Western-style.
For most of us a lot of the time though, we can stand to sit less. Think about the places you most often sit, and what can be done to reasonably minimize those, for example:
- Car: minimize driving (or being a passenger in a car); walk where reasonably possible. Public transport, if available, may have standing options.
- Office: a standing desk is, of course, the way to go. You can even use a standing desk converter, like this one. Just make sure to set it at the correct height, both in terms of where the keyboard and mouse go (the same height as your elbows are when your arms are dropped to your sides), and where the monitor goes (center of the monitor should be at eye-level).
- Note: laptops will never be right for this, unless the natural resting distance between your elbows and your eyes is about 4½ inches, which will only be the case if your total height is approximately 1 foot and 2 inches. For anyone taller than that, laptops are still great to have when on the move and as a backup, but not great for ergonomics.
- Workaround: if for some reason you must use a laptop for your day-to-day work, consider using a bluetooth keyboard so that you can still set them the appropriate height-distance apart and thus not have to hunch over them.
- Dining room: sitting to eat a main meal is reasonable, but consider standing options for lighter bites; a standing-height “brunch bar” is great if you can arrange one.
- Lounge: let it live up to its name, and actually lounge: if you’re not going to stand, then horizontal lounging is an improvement over sitting—as is sitting on the floor, and changing your position frequently. Who knew, kids had it right in that regard!
- Note: if, like this writer, you do a lot of reading, the same applies regardless of which room you’re doing it in.
- Bedroom: a culprit for many will be sitting while doing a beauty routine and/or possibly make-up. Easily avoided if you set a well-lit mirror at the correct height to use while standing.
- Note: at the correct height though! While hunching up over a wall-mounted mirror is an improvement over hunching up at a seated vanity, it’s not a great improvement. You want to be able to stand with good posture and do it comfortably.
- Bathroom: leave your phone outside—which is also a good approach for avoiding hemorrhoids! See also: Half Of Americans Over 50 Have Hemorrhoids, But They Can Be Prevented!
Want to know more?
We reviewed this book recently, which goes into all of the above in much more detail than we have room for here, plus also discusses a lot of social reframes that can be used (since a lot of sitting is a matter of social expectations, not actual need). It’s a very useful read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- Walking is better than standing. You may be wondering: “who can’t stand but can walk?” and the answer is, a lot of people with certain kinds of chronic pain, for whom walking is less chronic-pain-exacerbating than standing, because the human body is built for movement and inactivity can worsen things even more than movement.
-

A new emergency procedure for cardiac arrests aims to save more lives – here’s how it works
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
As of January this year, Aotearoa New Zealand became just the second country (after Canada) to adopt a groundbreaking new procedure for patients experiencing cardiac arrest.
Known as “double sequential external defibrillation” (DSED), it will change initial emergency response strategies and potentially improve survival rates for some patients.
Surviving cardiac arrest hinges crucially on effective resuscitation. When the heart is working normally, electrical pulses travel through its muscular walls creating regular, co-ordinated contractions.
But if normal electrical rhythms are disrupted, heartbeats can become unco-ordinated and ineffective, or cease entirely, leading to cardiac arrest.
Defibrillation is a cornerstone resuscitation method. It gives the heart a powerful electric shock to terminate the abnormal electrical activity. This allows the heart to re-establish its regular rhythm.
Its success hinges on the underlying dysfunctional heart rhythm and the proper positioning of the defibrillation pads that deliver the shock. The new procedure will provide a second option when standard positioning is not effective.
Using two defibrillators
During standard defibrillation, one pad is placed on the right side of the chest just below the collarbone. A second pad is placed below the left armpit. Shocks are given every two minutes.
Early defibrillation can dramatically improve the likelihood of surviving a cardiac arrest. However, around 20% of patients whose cardiac arrest is caused by “ventricular fibrillation” or “pulseless ventricular tachycardia” do not respond to the standard defibrillation approach. Both conditions are characterised by abnormal activity in the heart ventricles.
DSED is a novel method that provides rapid sequential shocks to the heart using two defibrillators. The pads are attached in two different locations: one on the front and side of the chest, the other on the front and back.
A single operator activates the defibrillators in sequence, with one hand moving from the first to the second. According to a recent randomised trial in Canada, this approach could more than double the chances of survival for patients with ventricular fibrillation or pulseless ventricular tachycardia who are not responding to standard shocks.
The second shock is thought to improve the chances of eliminating persistent abnormal electrical activity. It delivers more total energy to the heart, travelling along a different pathway closer to the heart’s left ventricle.
Evidence of success
New Zealand ambulance data from 2020 to 2023 identified about 1,390 people who could potentially benefit from novel defibrillation methods. This group has a current survival rate of only 14%.
Recognising the potential for DSED to dramatically improve survival for these patients, the National Ambulance Sector Clinical Working Group updated the clinical procedures and guidelines for emergency medical services personnel.
The guidelines now specify that if ventricular fibrillation or pulseless ventricular tachycardia persist after two shocks with standard defibrillation, the DSED method should be administered. Two defibrillators need to be available, and staff must be trained in the new approach.
Though the existing evidence for DSED is compelling, until recently it was based on theory and a small number of potentially biased observational studies. The Canadian trial was the first to directly compare DSED to standard treatment.
From a total of 261 patients, 30.4% treated with this strategy survived, compared to 13.3% when standard resuscitation protocols were followed.
The design of the trial minimised the risk of other factors confounding results. It provides confidence that survival improvements were due to the defibrillation approach and not regional differences in resources and training.
The study also corroborates and builds on existing theoretical and clinical scientific evidence. As the trial was stopped early due to the COVID-19 pandemic, however, the researchers could recruit fewer than half of the numbers planned for the study.
Despite these and other limitations, the international group of experts that advises on best practice for resuscitation updated its recommendations in 2023 in response to the trial results. It suggested (with caution) that emergency medical services consider DSED for patients with ventricular fibrillation or pulseless ventricular tachycardia who are not responding to standard treatment.
Training and implementation
Although the evidence is still emerging, implementation of DSED by emergency services in New Zealand has implications beyond the care of patients nationally. It is also a key step in advancing knowledge about optimal resuscitation strategies globally.
There are always concerns when translating an intervention from a controlled research environment to the relative disorder of the real world. But the balance of evidence was carefully considered before making the decision to change procedures for a group of patients who have a low likelihood of survival with current treatment.
Before using DSED, emergency medical personnel undergo mandatory education, simulation and training. Implementation is closely monitored to determine its impact.
Hospitals and emergency departments have been informed of the protocol changes and been given opportunities to ask questions and give feedback. As part of the implementation, the St John ambulance service will perform case reviews in addition to wider monitoring to ensure patient safety is prioritised.
Ultimately, those involved are optimistic this change to cardiac arrest management in New Zealand will have a positive impact on survival for affected patients.

Vinuli Withanarachchie, PhD candidate, College of Health, Massey University; Bridget Dicker, Associate Professor of Paramedicine, Auckland University of Technology, and Sarah Maessen, Research Associate, Auckland University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: