Yes, we still need chickenpox vaccines
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For people who grew up before a vaccine was available, chickenpox is largely remembered as an unpleasant experience that almost every child suffered through. The highly contagious disease tore through communities, leaving behind more than a few lasting scars.
For many children, chickenpox was much more than a week or two of itchy discomfort. It was a serious and sometimes life-threatening infection.
Prior to the chickenpox vaccine’s introduction in 1995, 90 percent of children got chickenpox. Those children grew into adults with an increased risk of developing shingles, a disease caused by the same virus—varicella-zoster—as chickenpox, which lies dormant in the body for decades.
The vaccine changed all that, nearly wiping out chickenpox in the U.S. in under three decades. The vaccine has been so successful that some people falsely believe the disease no longer exists and that vaccination is unnecessary. This couldn’t be further from the truth.
Vaccination spares children and adults from the misery of chickenpox and the serious short- and long-term risks associated with the disease. The CDC estimates that 93 percent of children in the U.S. are fully vaccinated against chickenpox. However, outbreaks can still occur among unvaccinated and under-vaccinated populations.
Here are some of the many reasons why we still need chickenpox vaccines.
Chickenpox is more serious than you may remember
For most children, chickenpox lasts around a week. Symptoms vary in severity but typically include a rash of small, itchy blisters that scab over, fever, fatigue, and headache.
However, in one out of every 4,000 chickenpox cases, the virus infects the brain, causing swelling. If the varicella-zoster virus makes it to the part of the brain that controls balance and muscle movements, it can cause a temporary loss of muscle control in the limbs that can last for months. Chickenpox can also cause other serious complications, including skin, lung, and blood infections.
Prior to the U.S.’ approval of the vaccine in 1995, children accounted for most of the country’s chickenpox cases, with over 10,000 U.S. children hospitalized with chickenpox each year.
The chickenpox vaccine is very effective and safe
Chickenpox is an extremely contagious disease. People without immunity have a 90 percent chance of contracting the virus if exposed.
Fortunately, the chickenpox vaccine provides lifetime protection and is around 90 percent effective against infection and nearly 100 percent effective against severe illness. It also reduces the risk of developing shingles later in life.
In addition to being incredibly effective, the chickenpox vaccine is very safe, and serious side effects are extremely rare. Some people may experience mild side effects after vaccination, such as pain at the injection site and a low fever.
Although infection provides immunity against future chickenpox infections, letting children catch chickenpox to build up immunity is never worth the risk, especially when a safe vaccine is available. The purpose of vaccination is to gain immunity without serious risk.
The chickenpox vaccine is one of the greatest vaccine success stories in history
It’s difficult to overstate the impact of the chickenpox vaccine. Within five years of the U.S. beginning universal vaccination against chickenpox, the disease had declined by over 80 percent in some regions.
Nearly 30 years after the introduction of the chickenpox vaccine, the disease is almost completely wiped out. Cases and hospitalizations have plummeted by 97 percent, and chickenpox deaths among people under 20 are essentially nonexistent.
Thanks to the vaccine, in less than a generation, a disease that once swept through schools and affected nearly every child has been nearly eliminated. And, unlike vaccines introduced in the early 20th century, no one can argue that improved hygiene, sanitation, and health helped reduce chickenpox cases beginning in the 1990s.
Having chickenpox as a child puts you at risk of shingles later
Although most people recover from chickenpox within a week or two, the virus that causes the disease, varicella-zoster, remains dormant in the body. This latent virus can reactivate years after the original infection as shingles, a tingling or burning rash that can cause severe pain and nerve damage.
One in 10 people who have chickenpox will develop shingles later in life. The risk increases as people get older as well as for those with weakened immune systems.
Getting chickenpox as an adult can be deadly
Although chickenpox is generally considered a childhood disease, it can affect unvaccinated people of any age. In fact, adult chickenpox is far deadlier than pediatric cases.
Serious complications like pneumonia and brain swelling are more common in adults than in children with chickenpox. One in 400 adults who get chickenpox develops pneumonia, and one to two out of 1,000 develop brain swelling.
Vaccines have virtually eliminated chickenpox, but outbreaks still happen
Although the chickenpox vaccine has dramatically reduced the impact of a once widespread disease, declining immunity could lead to future outbreaks. A Centers for Disease Control and Prevention analysis found that chickenpox vaccination rates dropped in half of U.S. states in the 2022-2023 school year compared to the previous year. And more than a dozen states have immunization rates below 90 percent.
In 2024, New York City and Florida had chickenpox outbreaks that primarily affected unvaccinated and under-vaccinated children. With declining public confidence in routine vaccines and rising school vaccine exemption rates, these types of outbreaks will likely become more common.
The CDC recommends that children receive two chickenpox vaccine doses before age 6. Older children and adults who are unvaccinated and have never had chickenpox should also receive two doses of the vaccine.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.

Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Bridging The Generation Gap Over The Holidays

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Often seen as a time for family connection, this same holiday period is often experienced as a time of family tension. But it doesn’t have to be that way!
Hopefully this will be of benefit to readers of all ages, but we’re going to write with the largest age-group of our readership, which is people who are most likely to have Gen-Z grandkids.
why are we writing about this?
Not only are health and happiness closely linked, and not only is mental health also just health, but… In terms of the healthy longevity secrets of the “Blue Zones”, strong intergenerational connections are usually a feature.
First, the obvious:
Any holiday tensions, of course, don’t usually start with grandkids, and are more likely amongst the adults, but some points of friction can be the same:
- Differences of opinion on political/social/economic issues
- Difference of opinion on parenting/dating choices
- Differences of opinion on life priorities
And yes, by the way, that includes even young teens (and perhaps younger) having opinions on these things—we are living in an information age, and this does mean a lot of information is a lot more accessible than it used to be, including for kids. Problems (at all ages) may occur when someone is only really exposed to views from within a certain “bias bubble”, but for better or worse, most people will have an opinion on most well-known things.
As a general rule of thumb, all of these differences of opinion can be shelved if (and only if) those involved seek to avoid conflict. And while age is no guarantee of maturity, often it’ll be the older person(s) in the strongest position to redirect things. So, have a stack of “safe” topics up your sleeve.
Bonus: you can also have non-conversational distractions up your sleeve! These may be kitchen-related, for example (time to produce something distracting, or if the nascent conflict was only between you and one other person, time to go check on something, thus removing yourself from the situation).
Next, about “family time” and technology
It can be tempting to try to have a “phones away” rule, but this will tend to only exacerbate a younger person’s withdrawal.
Better: ask (with a tone of cheerful curiosity, not accusation) about what captures their attention so. Ask about their favorite YouTubers or TikTokers or whatever it is that it is for them. Learn about that Subreddit.
Or maybe (more likely for Millennials) they were following what is going on in the world via social media, which takes on an intermediary role for the delivery of world news. Hopefully this won’t run into the differences of opinion that we mentioned up top, but it could also be a perfectly good avenue of conversation, and maybe there’s more common ground than you might expect.
Meanwhile, if you’re the older generation present, chances are your own social media use is more about the human element. That’s great, but watch out:
A common faux pas is taking pictures without asking, let alone posting them online without asking. For many people this may seem an odd thing to object to, but generationally speaking, the younger someone is (down to the upper single digits, anyway) the more likely they might feel strongly about this. So, ask first.
The reason, by the way, is that in this age of digital hypervisibility, what we choose to share online can be a deeply personal thing. And, say what you will about the pros or cons of someone carefully curating an image of how they wish to be seen, shortcutting through that for them with a candid photo posted on Facebook will not endear you to them, even if you can’t see anything wrong with the photo in question, for example.
See also: Make Social Media Work For Your Mental Health
Show an interest, but don’t interrogate
This one doesn’t take too much explanation. If people want to share about their lives, they’ll need only the smallest nudge to do so. If someone passes up an opportunity to talk about something you showed an interest in, chances are they have their own reasons for not wanting to talk about it. This might be hurtful if you feel like they’re keeping you out of their life, but the best way to get them to talk to you is just to be a good listener—not an interrogator that they have to dodge.
For some powerful tools on this, see: Listening, Better
Lastly, if things aren’t so good…
43% of people are currently experiencing some sort of familial estrangement, so if that’s you, you’re not on your own.
Sometimes, it really is too late to fix things, but sometimes it isn’t; we put together a guide that might help:
Family Estrangement & How To Fix It
Take care!
Share This Post
-

HRT: Bioidentical vs Animal
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
HRT: A Tale Of Two Approaches
In yesterday’s newsletter, we asked you for your assessment of menopausal hormone replacement therapy (HRT).
- A little over a third said “It can be medically beneficial, but has some minor drawbacks”
- A little under a third said “It helps, but at the cost of increased cancer risk; not worth it”
- Almost as many said “It’s a wondrous cure-all that makes you happier, healthier, and smell nice too”
- Four said “It is a dangerous scam and a sham; “au naturel” is the way to go”
So what does the science say?
Which HRT?
One subscriber who voted for “It’s a wondrous cure-all that makes you healthier, happier, and smell nice too” wrote to add:
❝My answer is based on biodentical hormone replacement therapy. Your survey did not specify.❞
And that’s an important distinction! We did indeed mean bioidentical HRT, because, being completely honest here, this European writer had no idea that Premarin etc were still in such wide circulation in the US.
So to quickly clear up any confusion:
- Bioidentical hormones: these are (as the name suggests) identical on a molecular level to the kind produced by humans.
- Conjugated Equine Estrogens: such as Premarin, come from animals. Indeed, the name “Premarin” comes from “pregnant mare urine”, the substance used to make it.
There are also hormone analogs, such as medroxyprogesterone acetate, which is a progestin and not the same thing as progesterone. Hormone analogs such as the aforementioned MPA are again, a predominantly-American thing—though they did test it first in third-world countries, after testing it on animals and finding it gave them various kinds of cancer (breast, cervical, ovarian, uterine).
A quick jumping-off point if you’re interested in that:
Depot medroxyprogesterone acetate and the risk of breast and gynecologic cancer
this is about its use as a contraceptive (so, much lower doses needed), but it is the same thing sometimes given in the US as part of menopausal HRT. You will note that the date on that research is 1996; DMPA is not exactly cutting-edge and was first widely used in the 1950s.
Similarly, CEEs (like Premarin) have been used since the 1930s, while estradiol (bioidentical estrogen) has been in use since the 1970s.
In short: we recommend being wary of those older kinds and mostly won’t be talking about them here.
Bioidentical hormones are safer: True or False?
True! This is an open-and-shut case:
❝Physiological data and clinical outcomes demonstrate that bioidentical hormones are associated with lower risks, including the risk of breast cancer and cardiovascular disease, and are more efficacious than their synthetic and animal-derived counterparts.
Until evidence is found to the contrary, bioidentical hormones remain the preferred method of HRT. ❞
Further research since that review has further backed up its findings.
Source: Are Bioidentical Hormones Safer or More Efficacious than Other Commonly Used Versions in HRT?
So simply, if you’re going on HRT (estrogen and/or progesterone), you might want to check it’s the bioidentical kind.
HRT can increase the risk of breast cancer: True or False?
Contingently True, but for most people, there is no significant increase in risk.
First: again, we’re talking bioidentical hormones, and in this case, estradiol. Older animal-derived attempts had much higher risks with much lesser efficaciousness.
There have been so many studies on this (alas, none that have been publicised enough to undo the bad PR in the wake of old-fashioned HRT from before the 70s), but here’s a systematic review that highlights some very important things:
❝Estradiol-only therapy carries no risk for breast cancer, while the breast cancer risk varies according to the type of progestogen.
Estradiol therapy combined with medroxyprogesterone, norethisterone and levonorgestrel related to an increased risk of breast cancer, estradiol therapy combined with dydrogesterone and progesterone carries no risk❞
In fewer words:
- Estradiol by itself: no increased risk of breast cancer
- Estradiol with MDPA or other progestogens that aren’t really progesterone: increased risk of breast cancer
- Estradiol with actual progesterone: back to no increased risk of breast cancer
So again, you might want to make sure you are getting actual bioidentical hormones, and not something else!
However! If you are aware that you already have an increased risk of breast cancer (e.g. family history, you’ve had it before, you know you have certain genes for it, etc), then you should certainly discuss that with your doctor, because your personal circumstances may be different:
❝Tailored HRT may be used without strong evidence of a deleterious effect after ovarian cancer, endometrial cancer, most other gynecological cancers, bowel cancer, melanoma, a family history of breast cancer, benign breast disease, in carriers of BRACA mutations, after breast cancer if adjuvant therapy is not being used, past thromboembolism, varicose veins, fibroids and past endometriosis.
Relative contraindications are existing cardiovascular and cerebrovascular disease and breast cancer being treated with adjuvant therapies❞
Source: HRT in difficult circumstances: are there any absolute contraindications?
HRT makes you happier, healthier, and smell nice too: True or False?
Contingently True, assuming you do want its effects, which generally means the restoration of much of the youthful vitality you enjoyed pre-menopause.
The “and smell nice too” was partly rhetorical, but also partly literal: our scent is largely informed by our hormones, and higher estrogen results in a sweeter scent; lower estrogen results in a more bitter scent. Not generally considered an important health matter, but it’s a thing, so hey.
More often, people take menopausal HRT for more energy, stronger bones (reduced osteoporosis risk), healthier heart (reduced CVD risk), improved sexual health, better mood, healthier skin and hair, and general avoidance of menopause symptoms:
Read more: Skin, hair and beyond: the impact of menopause
We’d need another whole main feature to discuss all the benefits properly; today we’re just mythbusting.
HRT does have some drawbacks: True or False?
True, and/but how serious they are (beyond the aforementioned consideration in the case of an already-increased risk of breast cancer) is a matter of opinion.
For example, it is common to get a reprise of monthly cramps and/or mood swings, depending on how one is taking the HRT and other factors (e.g. your own personal physiology and genetic predispositions). For most people, these will even out over time.
It’s also even common to get a reprise of (much slighter than before) monthly bleeding, unless you have for example had a hysterectomy (no uterus = no bleeding). Again, this will usually settle down in a matter of months.
If you experience anything more alarming than that, then indeed check with your doctor.
HRT is a dangerous scam and sham: True or False?
False, simply. As described above, for most people they’re quite safe. Again, talking bioidentical hormones.
The other kind are in the most neutral sense a sham (i.e. they are literally sham hormones), though they’re not without their merits and for many people they may be better than nothing.
As for being a scam, biodentical hormones are widely prescribed in the many countries that have universal healthcare and/or a single-payer healthcare system, where there would be no profit motive (and considerable cost) in doing so.
They’re prescribed because they are effective and thus reduce healthcare spending in other areas (such as treating osteoporosis or CVD after the fact) and improve Health Related Quality of Life, and by extension, health-adjusted life-years, which is one of the top-used metrics for such systems.
See for example:
Our apologies, gentlemen
We wanted to also talk about testosterone therapy for the andropause, but we’ve run out of room today (because of covering the important distinction of bioidentical vs old-fashioned HRT)!
To make it up to you, we’ll do a full main feature on it (it’s an interesting topic) in the near future, so watch this space
Ladies, we’ll also at some point cover the pros and cons of different means of administration, e.g. pills, transdermal gel, injections, patches, pessaries, etc—which often have big differences.
That’ll be in a while though, because we try to vary our topics, so we can’t talk about menopausal HRT all the time, fascinating and important a topic it is.
Meanwhile… take care, all!
Share This Post
-

Under Pressure: A Guide To Controlling High Blood Pressure – by Dr. Frita Fisher
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hypertension kills a lot of people, and does so with little warning—it can be asymptomatic before it gets severe enough to cause harm, and once it causes harm, well, one heart attack or stroke is already one too many.
Aimed more squarely at people in the 35–45 danger zone (young enough to not be getting regular blood pressure checks, old enough that it may have been building up for decades), this is a very good primer on blood pressure, factors affecting it, what goes wrong, what to do about it, and how to make a good strategy for managing it for life.
The style is easy-reading, making this short (91 pages) book a very quick read, but an informative one.
Bottom line: if you are already quite knowledgeable about blood pressure and blood pressure management, this one’s probably not for you. But if you’re in the category of “what do those numbers mean again?”, then this is a very handy book to have, to get you up to speed so that you can handle things as appropriate.
Click here to check out Under Pressure, and get/keep yours under control!
Share This Post
Related Posts
-
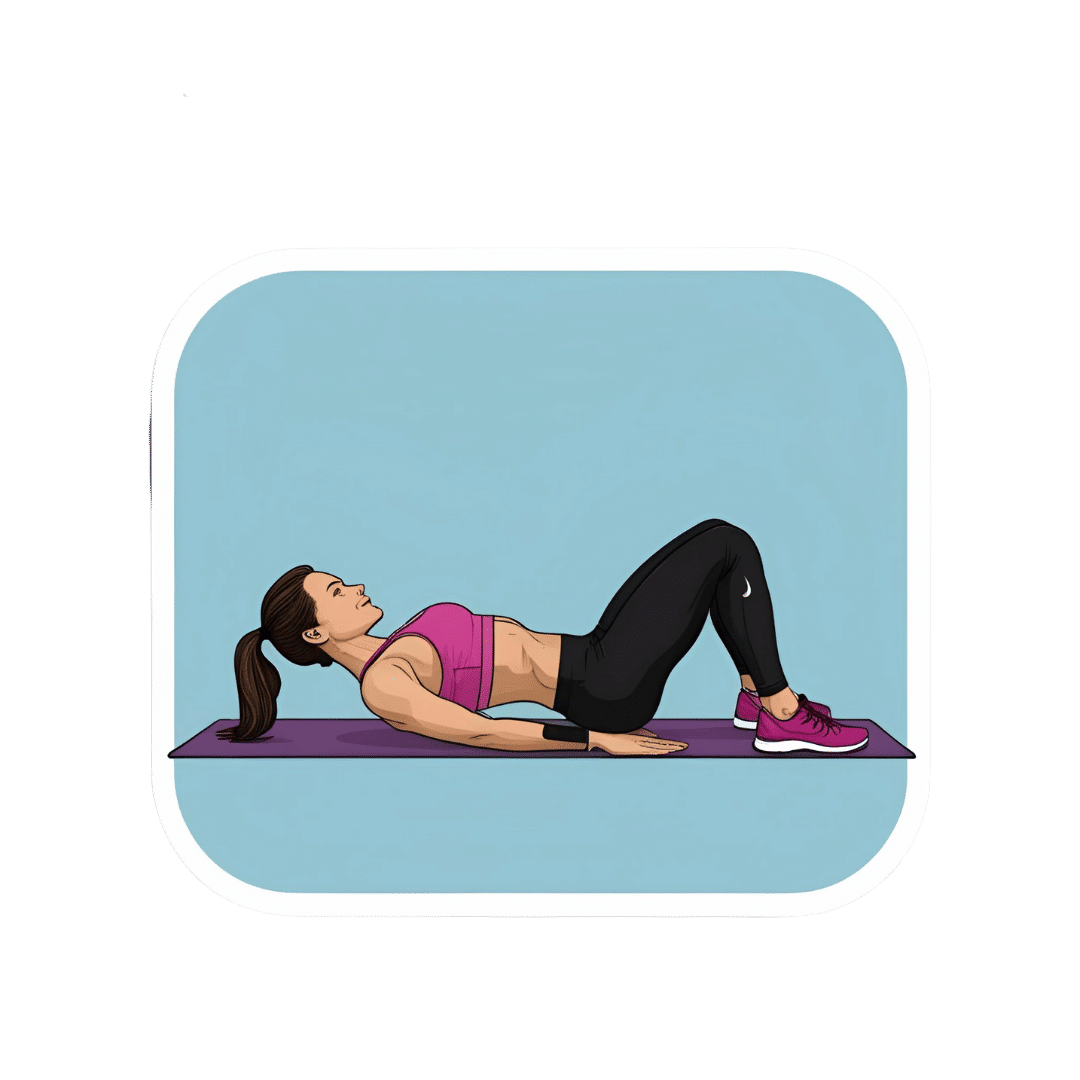
What Happens To Your Body When You Do 100 Glute Bridges Every Day
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Not just for a sculpted butt:
Benefits
With consistent daily glute bridge practice, you may expect:
- Rounder, toned butt: targets the gluteus maximus, toning and lifting the butt for a rounder appearance.
- Improved posture: strengthens glutes to support the spine and pelvis, alleviating lower back and hip pain. Stretches tight hip flexors from prolonged sitting.
- Stronger lower back: glutes support the lower back and spine, reducing pain and making it easier to lift heavy objects. Activating the glutes transfers force from legs to core, preventing injuries.
- Stronger knees: stabilizes the knee joint and promotes alignment by engaging glutes, hamstrings, and quadriceps, reducing knee pain.
- Sculpted hamstrings: contracts hamstrings during lifts for strength, while stretching them on the way down increases flexibility.
- Increased hip flexibility: strengthens muscles around the hip joint, improving mobility and counteracting tight hips from sedentary habits.
- Reduced back pain: strengthens glutes to correct pelvic tilt and reduce strain on the lower back.
- Faster running speed: improves hip extension, strengthens hamstrings, and activates the gluteus medius for better running power and balance.
- Enhanced strength training performance: strengthens glutes, back, and knees, improving performance in exercises like squats and deadlifts.
As for how to get going, the video offers the following very sound advice: begin with 25–30 reps per session and gradually increase to sets of 100 daily. It should take about 5 minutes (that’s 3 seconds per repetition). Results can be seen in as little as 2 weeks, with significant changes after a month of consistent practice.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Strong Curves: A Woman’s Guide to Building a Better Butt and Body – by Bret Contreras & Kellie Davis
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
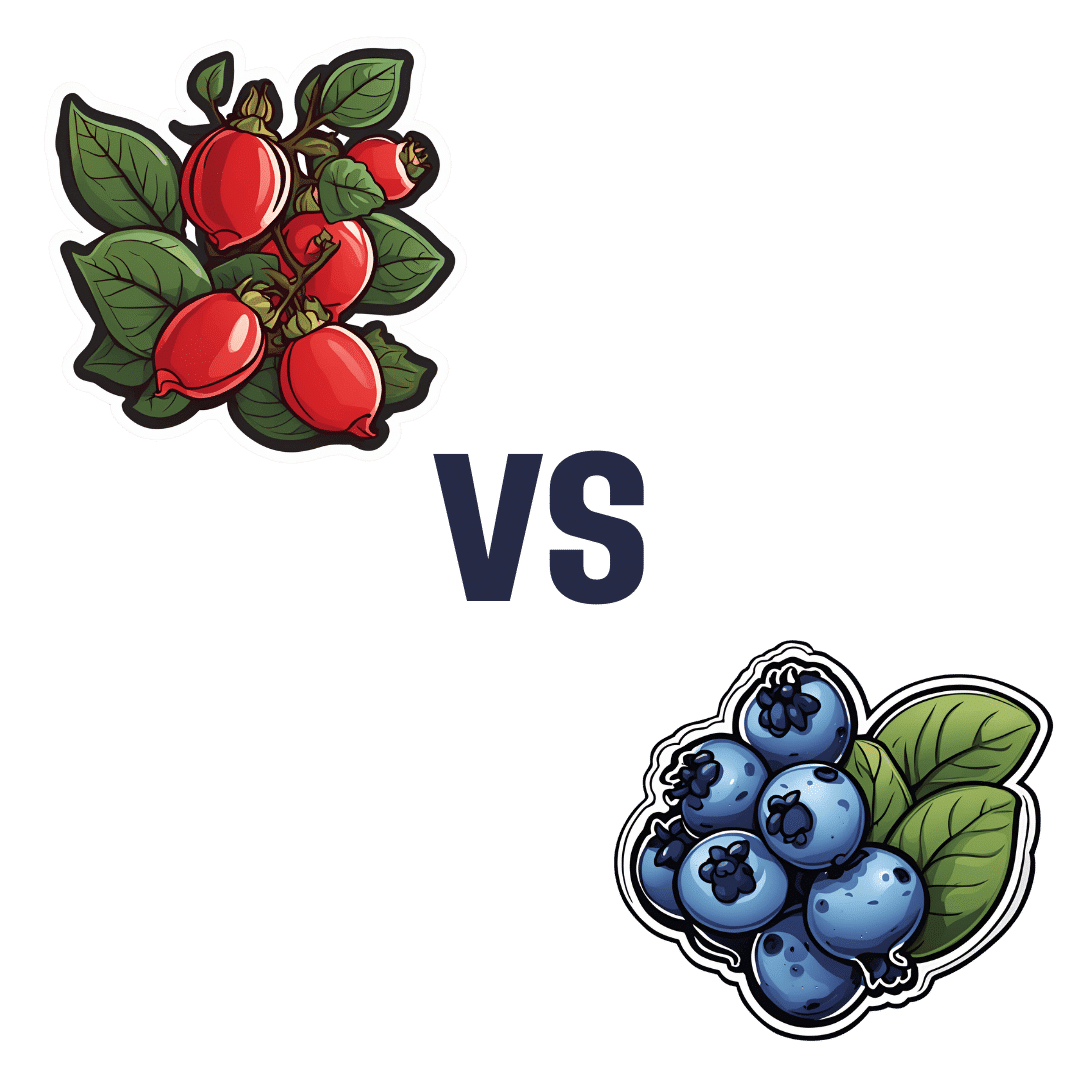
Rose Hips vs Blueberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing rose hips to blueberries, we picked the rose hips.
Why?
Both of these fruits are abundant sources of antioxidants and other polyphenols, but one of them stands out for overall nutritional density:
In terms of macros, rose hips have about 2x the carbohydrates, and/but about 10x the fiber. That’s an easy calculation and a clear win for rose hips.
When it comes to vitamins, rose hips have a lot more of vitamins A, B2, B3, B5, B6, C, E, K, and choline. On the other hand, blueberries boast more of vitamins B1 and B9. That’s a 9:2 lead for rose hips, even before we consider rose hips’ much greater margins of difference (kicking off with 80x the vitamin A, for instance, and many multiples of many of the others).
In the category of minerals, rose hips have a lot more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, and zinc. Meanwhile, blueberries are not higher in any minerals.
In short: as ever, enjoy both, but if you’re looking for nutritional density, there’s a clear winner here and it’s rose hips.
Want to learn more?
You might like to read:
It’s In The Hips: Rosehip’s Benefits, Inside & Out
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Falling vaccination rates put children at risk of preventable diseases. Governments need a new strategy to boost uptake
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Child vaccination is one of the most cost-effective health interventions. It accounts for 40% of the global reduction in infant deaths since 1974 and has led to big health gains in Australia over the past two decades.
Australia has been a vaccination success story. Ten years after we begun mass vaccination against polio in 1956, it was virtually eliminated. Our child vaccination rates have been among the best in the world.
But after peaking in 2020, child vaccination in Australia is falling. Governments need to implement a comprehensive strategy to boost vaccine uptake, or risk exposing more children to potentially preventable infectious diseases.
Yuri A/Shutterstock Child vaccination has been a triumph
Thirty years ago, Australia’s childhood vaccination rates were dismal. Then, in 1997, governments introduced the National Immunisation Program to vaccinate children against diseases such as diphtheria, tetanus, and measles.
Measures to increase coverage included financial incentives for parents and doctors, a public awareness campaign, and collecting and sharing local data to encourage the least-vaccinated regions to catch up with the rest of the country.
What followed was a public health triumph. In 1995, only 52% of one-year-olds were fully immunised. By 2020, Australia had reached 95% coverage for one-year-olds and five-year-olds. At this level, it’s difficult even for highly infectious diseases, such as measles, to spread in the community, protecting both the vaccinated and unvaccinated.
By 2020, 95% of children were vaccinated. Drazen Zigic/Shutterstock Gaps between regions and communities closed too. In 1999, the Northern Territory’s vaccination rate for one-year-olds was the lowest in the country, lagging the national average by six percentage points. By 2020, that gap had virtually disappeared.
The difference between vaccination rates for First Nations children and other children also narrowed considerably.
It made children healthier. The years of healthy life lost due to vaccine-preventable diseases for children aged four and younger fell by nearly 40% in the decade to 2015.
Some diseases have even been eliminated in Australia.
Our success is slipping away
But that success is at risk. Since 2020, the share of children who are fully vaccinated has fallen every year. For every child vaccine on the National Immunisation Schedule, protection was lower in 2024 than in 2020.
Gaps between parts of Australia are opening back up. Vaccination rates in the highest-coverage parts of Australia are largely stable, but they are falling quickly in areas with lower vaccination.
In 2018, there were only ten communities where more than 10% of one-year-old children were not fully vaccinated. Last year, that number ballooned to 50 communities. That leaves more areas vulnerable to disease and outbreaks.
While Noosa, the Gold Coast Hinterland and Richmond Valley (near Byron Bay) have persistently had some of the country’s lowest vaccination rates, areas such as Manjimup in Western Australia and Tasmania’s South East Coast have recorded big declines since 2018.
Missing out on vaccination isn’t just a problem for children.
One preprint study (which is yet to be peer-reviewed) suggests vaccination during pregnancy may also be declining.
Far too many older Australians are missing out on recommended vaccinations for flu, COVID, pneumococcal and shingles. Vaccination rates in aged care homes for flu and COVID are worryingly low.
What’s going wrong?
Australia isn’t alone. Since the pandemic, child vaccination rates have fallen in many high-income countries, including New Zealand, the United Kingdom and the United States.
Globally, in 2023, measles cases rose by 20%, and just this year, a measles outbreak in rural Texas has put at least 13 children in hospital.
Alarmingly, some regions in Australia have lower measles vaccination than that Texas county.
The timing of trends here and overseas suggests things shifted, or at least accelerated, during the pandemic. Vaccine hesitancy, fuelled by misinformation about COVID vaccines, is a growing threat.
This year, vaccine sceptic Robert F. Kennedy Jr was appointed to run the US health system, and Louisiana’s top health official has reportedly cancelled the promotion of mass vaccination.
In Australia, a recent survey found 6% of parents didn’t think vaccines were safe, and 5% believed they don’t work.
Those concerns are far more common among parents with children who are partially vaccinated or unvaccinated. Among the 2% of parents whose children are unvaccinated, almost half believe vaccines are not safe for their child, and four in ten believe vaccines didn’t work.
Other consequences of the pandemic were a spike in the cost of living, and a health system struggling to meet demand. More than one in ten parents said cost and difficulty getting an appointment were barriers to vaccinating their children.
There’s no single cause of sliding vaccination rates, so there’s no one solution. The best way to reverse these worrying trends is to work on all the key barriers at once – from a lack of awareness, to inconvenience, to lack of trust.
What governments should do
Governments should step up public health campaigns that counter misinformation, boost awareness of immunisation and its benefits, and communicate effectively to low-vaccination groups. The new Australian Centre for Disease Control should lead the charge.
Primary health networks, the regional bodies responsible for improving primary care, should share data on vaccination rates with GPs and pharmacies. These networks should also help make services more accessible to communities who are missing out, such as migrant groups and disadvantaged families.
State and local governments should do the same, sharing data and providing support to make maternal child health services and school-based vaccination programs accessible for all families.
Governments can communicate better about the benefits of vaccination. Yuri A/Shutterstock Governments should also be more ambitious about tackling the growing vaccine divides between different parts of the country. The relevant performance measure in the national vaccination agreement is weak. States must only increase five-year-old vaccination rates in four of the ten areas where it is lowest. That only covers a small fraction of low-vaccination areas, and only the final stage of child vaccination.
Australia needs to set tougher goals, and back them with funding.
Governments should fund tailored interventions in areas with the lowest rates of vaccination. Proven initiatives include training trusted community members as “community champions” to promote vaccinations, and pop-up clinics or home visits for free vaccinations.
At this time of year, childcare centres and schools are back in full swing. But every year, each new intake has less protection than the previous cohort. Governments are developing a new national vaccination strategy and must seize the opportunity to turn that trend around. If it commits to a bold national plan, Australia can get back to setting records for child vaccination.
Peter Breadon, Program Director, Health and Aged Care, Grattan Institute and Wendy Hu, Associate, Health Program, Grattan Institute
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: