The Wim Hof Method – by Wim Hof
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In Wednesday’s main feature, we wrote about the Wim Hof Method, and/but only scratched the surface. Such is the downside of being a super-condensed newsletter! However, it does give us the opportunity to feature the book:
The Wim Hof Method is definitely loudly trumpeted as “up there” with Atomic Habits or How Not To Die in the category of “life-changing” books. Why?
Firstly, it’s a very motivational book. Hof is a big proponent of the notion “if you think you can or you think you can’t, you’re right” idea, practises what he preaches, and makes clear he’s not special.
Secondly, it’s backed up with science. While it’s not a science-heavy book and that’s not the main focus, there are references to studies. Where physiological explanations are given for how certain things work, those explanations are sound. There’s no pseudoscience here, which is especially important for a book of this genre!
What does the book have that our article didn’t? A good few things:
- More about Hof’s own background and where it’s taken him. This is generally not a reason people buy books (unless they are biographies), but it’s interesting nonetheless.
- A lot more advice, data, and information about Cold Therapy and how it can (and, he argues convincingly, should) be built into your life.
- A lot about breathing exercises that we just didn’t cover at all in our article, but is actually an important part of the Wim Hof Method.
- More about stepping through the psychological barriers that can hold us back.
Bottom line: this book offers benefits that stretch into many areas of life, from some simple habits that can be built.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Stretching for 50+ – by Dr. Karl Knopf

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Knopf explores in this book the two-way relationship between aging and stretching (i.e., each can have a large impact on the other). Thinking about stretching in those terms is an important reframe for going into any stretching program. We’d say “after the age of 50”, but honestly, at any age. But this book is written with over-50s in mind, as the title goes.
There’s an extensive encyclopedic section on stretches per body part, which is exactly as you might expect from any book of this kind. There is also a flexibility self-assessment, so that progress can be measured easily, and so that the reader knows where might need more improvement.
Perhaps this book’s greatest strength is the section on specialized programs based on things ranging from working to improve symptoms of any chronic conditions you may have (or at least working around them, if outright improvement is not possible by stretching), to your recreational activities of importance to you—so, what kinds of flexibilities will be important to you, and also, what kinds of injury you are most likely to need to avoid.
Bottom line: if you’re 50 and would like to do more stretching and less aging, then this book can help with that.
Click here to check out Stretching for 50+, and extend your healthspan!
Share This Post
-

Native Americans Have Shorter Life Spans. Better Health Care Isn’t the Only Answer.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
HISLE, S.D. — Katherine Goodlow is only 20, but she has experienced enough to know that people around her are dying too young.
Goodlow, a member of the Lower Brule Sioux Tribe, said she’s lost six friends and acquaintances to suicide, two to car crashes, and one to appendicitis. Four of her relatives died in their 30s or 40s, from causes such as liver failure and covid-19, she said. And she recently lost a 1-year-old nephew.
“Most Native American kids and young people lose their friends at a young age,” said Goodlow, who is considering becoming a mental health therapist to help her community. “So, I’d say we’re basically used to it, but it hurts worse every time we lose someone.”
Native Americans tend to die much earlier than white Americans. Their median age at death was 14 years younger, according to an analysis of 2018-21 data from the Centers for Disease Control and Prevention
The disparity is even greater in Goodlow’s home state. Indigenous South Dakotans who died between 2017 and 2021 had a median age of 58 — 22 years younger than white South Dakotans, according to state data.
Donald Warne, a physician who is co-director of the Johns Hopkins Center for Indigenous Health and a member of the Oglala Sioux Tribe, can rattle off the most common medical conditions and accidents killing Native Americans.
But what’s ultimately behind this low life expectancy, agree Warne and many other experts on Indigenous health, are social and economic forces. They argue that in addition to bolstering medical care and fully funding the Indian Health Service — which provides health care to Native Americans — there needs to be a greater investment in case management, parenting classes, and home visits.
“It’s almost blasphemy for a physician to say,” but “the answer to addressing these things is not hiring more doctors and nurses,” Warne said. “The answer is having more community-based preventions.”
The Indian Health Service funds several kinds of these programs, including community health worker initiatives, and efforts to increase access to fresh produce and traditional foods.
Private insurers and state Medicaid programs, including South Dakota’s, are increasingly covering such services. But insurers don’t pay for all the services and aren’t reaching everyone who qualifies, according to Warne and the National Academy for State Health Policy.
Warne pointed to Family Spirit, a program developed by the Johns Hopkins center to improve health outcomes for Indigenous mothers and children.
Chelsea Randall, the director of maternal and child health at the Great Plains Tribal Leaders’ Health Board, said community health workers educate Native pregnant women and connect them with resources during home visits.
“We can be with them throughout their pregnancy and be supportive and be the advocate for them,” said Randall, whose organization runs Family Spirit programs across seven reservations in the Dakotas, and in Rapid City, South Dakota.
The community health workers help families until children turn 3, teaching parenting skills, family planning, drug abuse prevention, and stress management. They can also integrate the tribe’s culture by, for example, using their language or birthing traditions.
The health board funds Family Spirit through a grant from the federal Health Resources and Services Administration, Randall said. Community health workers, she said, use some of that money to provide child car seats and to teach parents how to properly install them to counter high rates of fatal crashes.
Other causes of early Native American deaths include homicide, drug overdoses, and chronic diseases, such as diabetes, Warne said. Native Americans also suffer a disproportionate number of infant and maternal deaths.
The crisis is evident in the obituaries from the Sioux Funeral Home, which mostly serves Lakota people from the Pine Ridge Reservation and surrounding area. The funeral home’s Facebook page posts obituaries for older adults, but also for many infants, toddlers, teenagers, young adults, and middle-aged residents.
Misty Merrival, who works at the funeral home, blames poor living conditions. Some community members struggle to find healthy food or afford heat in the winter, she said. They may live in homes with broken windows or that are crowded with extended family members. Some neighborhoods are strewn with trash, including intravenous needles and broken bottles.
Seeing all these premature deaths has inspired Merrival to keep herself and her teenage daughter healthy by abstaining from drugs and driving safely. They also talk every day about how they’re feeling, as a suicide-prevention strategy.
“We’ve made a promise to each other that we wouldn’t leave each other like that,” Merrival said.
Many Native Americans live in small towns or on poor, rural reservations. But rurality alone doesn’t explain the gap in life expectancy. For example, white people in rural Montana live 17 years longer, on average, than Native Americans in the state, according to state data reported by Lee Enterprises newspapers.
Many Indigenous people also face racism or personal trauma from child or sexual abuse and exposure to drugs or violence, Warne said. Some also deal with generational trauma from government programs and policies that broke up families and tried to suppress Native American culture.
Even when programs are available, they’re not always accessible.
Families without strong internet connections can’t easily make video appointments. Some lack cars or gas money to travel to clinics, and public transportation options are limited.
Randall, the health board official, is pregnant and facing her own transportation struggles.
It’s a three-hour round trip between her home in the town of Pine Ridge and her prenatal appointments in Rapid City. Randall has had to cancel several appointments when family members couldn’t lend their cars.
Goodlow, the 20-year-old who has lost several loved ones, lives with seven other people in her mother’s two-bedroom house along a gravel road. Their tiny community on the Pine Ridge Reservation has homes and ranches but no stores.
Goodlow attended several suicide-prevention presentations in high school. But the programs haven’t stopped the deaths. One friend recently killed herself after enduring the losses of her son, mother, best friend, and a niece and nephew.
A month later, another friend died from a burst appendix at age 17, Goodlow said. The next day, Goodlow woke up to find one of her grandmother’s parakeets had died. That afternoon, she watched one of her dogs die after having seizures.
“I thought it was like some sign,” Goodlow said. “I started crying and then I started thinking, ‘Why is this happening to me?’”
Warne said the overall conditions on some reservations can create despair. But those same reservations, including Pine Ridge, also contain flourishing art scenes and language and cultural revitalization programs. And not all Native American communities are poor.
Warne said federal, state, and tribal governments need to work together to improve life expectancy. He encourages tribes to negotiate contracts allowing them to manage their own health care facilities with federal dollars because that can open funding streams not available to the Indian Health Service.
Katrina Fuller is the health director at Siċaŋġu Co, a nonprofit group on the Rosebud Reservation in South Dakota. Fuller, a member of the Rosebud Sioux Tribe, said the organization works toward “wicozani,” or the good way of life, which encompasses the physical, emotional, cultural, and financial health of the community.
Siċaŋġu Co programs include bison restoration, youth development, a Lakota language immersion school, financial education, and food sovereignty initiatives.
“Some people out here that are struggling, they have dreams, too. They just need the resources, the training, even the moral support,” Fuller said. “I had one person in our health coaching class tell me they just really needed someone to believe in them, that they could do it.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-

Galveston Diet Cookbook for Beginners – by Martha McGrew
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We recently reviewed “The Galveston Diet”, and here’s a cookbook (by a nutritionist) to support that.
For the most part, it’s essentially keto-leaning, with an emphasis on protein and fats, but without quite the carb-cut that keto tends to have. It’s also quite plant-centric, but it’s not by default vegan or even vegetarian; you will find meat and fish in here. As you might expect from an anti-inflammatory cookbook, it’s light on the dairy too, though fermented dairy products such as yogurt do feature as well.
The recipes are quite simple and easy to follow, with suggestions of alternative ingredients along the way, making for extra variety as well as convenience.
If you are going to buy this book, you might want to take a look at the buying options, to ensure you get a full-color version, as recent reprints have photos in black and white, whereas older runs have color throughout.
Bottom line: if you’d like to cook the Galveston Diet way, this is as good a way to start as any.
Click here to check out the Galveston Diet Cookbook for Beginners, and get cooking!
Share This Post

Related Posts
-

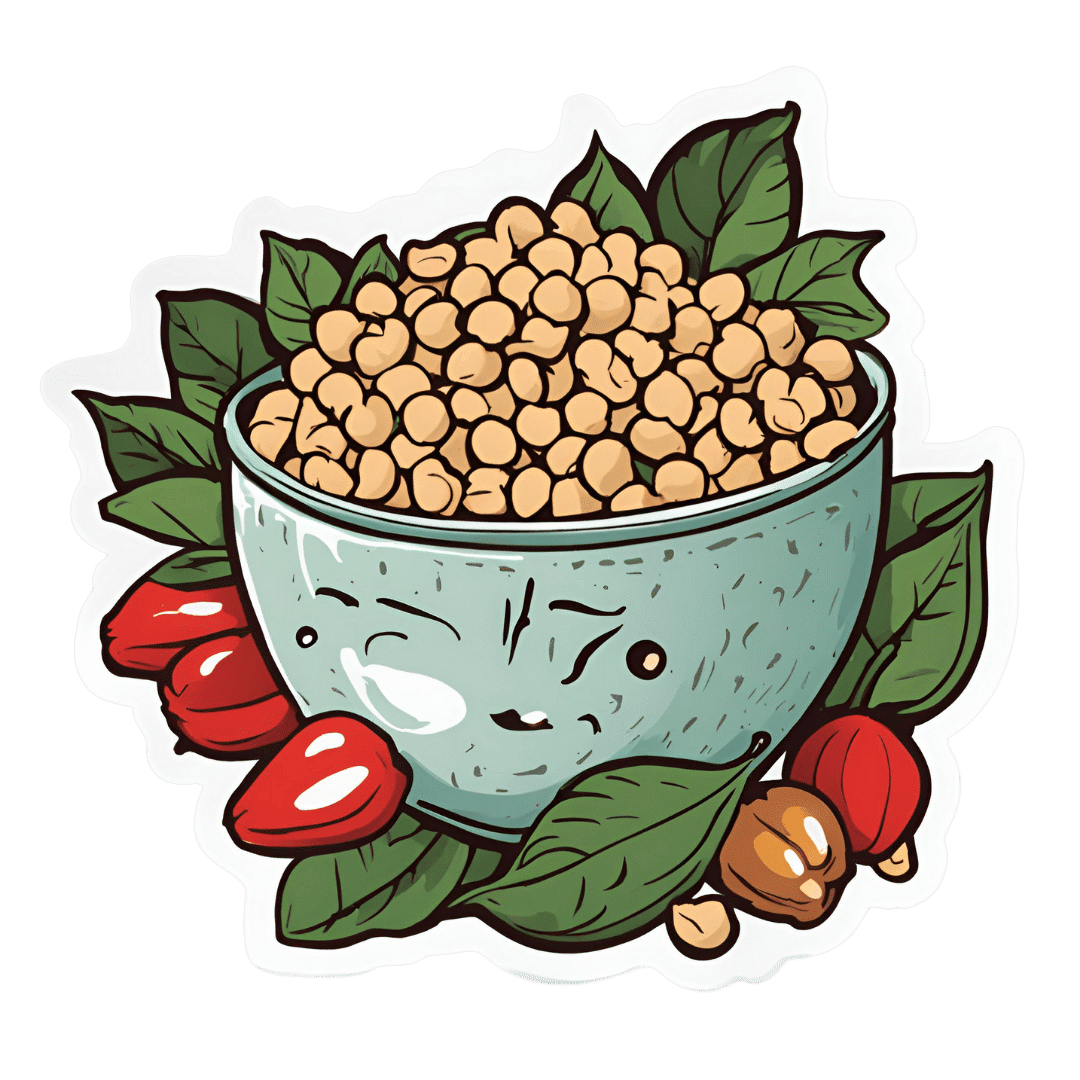
Protein Immune Support Salad
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How to get enough protein from a salad, without adding meat? Cashews and chickpeas have you more than covered! Along with the leafy greens and an impressive array of minor ingredients full of healthy phytochemicals, this one’s good for your muscles, bones, skin, immune health, and more.
You will need
- 1½ cups raw cashews (if allergic, omit; the chickpeas and coconut will still carry the dish for protein and healthy fats)
- 2 cans (2x 14oz) chickpeas, drained
- 1½ lbs baby spinach leaves
- 2 large onions, finely chopped
- 3 oz goji berries
- ½ bulb garlic, finely chopped
- 2 tbsp dessicated coconut
- 1 tbsp dried cumin
- 1 tbsp nutritional yeast
- 2 tsp chili flakes
- 1 tsp black pepper, coarse ground
- ½ tsp MSG, or 1 tsp low-sodium salt
- Extra virgin olive oil, for cooking
Method
(we suggest you read everything at least once before doing anything)
1) Heat a little oil in a pan; add the onions and cook for about 3 minutes.
2) Add the garlic and cook for a further 2 minutes.
3) Add the spinach, and cook until it wilts.
4) Add the remaining ingredients except the coconut, and cook for another three minutes.
5) Heat another pan (dry); add the coconut and toast for 1–2 minutes, until lightly golden. Add it to the main pan.
6) Serve hot as a main, or an attention-grabbing side:

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Cashew Nuts vs Coconut – Which is Healthier?
- What Matters Most For Your Heart?
- Beyond Supplements: The Real Immune-Boosters!
- Goji Berries: Which Benefits Do They Really Have?
- Our Top 5 Spices: How Much Is Enough For Benefits?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

A person in Texas caught bird flu after mixing with dairy cattle. Should we be worried?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The United States’ Centers for Disease Control and Prevention (CDC) has issued a health alert after the first case of H5N1 avian influenza, or bird flu, seemingly spread from a cow to a human.
A farm worker in Texas contracted the virus amid an outbreak in dairy cattle. This is the second human case in the US; a poultry worker tested positive in Colorado in 2022.
The virus strain identified in the Texan farm worker is not readily transmissible between humans and therefore not a pandemic threat. But it’s a significant development nonetheless.
Some background on bird flu
There are two types of avian influenza: highly pathogenic or low pathogenic, based on the level of disease the strain causes in birds. H5N1 is a highly pathogenic avian influenza.
H5N1 first emerged in 1997 in Hong Kong and then China in 2003, spreading through wild bird migration and poultry trading. It has caused periodic epidemics in poultry farms, with occasional human cases.
Influenza A viruses such as H5N1 are further divided into variants, called clades. The unique variant causing the current epidemic is H5N1 clade 2.3.4.4b, which emerged in late 2020 and is now widespread globally, especially in the Americas.
In the past, outbreaks could be controlled by culling of infected birds, and H5N1 would die down for a while. But this has become increasingly difficult due to escalating outbreaks since 2021.
Wild animals are now in the mix
Waterfowl (ducks, swans and geese) are the main global spreaders of avian flu, as they migrate across the world via specific routes that bypass Australia. The main hub for waterfowl to migrate around the world is Quinghai lake in China.
But there’s been an increasing number of infected non-waterfowl birds, such as true thrushes and raptors, which use different flyways. Worryingly, the infection has spread to Antarctica too, which means Australia is now at risk from different bird species which fly here.
H5N1 has escalated in an unprecedented fashion since 2021, and an increasing number of mammals including sea lions, goats, red foxes, coyotes, even domestic dogs and cats have become infected around the world.
Wild animals like red foxes which live in peri-urban areas are a possible new route of spread to farms, domestic pets and humans.
Dairy cows and goats have now become infected with H5N1 in at least 17 farms across seven US states.
What are the symptoms?
Globally, there have been 14 cases of H5N1 clade 2.3.4.4b virus in humans, and 889 H5N1 human cases overall since 2003.
Previous human cases have presented with a severe respiratory illness, but H5N1 2.3.4.4b is causing illness affecting other organs too, like the brain, eyes and liver.
For example, more recent cases have developed neurological complications including seizures, organ failure and stroke. It’s been estimated that around half of people infected with H5N1 will die.
The case in the Texan farm worker appears to be mild. This person presented with conjunctivitis, which is unusual.
Food safety
Contact with sick poultry is a key risk factor for human infection. Likewise, the farm worker in Texas was likely in close contact with the infected cattle.
The CDC advises pasteurised milk and well cooked eggs are safe. However, handling of infected meat or eggs in the process of cooking, or drinking unpasteurised milk, may pose a risk.
Although there’s no H5N1 in Australian poultry or cattle, hygienic food practices are always a good idea, as raw milk or poorly cooked meat, eggs or poultry can be contaminated with microbes such as salmonella and E Coli.
If it’s not a pandemic, why are we worried?
Scientists have feared avian influenza may cause a pandemic since about 2005. Avian flu viruses don’t easily spread in humans. But if an avian virus mutates to spread in humans, it can cause a pandemic.
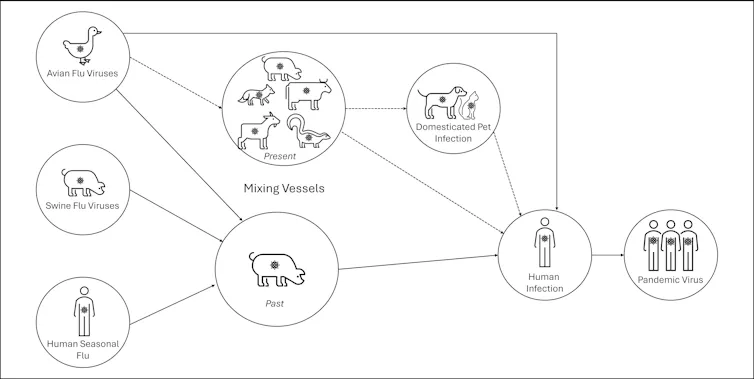
One concern is if birds were to infect an animal like a pig, this acts as a genetic mixing vessel. In areas where humans and livestock exist in close proximity, for example farms, markets or even in homes with backyard poultry, the probability of bird and human flu strains mixing and mutating to cause a new pandemic strain is higher.

There are a number of potential pathways to a pandemic caused by influenza. Author provided The cows infected in Texas were tested because farmers noticed they were producing less milk. If beef cattle are similarly affected, it may not be as easily identified, and the economic loss to farmers may be a disincentive to test or report infections.
How can we prevent a pandemic?
For now there is no spread of H5N1 between humans, so there’s no immediate risk of a pandemic.
However, we now have unprecedented and persistent infection with H5N1 clade 2.3.4.4b in farms, wild animals and a wider range of wild birds than ever before, creating more chances for H5N1 to mutate and cause a pandemic.
Unlike the previous epidemiology of avian flu, where hot spots were in Asia, the new hot spots (and likely sites of emergence of a pandemic) are in the Americas, Europe or in Africa.
Pandemics grow exponentially, so early warnings for animal and human outbreaks are crucial. We can monitor infections using surveillance tools such as our EPIWATCH platform.
The earlier epidemics can be detected, the better the chance of stamping them out and rapidly developing vaccines.
Although there is a vaccine for birds, it has been largely avoided until recently because it’s only partially effective and can mask outbreaks. But it’s no longer feasible to control an outbreak by culling infected birds, so some countries like France began vaccinating poultry in 2023.
For humans, seasonal flu vaccines may provide a small amount of cross-protection, but for the best protection, vaccines need to be matched exactly to the pandemic strain, and this takes time. The 2009 flu pandemic started in May in Australia, but the vaccines were available in September, after the pandemic peak.
To reduce the risk of a pandemic, we must identify how H5N1 is spreading to so many mammalian species, what new wild bird pathways pose a risk, and monitor for early signs of outbreaks and illness in animals, birds and humans. Economic compensation for farmers is also crucial to ensure we detect all outbreaks and avoid compromising the food supply.
C Raina MacIntyre, Professor of Global Biosecurity, NHMRC L3 Research Fellow, Head, Biosecurity Program, Kirby Institute, UNSW Sydney; Ashley Quigley, Senior Research Associate, Global Biosecurity, UNSW Sydney; Haley Stone, PhD Candidate, Biosecurity Program, Kirby Institute, UNSW Sydney; Matthew Scotch, Associate Dean of Research and Professor of Biomedical Informatics, College of Health Solutions, Arizona State University, and Rebecca Dawson, Research Associate, The Kirby Institute, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Can You Get Addicted To MSG, Like With Sugar?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝Hello, I love your newsletter 🙂 Can I have a question? While browsing through your recepies, I realised many contained MSG. As someone based in Europe, I am not used to using MSG while cooking (of course I know that processed food bought in supermarket containes MSG). There is a stigma, that MSG is not particulary healthy, but rather it should be really bad and cause negative effects like headaches. Is this true? Also, can you get addicted to MSG, just like you get addicted to sugar? Thank you :)❞
Thank you for the kind words, and the interesting questions!
Short answer: no and no 🙂
Longer answer: most of the negative reputation about MSG comes from a single piece of satire written in the US in the 1960s, which the popular press then misrepresented as a genuine concern, and the public then ran with, mostly due to racism/xenophobia/sinophobia specifically, given the US’s historically not fabulous relations with China, and the moniker of “Chinese restaurant syndrome”, notwithstanding that MSG was first isolated in Japan, not China, more than 100 years ago.
The silver lining that comes out of this is that because of the above, MSG has been one of the most-studied food additives in recent decades, with many teams of scientists in many countries trying to determine its risks and not finding any (except insofar as anything in extreme quantities can kill you, including water or oxygen).
You can read more about this and other* myths about MSG, here:
Monosodium Glutamate: Sinless Flavor-Enhancer Or Terrible Health Risk?
*such as pertaining to gluten sensitivity, which in reality MSG has no bearing on whatsoever as it does not contain gluten and is not even made of the same basic stuff; gluten being a protein made of (amongst other things) the amino acid glutamine, not a glutamate salt. Glutamate is as closely related to gluten as cyanocobalamin (vitamin B12) is to cyanide (the famous poison).
PS: if you didn’t click the above link to read that article, then 1) we really do recommend it 2) we did some LD50 calculations there and looked at available research, and found that for someone of this writer’s (very medium) size, eating 1kg of MSG at once is sufficient to cause toxicity, and injecting >250g of MSG may cause heart problems. So we don’t recommend doing that.
However, ½ tsp in a recipe that gives multiple portions is not going to get you anywhere close to the danger zone, unless you consume that entire meal by yourself hundreds of times per day. And if you do, the MSG is probably the least of your concerns.
(2 tsp of cassia cinnamon, however, is enough to cause coumarin toxicity; for this reason we recommend Ceylon (or “True” or “Sweet”) cinnamon in our recipes, as it has almost undetectable levels of coumarin)
With regard to your interesting question about addiction, first of all let’s speak briefly about sugar addiction:
Sugar addiction is, by broad scientific consensus, agreed-upon as an extant thing that does exist, and contemporary research is more looking into the “hows” and “whys” and “whats” rather than the “whether”. It is a somewhat complicated topic, because it’s halfway between what science would usually consider a chemical addiction, and what science would usually consider a behavioral addiction:
The Not-So-Sweet Science Of Sugar Addiction
The reasonable prevailing hypothesis, therefore, is that sugar simply has two moderate mechanisms of addiction, rather than one strong one.
The biochemical side of sugar addiction comes from the body’s metabolism of sugar, so this cannot be a thing for MSG, because there is nothing to metabolize in the same sense of the word (MSG being an inorganic compound with zero calories).
People can crave salt, especially when deficient in it, and MSG does contain sodium (it’s what the “S” stands for), but it contains a little under ⅓ of the sodium that table salt does (sodium chloride in whatever form, be it sea salt, rock salt, or such):
MSG vs. Salt: Sodium Comparison ← we do molecular calculations here!
Sea Salt vs MSG – Which is Healthier? ← this one for a head-to-head
However, even craving salt does not constitute an addiction; nobody is shamefully hiding their rock salt crystals under their bed and getting a fix when they feel low, and nor does withdrawal cause adverse side effects, except insofar as (once again) a person deficient in salt will crave salt.
Finally, the only other way we know of that one might wonder if MSG could be addictive, is about glutamate and glutamate receptors. The glutamate in MSG is the same glutamate (down to the atoms) as the glutamate formed if one consumes tomatoes in the presence of salt, and triggers the same glutamate receptors in the same way. We have the same number of receptors either way, and uptake is exactly the same (because again, it’s exactly the same chemical) so there is a maximum to how strong this effect can be, and that maximum is the same whatever the source of the glutamate was.
In this respect, if MSG is addictive, then so is a tomato salad with a pinch of salt: it’s not—it’s just tasty.
We haven’t cited papers in today’s article, but it’s just because we cited them already in the articles we linked, and so we avoided doubling up. Most of them are in that first link we gave 🙂
One final note
Technically anyone can develop a sensitivity to anything, so in theory someone could develop a sensitivity to MSG, just like they could for any other ingredient. Our usual legal/medical disclaimer applies.
However, it’s certainly not a common trigger, putting it well below common allergens like nuts (or less common allergens like, say, bananas), not even in the same league as common intolerances such as gluten, and less worthy of health risk warnings than, say, spinach (high in oxalates; fine for most people but best avoided if you have kidney problems).
The reason we use it in the recipes we use it in, is simply because it’s a lower-sodium alternative to salt, and while it contains a (very) tiny bit less sodium than low-sodium salt (which itself has about ⅓ the sodium of regular salt), it has more of a flavor-enhancing effect, such that one can use half as much, for a more than sixfold total sodium reduction. Which for most of us in the industrialized world, is beneficial.
Want to try some?
If today’s article has inspired you to give MSG a try, here’s an example product on Amazon 😎
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: