Elderhood – by Dr. Louise Aronson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Where does “middle age” end, and “old age” begin? By the United States’ CDC’s categorization, human life involves:
- 17 stages of childhood, deemed 0–18
- 5 stages of adulthood, deemed 18–60
- 1 stage of elderhood, deemed 60+
Isn’t there something missing here? Do we just fall off some sort of conveyor belt on our sixtieth birthdays, into one big bucket marked “old”?
Yesterday you were 59 and enjoying your middle age; today you have, apparently, the same medical factors and care needs as a 114-year-old.
Dr. Louise Aronson, a geriatrician, notes however that medical science tends to underestimate the differences found in more advanced old age, and underresearch them. That elders consume half of a country’s medicines, but are not required to be included in clinical trials. That side effects not only are often different than for younger adults, but also can cause symptoms that are then dismissed as “Oh she’s just old”.
She explores, mostly through personal career anecdotes, the well-intentioned disregard that is frequently given by the medical profession, and—importantly—how we might overcome that, as individuals and as a society.
Bottom line: if you are over the age of 60, love someone over the age of 60, this is a book for you. Similarly if you and/or they plan to live past the age of 60, this is also a book for you.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

War in Ukraine affected wellbeing worldwide, but people’s speed of recovery depended on their personality

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The war in Ukraine has had impacts around the world. Supply chains have been disrupted, the cost of living has soared and we’ve seen the fastest-growing refugee crisis since World War II. All of these are in addition to the devastating humanitarian and economic impacts within Ukraine.
Our international team was conducting a global study on wellbeing in the lead up to and after the Russian invasion. This provided a unique opportunity to examine the psychological impact of the outbreak of war.
As we explain in a new study published in Nature Communications, we learned the toll on people’s wellbeing was evident across nations, not just in Ukraine. These effects appear to have been temporary – at least for the average person.
But people with certain psychological vulnerabilities struggled to recover from the shock of the war.
Tracking wellbeing during the outbreak of war
People who took part in our study completed a rigorous “experience-sampling” protocol. Specifically, we asked them to report their momentary wellbeing four times per day for a whole month.
Data collection began in October 2021 and continued throughout 2022. So we had been tracking wellbeing around the world during the weeks surrounding the outbreak of war in February 2022.
We also collected measures of personality, along with various sociodemographic variables (including age, gender, political views). This enabled us to assess whether different people responded differently to the crisis. We could also compare these effects across countries.
Our analyses focused primarily on 1,341 participants living in 17 European countries, excluding Ukraine itself (44,894 experience-sampling reports in total). We also expanded these analyses to capture the experiences of 1,735 people living in 43 countries around the world (54,851 experience-sampling reports) – including in Australia.
A global dip in wellbeing
On February 24 2022, the day Russia invaded Ukraine, there was a sharp decline in wellbeing around the world. There was no decline in the month leading up to the outbreak of war, suggesting the change in wellbeing was not already occurring for some other reason.
However, there was a gradual increase in wellbeing during the month after the Russian invasion, suggestive of a “return to baseline” effect. Such effects are commonly reported in psychological research: situations and events that impact our wellbeing often (though not always) do so temporarily.
Unsurprisingly, people in Europe experienced a sharper dip in wellbeing compared to people living elsewhere around the world. Presumably the war was much more salient for those closest to the conflict, compared to those living on an entirely different continent.
Interestingly, day-to-day fluctuations in wellbeing mirrored the salience of the war on social media as events unfolded. Specifically, wellbeing was lower on days when there were more tweets mentioning Ukraine on Twitter/X.
Our results indicate that, on average, it took around two months for people to return to their baseline levels of wellbeing after the invasion.
Different people, different recoveries
There are strong links between our wellbeing and our individual personalities.
However, the dip in wellbeing following the Russian invasion was fairly uniform across individuals. None of the individual factors assessed in our study, including personality and sociodemographic factors, predicted people’s response to the outbreak of war.
On the other hand, personality did play a role in how quickly people recovered. Individual differences in people’s recovery were linked to a personality trait called “stability”. Stability is a broad dimension of personality that combines low neuroticism with high agreeableness and conscientiousness (three traits from the Big Five personality framework).
Stability is so named because it reflects the stability of one’s overall psychological functioning. This can be illustrated by breaking stability down into its three components:
- low neuroticism describes emotional stability. People low in this trait experience less intense negative emotions such as anxiety, fear or anger, in response to negative events
- high agreeableness describes social stability. People high in this trait are generally more cooperative, kind, and motivated to maintain social harmony
- high conscientiousness describes motivational stability. People high in this trait show more effective patterns of goal-directed self-regulation.
So, our data show that people with less stable personalities fared worse in terms of recovering from the impact the war in Ukraine had on wellbeing.
In a supplementary analysis, we found the effect of stability was driven specifically by neuroticism and agreeableness. The fact that people higher in neuroticism recovered more slowly accords with a wealth of research linking this trait with coping difficulties and poor mental health.
These effects of personality on recovery were stronger than those of sociodemographic factors, such as age, gender or political views, which were not statistically significant.
Overall, our findings suggest that people with certain psychological vulnerabilities will often struggle to recover from the shock of global events such as the outbreak of war in Ukraine.

Luke Smillie, Professor in Personality Psychology, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
How we can prepare for future public health emergencies
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The U.S. is experiencing an increasing number of disease outbreaks and extreme weather events. While state and national preparedness for public health emergencies has improved in some areas, dangerous gaps remain, says a recent report from Trust for America’s Health.
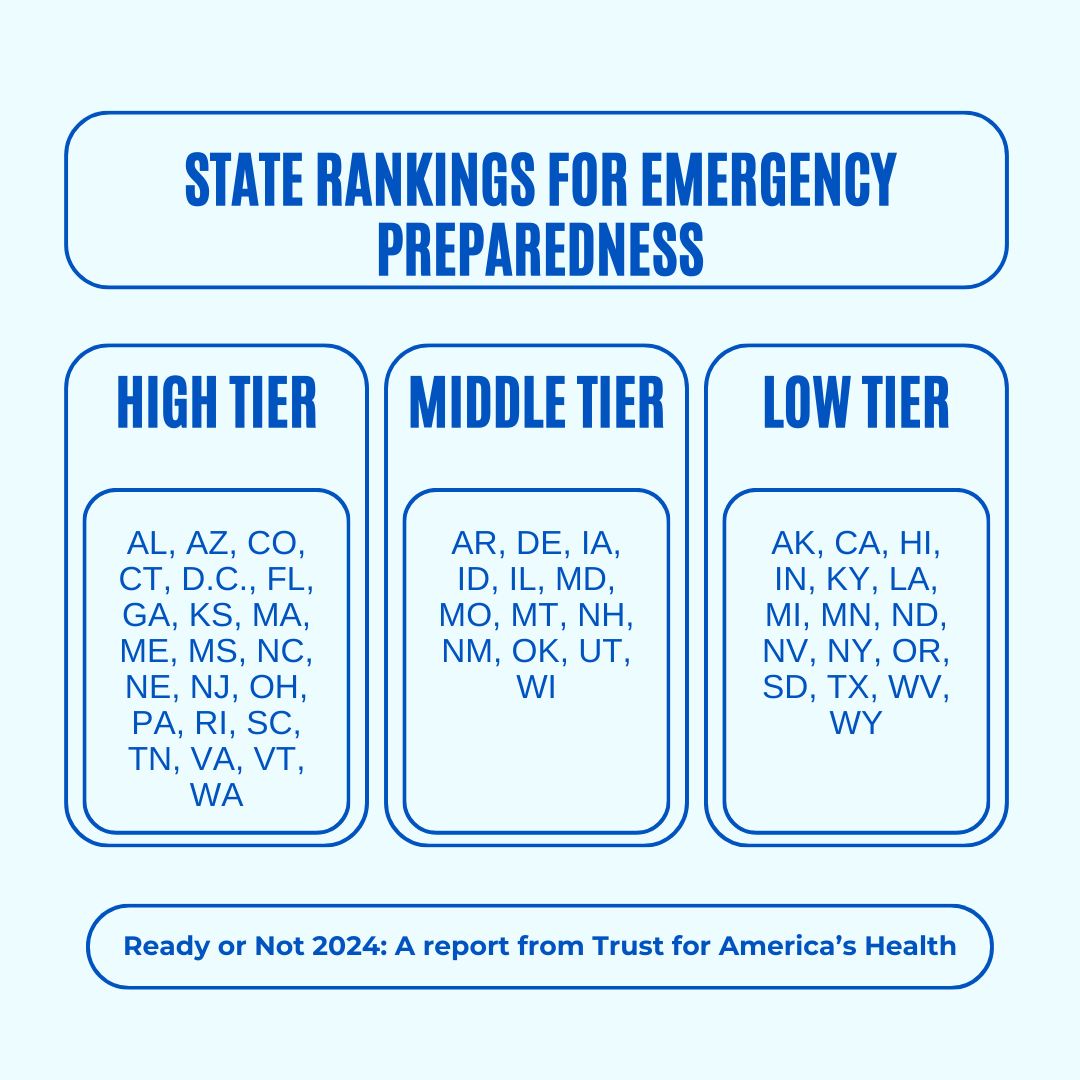
Titled, “Ready or Not 2024: Protecting the Public’s Health from Diseases, Disasters, and Bioterrorism,” the report identifies gaps in national and state preparedness for public health emergencies and provides recommendations for improvement.
Using nine key indicators, the report categorizes all U.S. states and the District of Columbia into three readiness levels: high, medium, and low. The writers hope the report will help policymakers in under-performing states improve public health infrastructure.
Read on to learn more about what the research found and how we can individually prepare for future public health emergencies.
There’s work to be done

The report highlights areas with strong performance as well as those that need improvement.
Some areas with strong performance:
- State public health funding: Most states and the District of Columbia either maintained or increased their public health funding during the 2023 fiscal year.
- Health care labor force preparedness: Most states have started expanding the health care labor force for improved emergency response. As of 2023, 39 states participated in the Nurse Licensure Compact, which allows nurses to work in multiple member states without the need for additional state licenses.
Some areas that need improvement:
- Hospital safety scores: Only 25 percent of acute care hospitals earned the highest patient safety grade in fall 2023. These scores measure health care-associated infection rates, intensive care unit capacity, and other metrics. More high-scoring hospitals would improve preparedness for future public health emergencies.
- Access to paid time off: From March 2018 to March 2023, only 55 percent of U.S. workers used paid time off. Access to paid time off is important for reducing the spread of infectious diseases.
We can all do our part by staying up to date on vaccines
While the report focuses on policy changes that would improve emergency preparedness, Trust for America’s Health’s research identifies one way that we can individually prepare for future public health emergencies: staying up to date on vaccines.
The report found that during the 2022-2023 flu season, only 49 percent of those eligible for the flu vaccine received it. Public health experts are concerned that false claims about COVID-19 vaccines have resulted in overall vaccine hesitancy.
A decline in vaccination rates has led to an uptick in life-threatening, vaccine-preventable diseases, such as measles. Increasing vaccine uptake would prevent the spread of vaccine-preventable diseases and reduce strain on hospital systems during public health crises.
Make sure that you and your children have received all recommended vaccines to prevent severe illness, hospitalization, and death. Learn more about recommended vaccines for adults and children from the CDC.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Share This Post
-

Diet Tips for Crohn’s Disease
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝Doctors are great at saving lives like mine. I’m a two time survivor of colon cancer and have recently been diagnosed with Chron’s disease at 62. No one is the health system can or is prepared to tell me an appropriate diet to follow or what to avoid. Can you?❞
Congratulations on the survivorship!
As to Crohn’s, that’s indeed quite a pain, isn’t it? In some ways, a good diet for Crohn’s is the same as a good diet for most other people, with one major exception: fiber
…and unfortunately, that changes everything, in terms of a whole-foods majority plant-based diet.
What stays the same:
- You still ideally want to eat a lot of plants
- You definitely want to avoid meat and dairy in general
- Eating fish is still usually* fine, same with eggs
- Get plenty of water
What needs to change:
- Consider swapping grains for potatoes or pasta (at least: avoid grains)
- Peel vegetables that are peelable; discard the peel or use it to make stock
- Consider steaming fruit and veg for easier digestion
- Skip spicy foods (moderate spices, like ginger, turmeric, and black pepper, are usually fine in moderation)
Much of this latter list is opposite to the advice for people without Crohn’s Disease.
*A good practice, by the way, is to keep a food journal. There are apps that you can get for free, or you can do it the old-fashioned way on paper if prefer.
But the important part is: make a note not just of what you ate, but also of how you felt afterwards. That way, you can start to get a picture of patterns, and what’s working (or not) for you, and build up a more personalized set of guidelines than anyone else could give to you.
We hope the above pointers at least help you get going on the right foot, though!
Share This Post


Related Posts
-
Palliative care as a true art form
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How do you ease the pain from an ailment amidst lost words? How can you serve the afflicted when lines start to blur? When the foundation of communication begins to crumble, what will be the pillar health-care professionals can lean on to support patients afflicted with dementia during their final days?
The practice of medicine is both highly analytical and evidence based in nature. However, it is considered a “practice” because at the highest level, it resembles a musician navigating an instrument. It resembles art. Between lab values, imaging techniques and treatment options, the nuances for individualized patient care so often become threatened.
Dementia, a non-malignant terminal illness, involves the progressive cognitive and social decline in those afflicted. Though there is no cure, dementia is commonly met in the setting of end-of-life care. During this final stage of life, the importance of comfort via symptomatic management and communication usually is a priority in patient care. But what about the care of a patient suffering from dementia? While communication serves as the vehicle to deliver care at a high level, medical professionals are suddenly met with a roadblock. And there … behind the pieces of shattered communication and a dampened map of ethical guidelines, health-care providers are at a standstill.
It’s 4:37 a.m. You receive a text message from the overnight nurse at a care facility regarding a current seizure. After lorazepam is ordered and administered, Mr. H, a quick-witted 76-year-old, stabilizes. Phenobarbital 15mg SC qhs was also added to prevent future similar events. You exhale a sigh of relief.
Mr. H. has been admitted to the floor 36 hours earlier after having a seizure while playing poker with colleagues. Since he became your patient, he’s shared many stories from professional and family life with you, along with as many jokes as he could fit in between. However, over the course of the next seven days, Mr. H. would develop aspiration pneumonia, progressing to ventilator dependency and, ultimately, multi-organ failure with rapid cognitive decline.
What strategies and tools would you use to maximize the well-being of your patient during his decline? How would you bridge the gap of understanding between the patient’s family and health-care team to provide the standard of care that all patients are owed?
To give Mr. H. the type of care he would have wanted, upon his hospital admission, he should have been questioned about his understanding of illness along with the goals of care of the medical team. The patient should have been informed that it is imperative to adhere to the medical regimen implemented by his team along with the risks of not doing so. In the event disease-related complications arose, advanced directives should have been documented to avoid any unnecessary measures.
It is important to note, that with each change in status of the patient’s health status, the goal of treatment must be reassessed. The patient or surrogate decision-maker’s understanding of these goals is paramount in maintaining the patient’s autonomy. It is often said that effective communication is the bedrock of a healthy relationship. This is true regardless of type of relationship.
This is why I and Megan Vierhout wrote Integrated End of Life Care in Dementia: A Comprehensive Guide, a book targeted at providing a much-needed road map to navigate the many challenges involved in end-of-life care for individuals with dementia. Ultimately, our aim is to provide a compass for both health-care professionals and the families of those affected by the progressive effects of dementia. We provide practical advice on optimizing communication with individuals with dementia while taking their cognitive limitations, preferences and needs into account.
I invite you to explore the unpredictable terrain of end-of-life care for patients with dementia. Together, we can pave a smoother, sturdier path toward the practice of medicine as a true art form.
This article is republished from healthydebate under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

More Salt, Not Less?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝I’m curious about the salt part – learning about LMNT and what they say about us needing more salt than what’s recommended by the government, would you mind looking into that? From a personal experience, I definitely noticed a massive positive difference during my 3-5 day water fasts when I added salt to my water compared to when I just drank water. So I’m curious what the actual range for salt intake is that we should be aiming for.❞
That’s a fascinating question, and we’ll have to tackle it in several parts:
When fasting
3–5 days is a long time to take only water; we’re sure you know most people fast from food for much less time than that. Nevertheless, when fasting, the body needs more water than usual—because of the increase in metabolism due to freeing up bodily resources for cellular maintenance. Water is necessary when replacing cells (most of which are mostly water, by mass), and for ferrying nutrients around the body—as well as escorting unwanted substances out of the body.
Normally, the body’s natural osmoregulatory process handles this, balancing water with salts of various kinds, to maintain homeostasis.
However, it can only do that if it has the requisite parts (e.g. water and salts), and if you’re fasting from food, you’re not replenishing lost salts unless you supplement.
Normally, monitoring our salt intake can be a bit of a guessing game, but when fasting for an entire day, it’s clear how much salt we consumed in our food that day: zero
So, taking the recommended amount of sodium, which varies but is usually in the 1200–1500mg range (low end if over aged 70+; high end if aged under 50), becomes sensible.
More detail: How Much Sodium You Need Per Day
See also, on a related note:
When To Take Electrolytes (And When We Shouldn’t!)
When not fasting
Our readers here are probably not “the average person” (since we have a very health-conscious subscriber-base), but the average person in N. America consumes about 9g of salt per day, which is several multiples of the maximum recommended safe amount.
The WHO recommends no more than 5g per day, and the AHA recommends no more than 2.3g per day, and that we should aim for 1.5g per day (this is, you’ll note, consistent with the previous “1200–1500mg range”).
Read more: Massive efforts needed to reduce salt intake and protect lives
Questionable claims
We can’t speak for LMNT (and indeed, had to look them up to discover they are an electrolytes supplement brand), but we can say that sometimes there are articles about such things as “The doctor who says we should eat more salt, not less”, and that’s usually about Dr. James DiNicolantonio, a doctor of pharmacy, who wrote a book that, because of this question today, we’ve now also reviewed:
Spoiler, our review was not favorable.
The body knows
Our kidneys (unless they are diseased or missing) do a full-time job of getting rid of excess things from our blood, and dumping them into one’s urine.
That includes excess sugar (which is how diabetes was originally diagnosed) and excess salt. In both cases, they can only process so much, but they do their best.
Dr. DiNicolantino recognizes this in his book, but chalks it up to “if we do take too much salt, we’ll just pass it in urine, so no big deal”.
Unfortunately, this assumes that our kidneys have infinite operating capacity, and they’re good, but they’re not that good. They can only filter so much per hour (it’s about 1 liter of fluids). Remember we have about 5 liters of blood, consume 2–3 liters of water per day, and depending on our diet, several more liters of water in food (easy to consume several more liters of water in food if one eats fruit, let alone soups and stews etc), and when things arrive in our body, the body gets to work on them right away, because it doesn’t know how much time it’s going to have to get it done, before the next intake comes.
It is reasonable to believe that if we needed 8–10g of salt per day, as Dr. DiNicolantonio claims, our kidneys would not start dumping once we hit much, much lower levels in our blood (lower even than the daily recommended intake, because not all of the salt in our body is in our blood, obviously).
See also: How Too Much Salt Can Lead To Organ Failure
Lastly, a note about high blood pressure
This is one where the “salt’s not the bad guy” crowd have at least something close to a point, because while salt is indeed still a bad guy (if taken above the recommended amounts, without good medical reason), when it comes to high blood pressure specifically, it’s not the worst bad guy, nor is it even in the top 5:
Hypertension: Factors Far More Relevant Than Salt
Thanks for writing in with such an interesting question!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Health Simplified – by Daniel Cottmeyer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Health Simplified – by Daniel Cottmeyer
A lot of books focus on the most marketable aspects of health, such as fat loss or muscle gain. Instead, Cottmeyer takes a “birds-eye-view” of health in all its aspects, and then boils it down to the most critical key parts.
Rather than giving a science-dense tome that nobody reads, or a light motivational piece that everyone reads but it amounts to “you can do it!”, here we get substance… but in a digestible form.
Which we at 10almonds love.
The book presents a simple action plan to:
- Improve your relationship with food/exercise
- Actually get better sleep
- Understand how nutrition really works
- Set up helpful habits that are workable and sustainable
- Bring these components together synergistically
Bottom line: if you’re going to buy only one health/fitness book, this is a fine contender.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: