Migraine Mythbusting
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Migraine: When Headaches Are The Tip Of The Neurological Iceberg
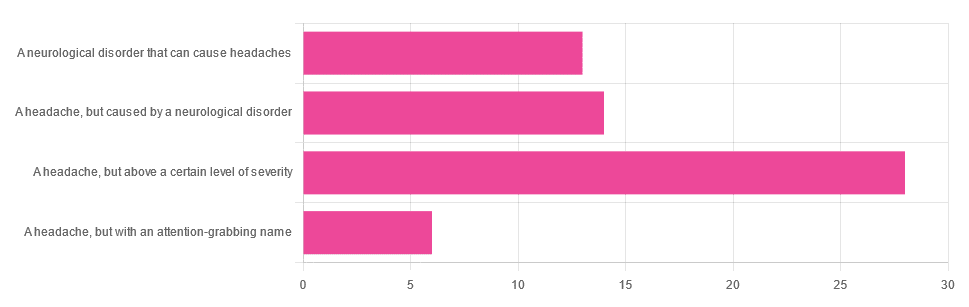
Yesterday, we asked you “What is a migraine?” and got the above-depicted, below-described spread of responses:
- Just under 46% said “a headache, but above a certain level of severity”
- Just under 23% said “a headache, but caused by a neurological disorder”
- Just over 21% said “a neurological disorder that can cause headaches”
- Just under 10% said “a headache, but with an attention-grabbing name”
So… What does the science say?
A migraine is a headache, but above a certain level of severity: True or False?
While that’s usually a very noticeable part of it… That’s only one part of it, and not a required diagnostic criterion. So, in terms of defining what a migraine is, False.
Indeed, migraine may occur without any headache, let alone a severe one, for example: Abdominal Migraine—though this is much less well-researched than the more common with-headache varieties.
Here are the defining characteristics of a migraine, with the handy mnemonic 5-4-3-2-1:
- 5 or more attacks
- 4 hours to 3 days in duration
- 2 or more of the following:
- Unilateral (affects only one side of the head)
- Pulsating
- Moderate or severe pain intensity
- Worsened by or causing avoidance of routine physical activity
- 1 or more of the following:
- Nausea and/or vomiting
- Sensitivity to both light and sound
Source: Cephalalgia | ICHD-II Classification: Parts 1–3: Primary, Secondary and Other
As one of our subscribers wrote:
❝I have chronic migraine, and it is NOT fun. It takes away from my enjoyment of family activities, time with friends, and even enjoying alone time. Anyone who says a migraine is just a bad headache has not had to deal with vertigo, nausea, loss of balance, photophobia, light sensitivity, or a host of other symptoms.❞
Migraine is a neurological disorder: True or False?
True! While the underlying causes aren’t known, what is known is that there are genetic and neurological factors at play.
❝Migraine is a recurrent, disabling neurological disorder. The World Health Organization ranks migraine as the most prevalent, disabling, long-term neurological condition when taking into account years lost due to disability.
Considerable progress has been made in elucidating the pathophysiological mechanisms of migraine, associated genetic factors that may influence susceptibility to the disease❞
Source: JHP | Mechanisms of migraine as a chronic evolutive condition
Migraine is just a headache with a more attention-grabbing name: True or False?
Clearly, False.
As we’ve already covered why above, we’ll just close today with a nod to an old joke amongst people with chronic illnesses in general:
“Are you just saying that because you want attention?”
“Yes… Medical attention!”
Want to learn more?
You can find a lot of resources at…
NIH | National Institute of Neurological Disorders & Stroke | Migraine
and…
The Migraine Trust ← helpfully, this one has a “Calm mode” to tone down the colorscheme of the website!
Particularly useful from the above site are its pages:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Alzheimer’s may have once spread from person to person, but the risk of that happening today is incredibly low

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
An article published this week in the prestigious journal Nature Medicine documents what is believed to be the first evidence that Alzheimer’s disease can be transmitted from person to person.
The finding arose from long-term follow up of patients who received human growth hormone (hGH) that was taken from brain tissue of deceased donors.
Preparations of donated hGH were used in medicine to treat a variety of conditions from 1959 onwards – including in Australia from the mid 60s.
The practice stopped in 1985 when it was discovered around 200 patients worldwide who had received these donations went on to develop Creuztfeldt-Jakob disease (CJD), which causes a rapidly progressive dementia. This is an otherwise extremely rare condition, affecting roughly one person in a million.
What’s CJD got to do with Alzehimer’s?
CJD is caused by prions: infective particles that are neither bacterial or viral, but consist of abnormally folded proteins that can be transmitted from cell to cell.
Other prion diseases include kuru, a dementia seen in New Guinea tribespeople caused by eating human tissue, scrapie (a disease of sheep) and variant CJD or bovine spongiform encephalopathy, otherwise known as mad cow disease. This raised public health concerns over the eating of beef products in the United Kingdom in the 1980s.
Human growth hormone used to come from donated organs
Human growth hormone (hGH) is produced in the brain by the pituitary gland. Treatments were originally prepared from purified human pituitary tissue.
But because the amount of hGH contained in a single gland is extremely small, any single dose given to any one patient could contain material from around 16,000 donated glands.
An average course of hGH treatment lasts around four years, so the chances of receiving contaminated material – even for a very rare condition such as CJD – became quite high for such people.
hGH is now manufactured synthetically in a laboratory, rather than from human tissue. So this particular mode of CJD transmission is no longer a risk.

Human growth hormone is now produced in a lab.
National Cancer Institute/UnsplashWhat are the latest findings about Alzheimer’s disease?
The Nature Medicine paper provides the first evidence that transmission of Alzheimer’s disease can occur via human-to-human transmission.
The authors examined the outcomes of people who received donated hGH until 1985. They found five such recipients had developed early-onset Alzheimer’s disease.
They considered other explanations for the findings but concluded donated hGH was the likely cause.
Given Alzheimer’s disease is a much more common illness than CJD, the authors presume those who received donated hGH before 1985 may be at higher risk of developing Alzheimer’s disease.
Alzheimer’s disease is caused by presence of two abnormally folded proteins: amyloid and tau. There is increasing evidence these proteins spread in the brain in a similar way to prion diseases. So the mode of transmission the authors propose is certainly plausible.
However, given the amyloid protein deposits in the brain at least 20 years before clinical Alzheimer’s disease develops, there is likely to be a considerable time lag before cases that might arise from the receipt of donated hGH become evident.
When was this process used in Australia?
In Australia, donated pituitary material was used from 1967 to 1985 to treat people with short stature and infertility.
More than 2,000 people received such treatment. Four developed CJD, the last case identified in 1991. All four cases were likely linked to a single contaminated batch.
The risks of any other cases of CJD developing now in pituitary material recipients, so long after the occurrence of the last identified case in Australia, are considered to be incredibly small.
Early-onset Alzheimer’s disease (defined as occurring before the age of 65) is uncommon, accounting for around 5% of all cases. Below the age of 50 it’s rare and likely to have a genetic contribution.
Early onset Alzheimer’s means it occurs before age 65.
perfectlab/ShutterstockThe risk is very low – and you can’t ‘catch’ it like a virus
The Nature Medicine paper identified five cases which were diagnosed in people aged 38 to 55. This is more than could be expected by chance, but still very low in comparison to the total number of patients treated worldwide.
Although the long “incubation period” of Alzheimer’s disease may mean more similar cases may be identified in the future, the absolute risk remains very low. The main scientific interest of the article lies in the fact it’s first to demonstrate that Alzheimer’s disease can be transmitted from person to person in a similar way to prion diseases, rather than in any public health risk.
The authors were keen to emphasise, as I will, that Alzheimer’s cannot be contracted via contact with or providing care to people with Alzheimer’s disease.

Steve Macfarlane, Head of Clinical Services, Dementia Support Australia, & Associate Professor of Psychiatry, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Blackberries vs Grapes – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing blackberries to grapes, we picked the blackberries.
Why?
It’s not even close:
In terms of macros, blackberries have more than 5x the fiber, for about half the carbs, resulting in a notably lower glycemic index. They also have more than 2x the protein, but unlike the fiber, it’s not much in either fruit, so we might disregard it. Still, an easy win for blackberries either way.
In the category of vitamins, blackberries have more of vitamins A, B3, B5, B9, C, E, K, and choline, while grapes have more of vitamins B1, B2, and B6. Another clear win for blackberries.
When it comes to minerals, blackberries have a lot more calcium, copper, iron, magnesium, phosphorus, selenium, and zinc, while grapes have slightly more manganese and potassium. Once again, blackberries emerge victorious.
Looking at polyphenols, both have an abundance of many polyphenols, but blackberries have more, both in types and in total mass (mg/100g).
Thus, blackberries overwhelmingly win the day, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
Can We Drink To Good Health? ← while there are polyphenols such as resveratrol in red wine that per se would boost heart health, there’s so little per glass that you may need 100–1000 glasses per day to get the dosage that provides benefits in mouse studies.
If you’re not a mouse, you might even need more than that!
To this end, many people prefer resveratrol supplementation ← link is to an example product on Amazon, but there are plenty more so feel free to shop around 😎
Enjoy!
Share This Post
-

Loving Life at 50+ – by Maria Sabando
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What a pleasant mix of a book! Sabando writes about aging with a great blend of light-heartedness and seriousness, and gives extra attention to the important balancing act of:
- Indulging sufficiently to enjoy life
- Staying well enough to enjoy life
…because one without the other will not generally result in an enjoyable life! An American proud of her Italian heritage, she blends (as many immigrant families do) cultures and perspectives, aiming where she can for “the best of both” in that regard, too.
Nor is this just a philosophical book—there’s yoga to be learned here, chapter by chapter, and recipes peppered throughout. The recipes, by the way, are simple and… Honestly, not as healthy as the recipes we share here at 10almonds, but they are good and when it comes to those indulgences we mentioned, her philosophy is that strategic mindful indulgence keeps mindless binge-eating at bay. Which is generally speaking not a bad approach, and is one we’ve written about before as well.
When it comes to health advice, the author is no doctor or scientist, but her husband (a doctor) had input throughout, keeping things on track and medically sound.
The style is very casual, like talking to a friend, which makes for a very easy and enjoyable read. Absolutely a book that one could read casually in the garden, put down when interrupted, pick up again, and continue happily where one left off.
Bottom line: whatever your age (no matter whether your 50th birthday is in your shrinkingly near future or your increasingly distant past), there’s wisdom to be gained here—it’s not a manual (unless you want to treat it as one), it’s more… Thought-provoking, from cover to cover. Highly recommendable.
Click here to check out Loving Life at 50+, and love life at 50+!
Share This Post



Related Posts
-
How Old Is Too Old For HRT?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝I think you guys do a great job. Wondering if I can suggest a topic? Older women who were not offered hormone replacement therepy because of a long term study that was misread. Now, we need science to tell us if we are too old to benefit from begininng to take HRT. Not sure how old your readers are on average but it would be a great topic for older woman. Thanks❞
Thank you for the kind words, and the topic suggestion!
About the menopause and older age thereafter
We’ve talked a bit before about the menopause, for example:
What You Should Have Been Told About The Menopause Beforehand
And we’ve even discussed the unfortunate social phenomenon of post-menopausal women thinking “well, that’s over and done with now, time to forget about that”, because spoiler, it will never be over and done with—your body is always changing every day, and will continue to do so until you no longer have a body to change.
This means, therefore, that since changes are going to happen no matter what, the onus is on us to make the changes as positive (rather than negative) as possible:
Menopause, & When Not To Let Your Guard Down
About cancer risk
It sounds like you know this one, but for any who were unaware: indeed, there was an incredibly overblown and misrepresented study, and even that was about older forms of HRT (being conjugated equine estrogens, instead of bioidentical estradiol):
As for those who have previously had breast cancer or similar, there is also:
The Hormone Therapy That Reduces Breast Cancer Risk & More
Is it too late?
Fortunately, there is a quick and easy test to know whether you are too old to benefit:
First, find your pulse, by touching the first two fingers of one hand, against the wrist of the other. If you’re unfamiliar with where to find the pulse at the wrist, here’s a quick explainer.
Or if you prefer a video:
Click Here If The Embedded Video Doesn’t Load Automatically!
Did you find it?
Good; in that case, it’s not too late!
Scientists have tackled this question, looking at women of various ages, and finding that when comparing age groups taking HRT, disease risk changes do not generally vary much by age i.e., someone at 80 gets the same relative benefit from HRT as someone at 50, with no extra risks from the HRT. For example, if taking HRT at 50 reduces a risk by n% compared to an otherwise similar 50-year-old not on HRT, then doing so at 80 reduces the same risk by approximately the same percentage, compared to an otherwise similar 80-year-old not on HRT.
There are a couple of exceptions, such as in the case of already having advanced atherosclerotic lesions (in which specific case HRT could increase inflammation; not something it usually does), or in the case of using conjugated equine estrogens instead of modern bioidentical estradiol (as we talked about before).
Thus, for the most part, HRT is considered safe and effective regardless of age:
How old is too old for hormone therapy?
👆 that’s from 2015 though, so how about a new study, from 2024?
❝Compared with never use or discontinuation of menopausal hormone therapy after age 65 years, the use of estrogen monotherapy beyond age 65 years was associated with significant risk reductions in mortality (19% or adjusted hazards ratio, 0.81; 95% CI, 0.79-0.82), breast cancer (16%), lung cancer (13%), colorectal cancer (12%), congestive heart failure (CHF) (5%), venous thromboembolism (3%), atrial fibrillation (4%), acute myocardial infarction (11%), and dementia (2%).❞
❝Among senior Medicare women, the implications of menopausal hormone therapy use beyond age 65 years vary by types, routes, and strengths. In general, risk reductions appear to be greater with low rather than medium or high doses, vaginal or transdermal rather than oral preparations, and with estradiol rather than conjugated estrogen.❞
Read in full: Use of menopausal hormone therapy beyond age 65 years and its effects on women’s health outcomes by types, routes, and doses
As for more immediately-enjoyable benefits (improved mood, healthier skin, better sexual function, etc), yes, those also are benefits that people enjoy at least into their eighth decade:
See: Use of hormone therapy in Swedish women aged 80 years or older
What about…
Statistically speaking, most people who take HRT have a great time with it and consider it life-changing in a good way. However, nothing is perfect; sometimes going on HRT can have a shaky start, and for those people, there may be some things that need addressing. So for that, check out:
HRT Side Effects & Troubleshooting
And also, while estrogen monotherapy is very common, it is absolutely worthwhile to consider also taking progesterone alongside it:
Progesterone Menopausal HRT: When, Why, And How To Benefit
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

High-Protein Paneer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Paneer (a kind of Desi cheese used in many recipes from that region) is traditionally very high in fat, mostly saturated. Which is delicious, but not exactly the most healthy.
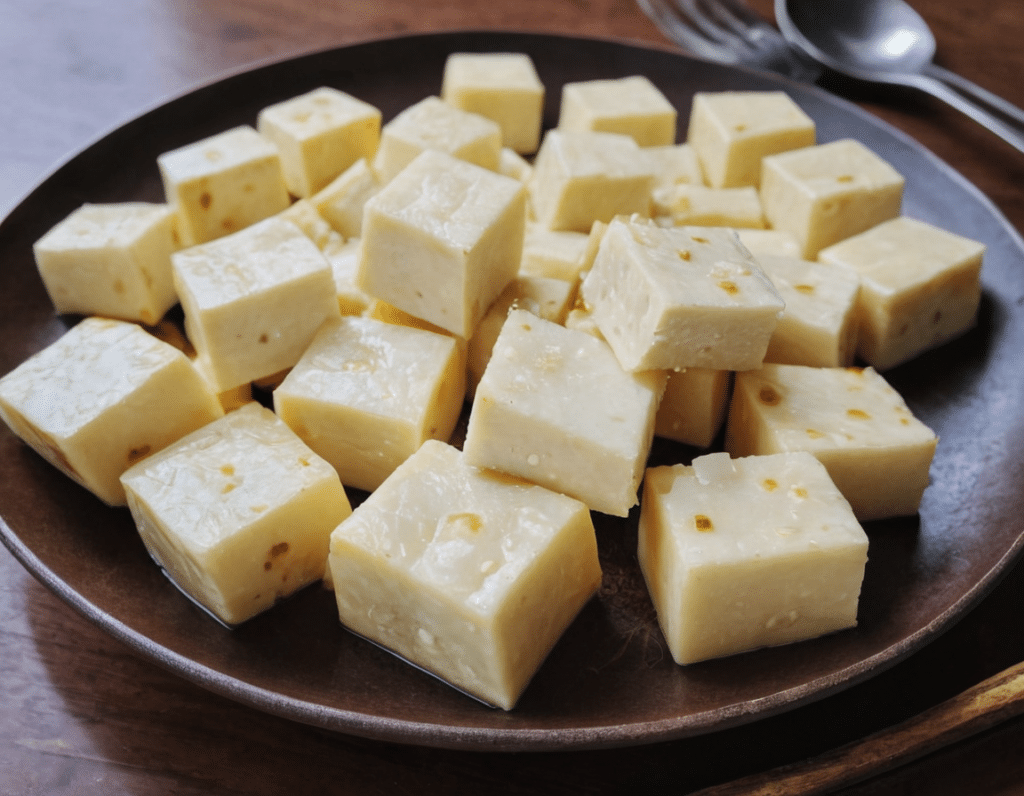
Today we’ll be making a plant-based paneer that does exactly the same jobs (has a similar texture and gentle flavor, takes on the flavors of dishes in the same way, etc) but with a fraction of the fat (of which only a trace amount is saturated, in this plant-based version), and even more protein. We’ll use this paneer in some recipes in the future, but it can be enjoyed by itself already, so let’s get going…
You will need
- ½ cup gram flour (unwhitened chickpea flour)
- Optional: 1 tsp low-sodium salt
Method
(we suggest you read everything at least once before doing anything)
1) Whisk the flour (and salt, if using) with 2 cups water in a big bowl, whisking until the texture is smooth.
2) Transfer to a large saucepan on a low-to-medium heat; you want it hot, but not quite a simmer. Keep whisking until the mixture becomes thick like polenta. This should take 10–15 minutes, so consider having someone else to take shifts if the idea of whisking continually for that long isn’t reasonable to you.
3) Transfer to a non-stick baking tin that will allow you to pour it about ½” deep. If the tin’s too large, you can always use a spatula to push it up against two or three sides, so that it’s the right depth
3) Refrigerate for at least 10 minutes, but longer is better if you have the time.
4) When ready to serve/use, cut it into ½” cubes. These can be served/used now, or kept for about a week in the fridge.
Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Menopause: 50 Things You Need to Know – by Dr. Felice Gersh
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Can you list 50 important facts about the menopause? If not, you’ll surely find things to learn in here.
The book is divided into three main sections:
- What to expect in perimenopause
- What to expect in early menopause
- What to expect in late menopause
Each section comes with an alarming array of symptoms, ranging from perimenopause fatigue and acne to late menopause tooth loss and vaginal prolapse. This is not to say that everyone will experience everything (fortunately), but rather, that these are the things that can happen and should not arrive unexpected.
Helpfully, of course, Dr. Gersh also gives advice on how to improve your energy and skin health, as well as keep your teeth and vagina in place. And similar professional insights for the rest of the “50 things you need to know”.
The style is like one big (182 pages) patient information leaflet—thus, very clear, explaining everything, and offering reassurance where possible and also what things are reasonable cause for seeking personalized medical attention.
Bottom line: if menopause is in your future, present, or very near past, this is an excellent book for you.
Click here to check out Menopause: 50 Things You Need To Know, and know them!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: